Pregnancy is a complex state in a woman's life. It is associated with anatomical and physiologic changes that greatly affect not only the mother but the living fetus inside her womb. This is a case of a 22-year-old woman at 36 5/7 weeks age of gestation presented with intractable tachycardia. The patient presented at the emergency room in cardiorespiratory distress in conjunction with preterm labor. The dilemma of the management would be thoroughly discussed in consideration of the present maternal cardiac condition and pregnancy.
Maternal cardiac disease, Heart disease in pregnancy, Electro cardioversion
Cardiovascular alterations during pregnancy are characterized by an increased vascular volume, cardiac output, and heart rate, with a marked fall in vascular resistance. Cardiac output is about 40-50% higher during the third trimester. Given the physiologic changes, pregnancy predisposes a woman to cardiovascular situations that could affect maternal and fetal well-being. On the other hand, there are individuals who have known cardiac lesions or a history of cardiovascular disease that precipitates cardiac complications.
Supraventricular tachycardia in pregnancy imposes a serious threat to the mother and fetus. The incidence of paroxysmal supraventricular tachycardia in the general population is 35 cases per 100,000 population per year, with a prevalence of 2.25 cases per 1,000 population. The proposed mechanisms in developing supraventricular tachycardia in gravidas include hyperdynamic circulation, altered hormonal milieu, increased circulating levels of catecholamines, increased adrenergic receptor sensitivity, and increased maternal effective circulating volume causing atrial stretch [1]. The most common presentation is palpitations. In more than 50% of pregnant women investigated for palpitations, ectopic beats, and non-sustained arrhythmias were recorded while sustained tachycardias account to 2-3 per 1,000 cases [2]. These cases can be managed effectively with conservative management in the forms of medical cardioversion or electro-cardioversion. Management is individualized and depends on the response of the heart to treatment modalities. This case focuses on the successful management of supraventricular tachycardia in pregnancy that resulted to a safe vaginal delivery.
To discuss a case of supraventricular tachycardia in pregnancy and its management.
1. To discuss the cardiovascular adaptations to pregnancy.
2. To discuss supraventricular tachycardia in pregnancy.
3. To discuss the management of supraventricular tachycardia in pregnancy.
This is the first documented article to feature the management of supraventricular tachycardia during pregnancy in the Philippines. This will help future cases in the immediate management of intractable supraventricular tachycardia among gravidas as it presents the dilemmas on the management of the case.
This is a case of B.O. a 22-year-old G3P1 (1011) who came in as a referral from another obstetrician because of tachycardia. She had a past history of cardiac disease in her last pregnancy in 2014 but the main pathology was unknown. There was no history of hereditary illnesses in the family. She is a non-smoker and non-alcoholic beverage drinker. She had her menarche at 11-years-old with menses occurring at regular intervals, lasting for 3-4 days consuming 3 moderately soaked pads per day. Her first sexual contact was at 16-years-old with one monogamous sexual partner. There was no history of contraceptive pill use. She is a Gravida 3 Para 1 (1011). Her first pregnancy was a molar pregnancy for which she underwent suction curettage. Her second pregnancy was delivered by spontaneous vaginal delivery which was complicated by cardiac dysrhythmia secondary to an unknown structural cardiac disease. Her last menses was on October 29, 2019 giving her an amenorrhea of 36 weeks and 5 days.
History of present illness started at 28 weeks of pregnancy when she started to experience dyspnea on exertion and 2-pillow orthopnea. She had prenatal check up with a private obstetrician and was advised to see a cardiologist but failed to do so because of financial constraints.
Few hours prior to admission, patient consulted her obstetrician because of labor pains. She was assessed to be tachycardic and was referred to our institution. At the emergency room, patient was ambulatory but in cardiorespiratory distress. There was no appreciable blood pressure. She was tachycardic at 182 beats per minute with a respiratory rate at 26 cycles per minute and oxygen saturation of 98%. She was immediately brought to the resuscitation area. Oxygen at 4 LPM was given thru nasal cannula. Carotid massage was done (Figure 1). ECG was done which revealed supraventricular tachycardia with narrow QRS complexes on chest leads V1-V6 (Figure 2).
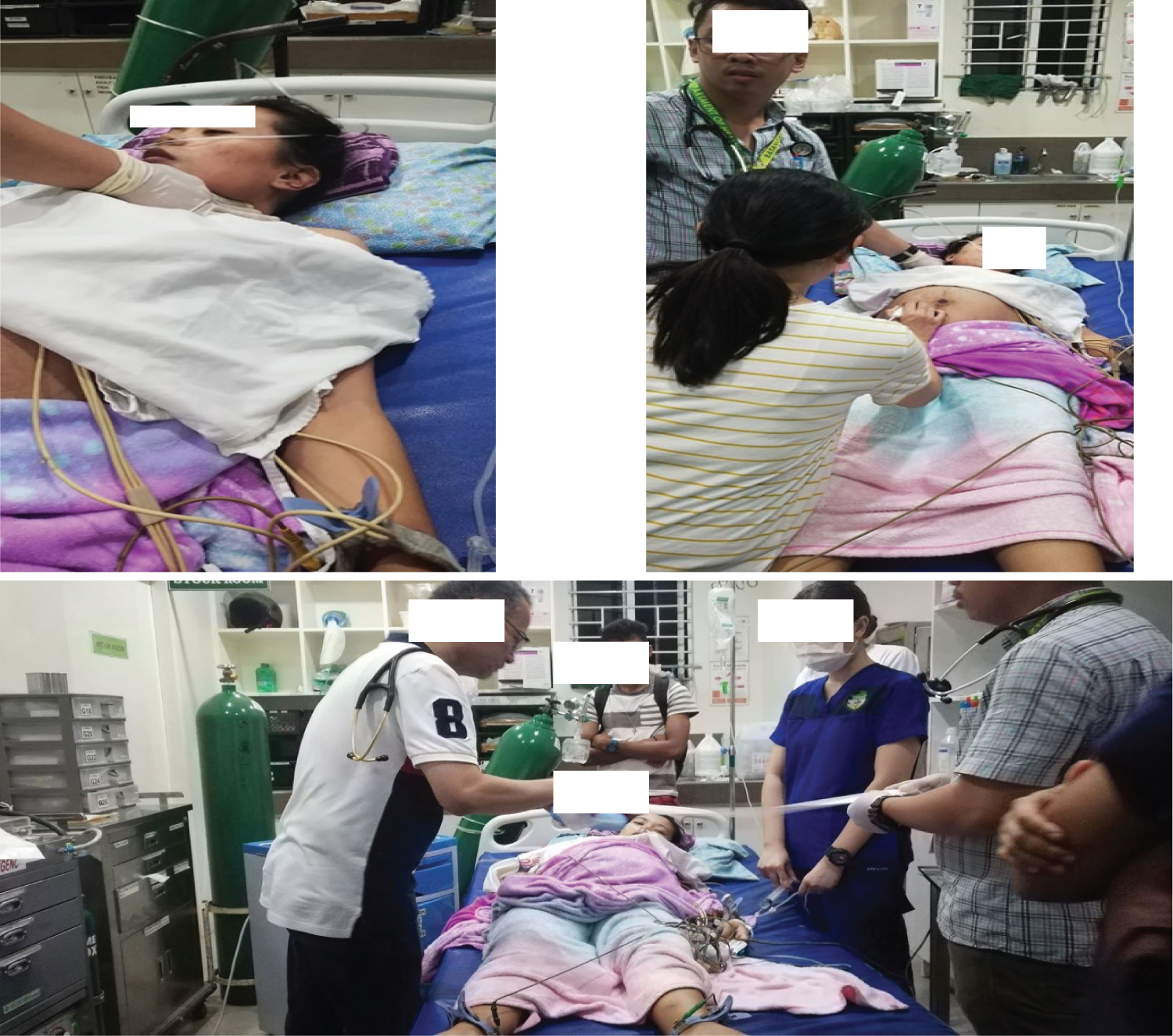 Figure 1: Patient stabilized with vagal stimulation. The fetal heart rate was monitored and there was no noted fetal bradycardia during cardiac resuscitation.
View Figure 1
Figure 1: Patient stabilized with vagal stimulation. The fetal heart rate was monitored and there was no noted fetal bradycardia during cardiac resuscitation.
View Figure 1
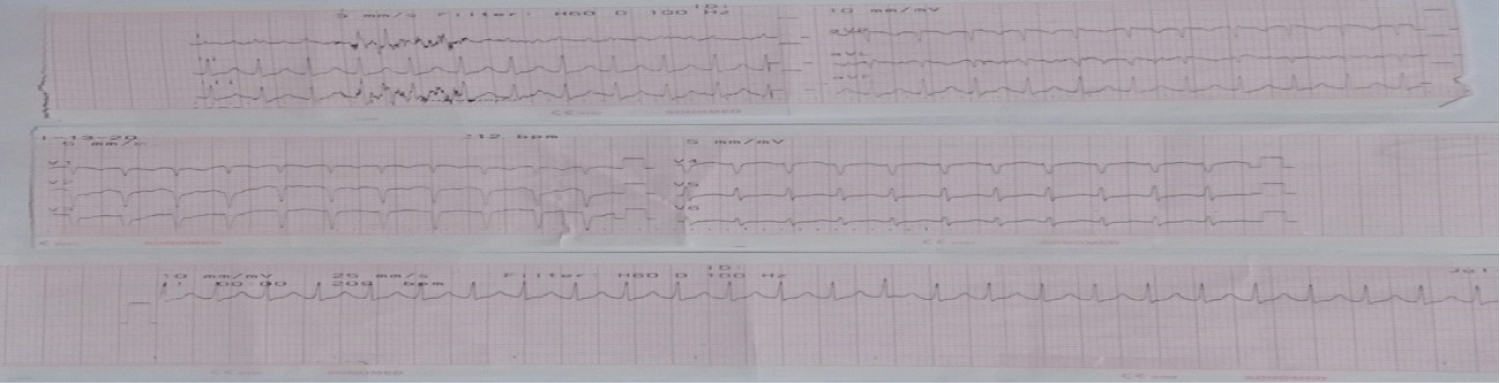 Figure 2: Initial ECG shows supraventricular tachycardia with narrow QRS complexes on chest leads V1-V6.
View Figure 2
Figure 2: Initial ECG shows supraventricular tachycardia with narrow QRS complexes on chest leads V1-V6.
View Figure 2
The case was immediately referred to the service consultant, cardiologist and perinatologist. Patient was pale. Her neck veins were not distended. She had a dynamic precordium with apex beat at left 6th intercostal space without murmurs. She had clear breath sounds. On abdominal examination, the fundic height was 28 cms with an estimated fetal weight of 2635g. The fetal heart tone was 143 beats per minute at the left lower quadrant. On internal examination, cervix was 1 cm dilated, beginning effacement with intact bag of water, cephalic at station -2, no blood per examining finger.
The admitting diagnosis was G3P1 (1011) Pregnancy uterine 36 5/7 weeks Age of Gestation, Cephalic in preterm labor Gravidocardiac NYHA Functional Class IV. Upon rechecking the vital signs, the blood pressure was still not appreciated and tachycardia increased to 210 beats per minute. The case was referred to IM Cardiology and two management options were discussed: 1) To manage this case medically or 2) To give series of electrocardioversions. Medical management was deemed not feasible because blood pressure was not appreciated. The plan was to stabilize the mother then do vaginal delivery once the patient is stable. Vagal stimulation continued. Cardioversion was initiated at 50 joules under intravenous sedation of Midazolam 5 mg. Post-cardioversion, the vital signs were as follows: BP 100/70 with a heart rate of 192 beats/min. Electrocardiography showed supraventricular tachycardia with widened QRS complexes on chest leads V1-V6 (Figure 3).
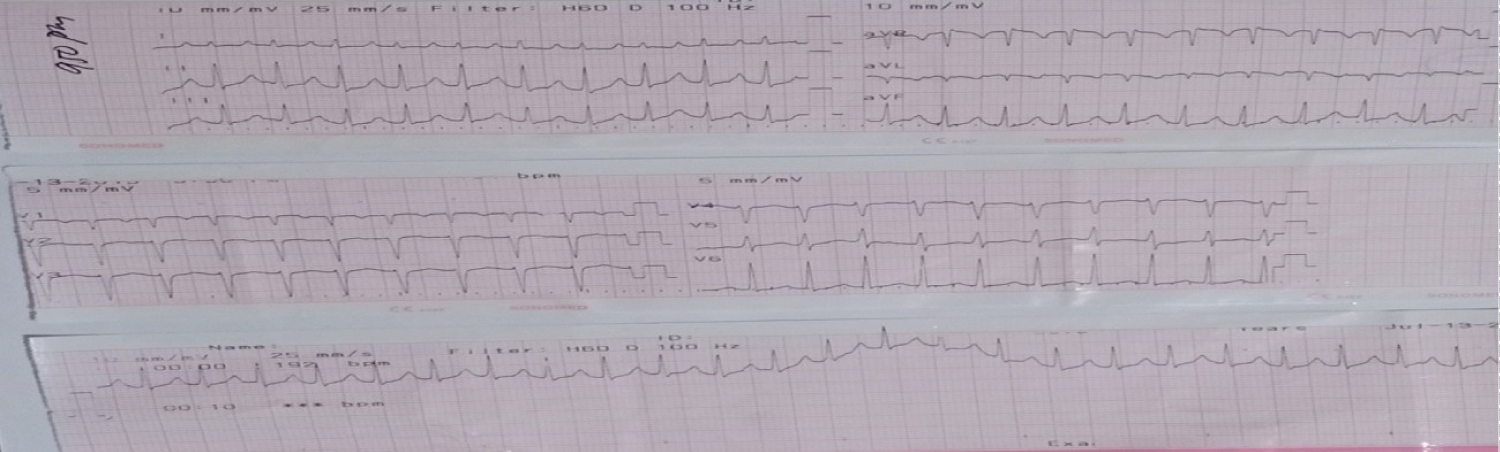 Figure 3: ECG shows supraventricular tachycardia after cardioversion of 50 joules.
View Figure 3
Figure 3: ECG shows supraventricular tachycardia after cardioversion of 50 joules.
View Figure 3
In the presence of a normal blood pressure, medical management was initiated using Adenosine 6 mg intavenously. After two doses of adenosine, supraventricular tachycardia was still noted at 215 bpm (Figure 4). Electrocardioversion was done again twice at 100 joules and 200 joules for persistent supraventricular tachycardia of 203 bpm (Figure 5) and 200 bpm (Figure 6) respectively. The cardiologist then decided to give Verapamil 5 mg intravenously but still tachycardic at 222 bpm (Figure 7). However, hypotension at palpatory 70 was noted. Digoxin 0.5 mg was then given intravenously and still tachycardic at 203 bpm and noted atrial fibrillation (Figure 8). Another cardioversion was given at 200 joules but still tachycardic at 192 bpm (Figure 9). The decision to further stabilize and monitor the patient and the baby in the labor room was then made. The cardiac rate prior to transfer to the obstetrical complex was 189 bpm. The following medications were then started: Lanoxin 0.5 mg IV then 0.25 mg every 6 hours for 4 doses; Midazolam single dose and Amniodarone 150 mg + 10 cc of D5LR then 300 mg in 100 cc of D5W to run for 4 hours for 6 cycles. Vital signs at the labor room were as follows: BP 100/70, CR 183/min, RR 29/min with oxygen saturation of 98%. Cardiotocography was done which revealed a Category I tracing (Figure 10). The mother and the baby were continuously monitored. She was hooked to a cardiac monitor and continuous fetal heart rate monitoring.
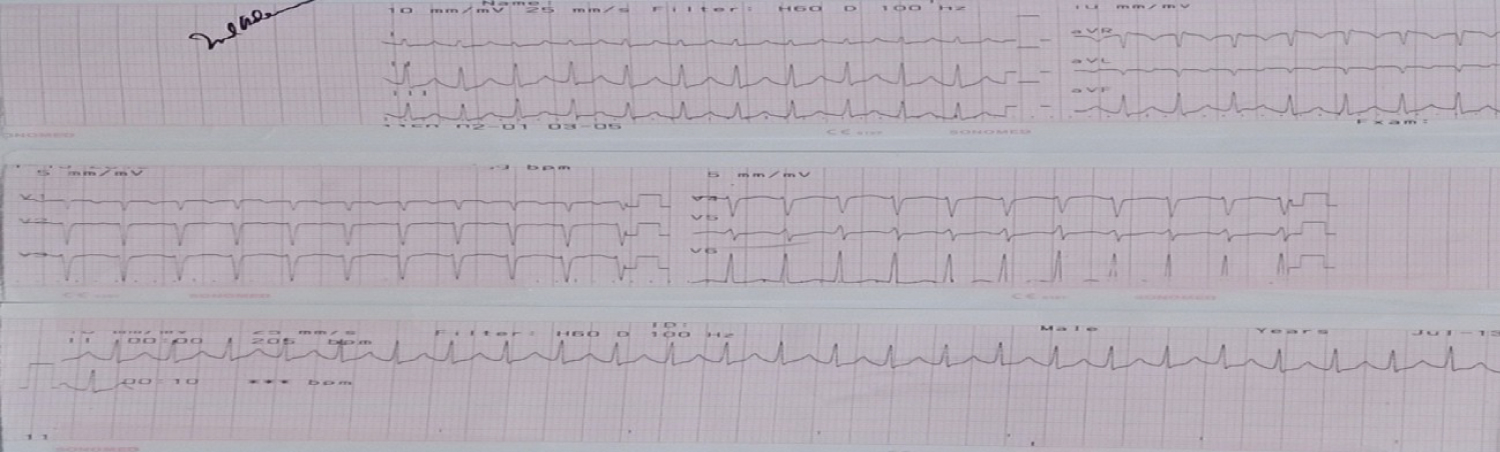 Figure 4: ECG shows supraventricular tachycardia post-administration of adenosine.
View Figure 4
Figure 4: ECG shows supraventricular tachycardia post-administration of adenosine.
View Figure 4
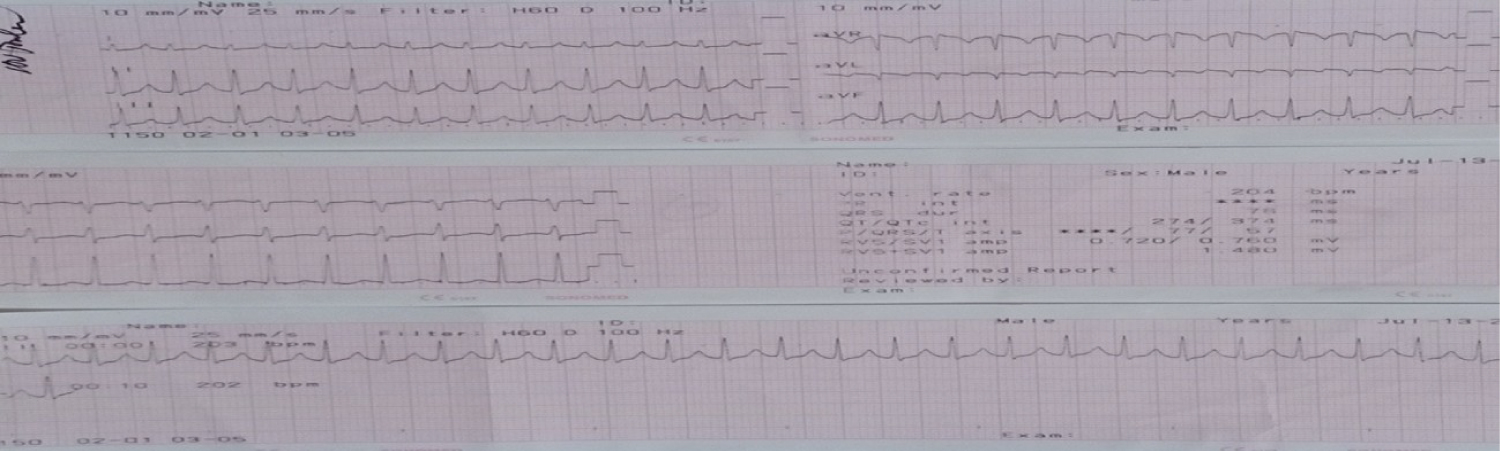 Figure 5: ECG shows supraventricular tachycardia after cardioversion with 100 Joules.
View Figure 5
Figure 5: ECG shows supraventricular tachycardia after cardioversion with 100 Joules.
View Figure 5
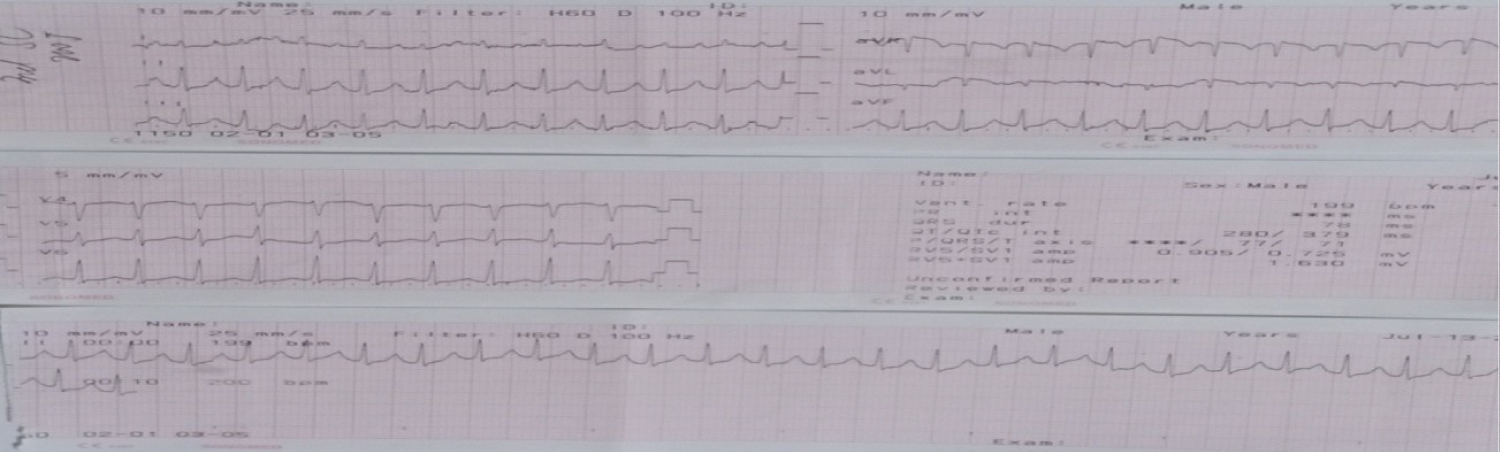 Figure 6: ECG shows supraventricular tachycardia after cardioversion of 200 Joules.
View Figure 6
Figure 6: ECG shows supraventricular tachycardia after cardioversion of 200 Joules.
View Figure 6
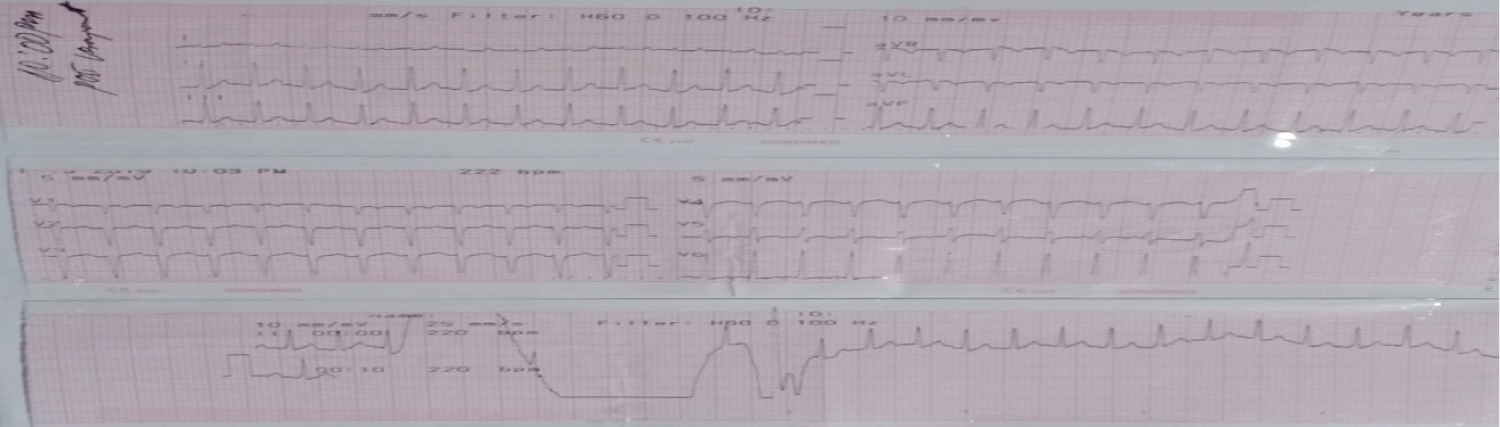 Figure 7: ECG shows supraventricular tachycardia after administration of Verapamil.
View Figure 7
Figure 7: ECG shows supraventricular tachycardia after administration of Verapamil.
View Figure 7
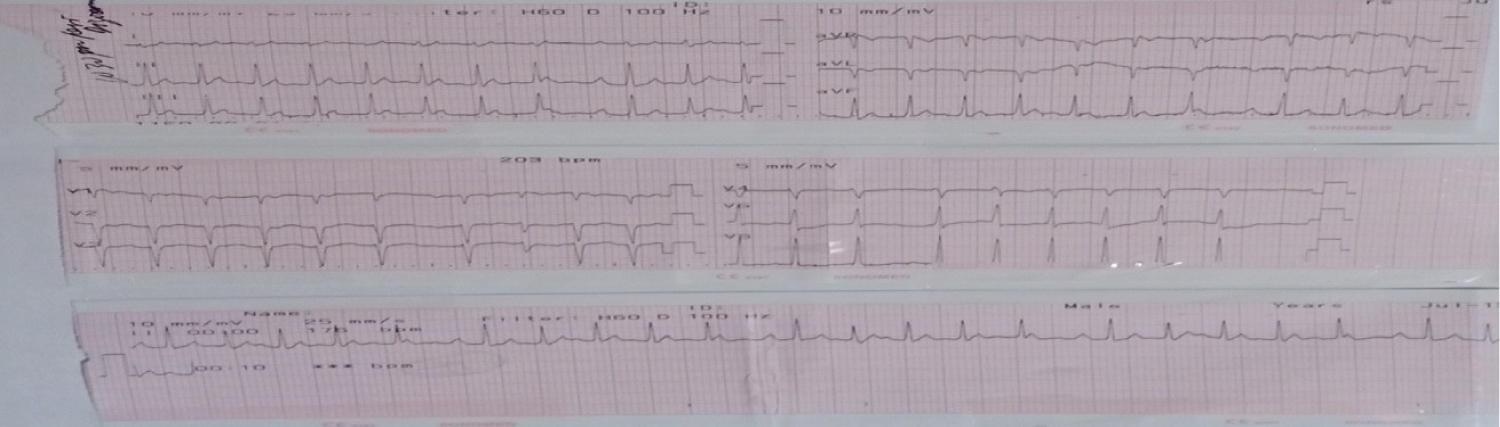 Figure 8: ECG shows atrial fibrillation post administration of Digoxin.
View Figure 8
Figure 8: ECG shows atrial fibrillation post administration of Digoxin.
View Figure 8
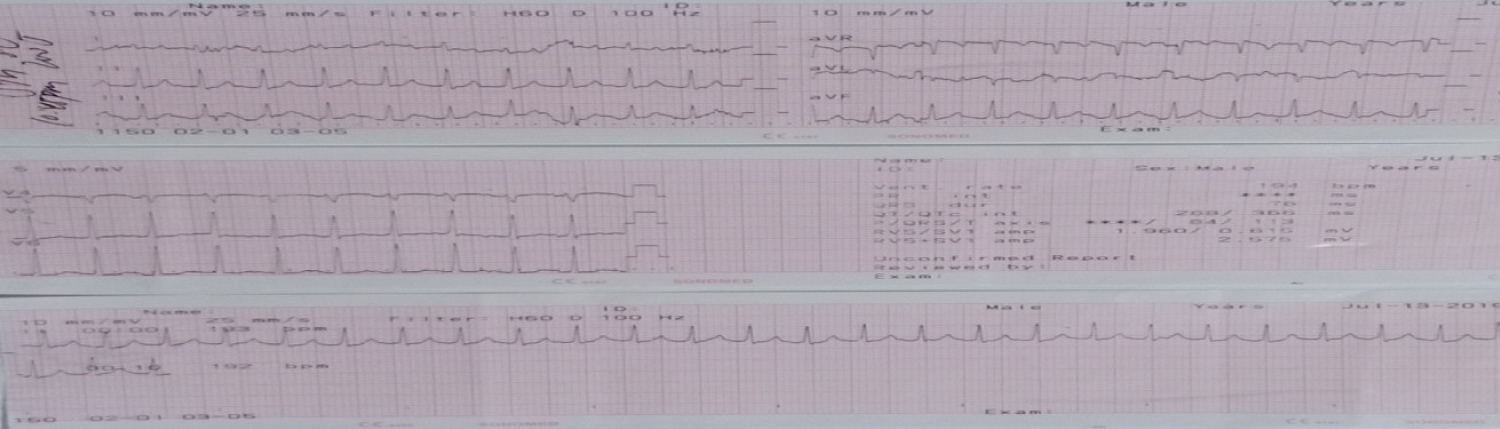 Figure 9: ECG shows supraventricular tachycardia after cardioversion of 200 Joules.
View Figure 9
Figure 9: ECG shows supraventricular tachycardia after cardioversion of 200 Joules.
View Figure 9
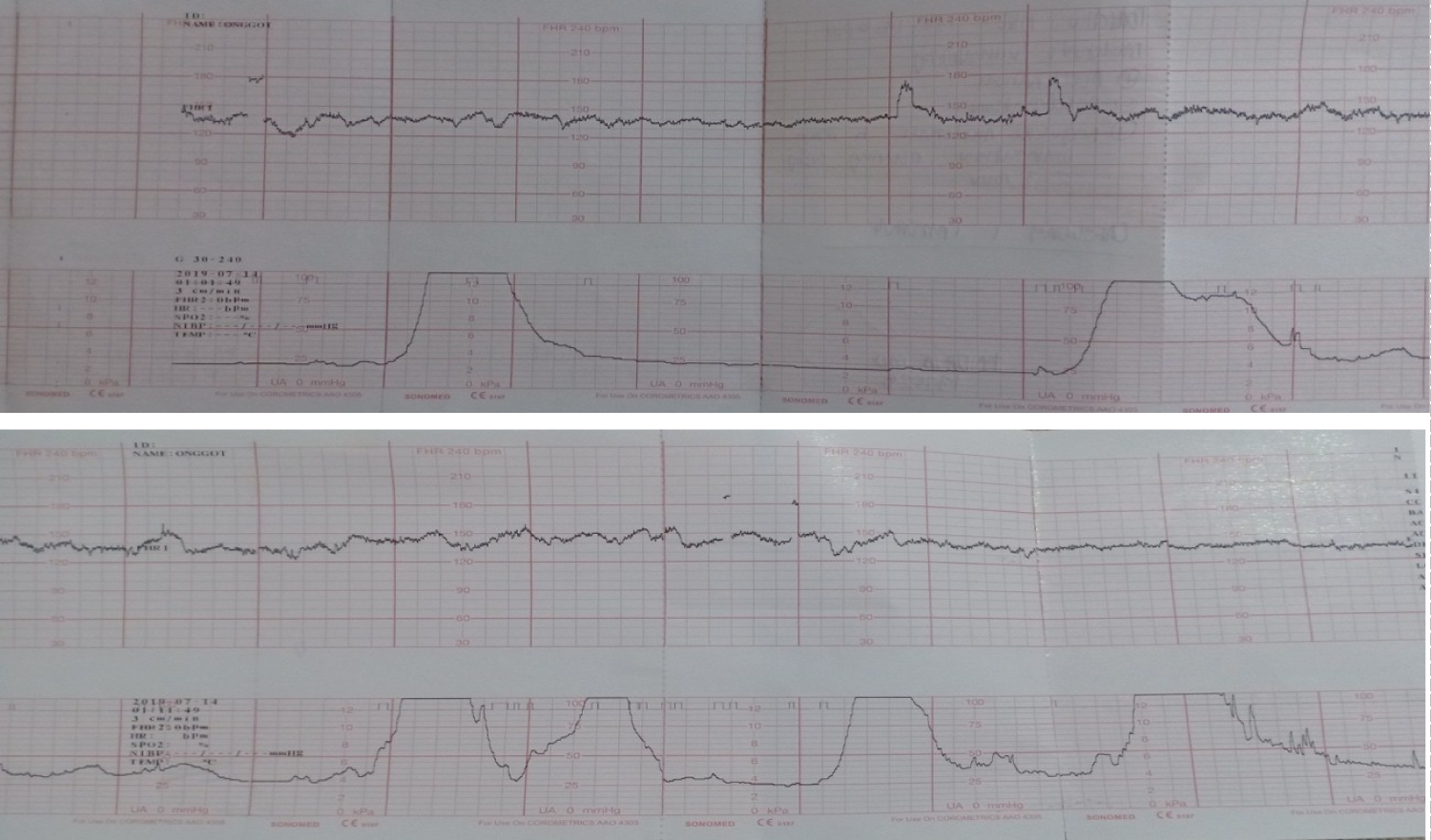 Figure 10: CTG tracing shows a Category I tracing: Baseline Fetal Heart Rate: 130-135 bpm
Figure 10: CTG tracing shows a Category I tracing: Baseline Fetal Heart Rate: 130-135 bpm
Variability: Moderate
(+) Accelerations (-) Decelerations
Regular moderate contractions occurring every 2-3 minutes
View Figure 10
On the fourth hour of admission, the cervix was noted to be 5 cm dilated, 50% effaced, intact bag of water, and cephalic at the station - 2. Plan was for assisted vaginal delivery under epidural anesthesia. Progress of labor was monitored by the following services: obstetrics, internal medicine, and anesthesiology. Atrial fibrillation was noted, hence, electrocardioversion at 200 joules was given 30 minutes prior to delivery. She delivered to a live term baby girl, with a birth weight of 2915 grams, APGAR score of 8, 9, 38 weeks by pediatric aging by spontaneous vaginal delivery with median episiotomy and repair under epidural anesthesia. Post-delivery, she was given another 200 joules of cardioversion due to atrial fibrillation. At the recovery room, her cardiac rate range was 160-180 bpm. She was transferred to the general intensive care unit where she was closely monitored (Figure 11).
 Figure 11: Patient at postpartum Day 1.
View Figure 11
Figure 11: Patient at postpartum Day 1.
View Figure 11
On postpartum day 3, a chest radiograph revealed marked cardiomegaly. The two-dimensional echocardiography revealed dilated left ventricle with severe generalized hypokinesia with an ejection fraction of 26%, dilated left atrium, normal right atrium, right ventricle, main pulmonary artery and aortic root dimension, thickened mitral valve leaflet with low flow configuration and widened EPSS. The aortic, tricuspid and pulmonic valves were structurally normal and there was no pericardial or pleural effusion noted. On color flow and Doppler study, there was moderate mitral regurgitation and mild pulmonary hypertension (Figure 12). These findings suggested a dilated cardiomayopathy. Gradually her heart rate decreased with the following medications: Atropine, Amniodarone, Lanoxin, Carvedilol, Metoprolol, and Warfarin. She was discharged and improved on her 10th hospital day (Table 1 and Table 2).
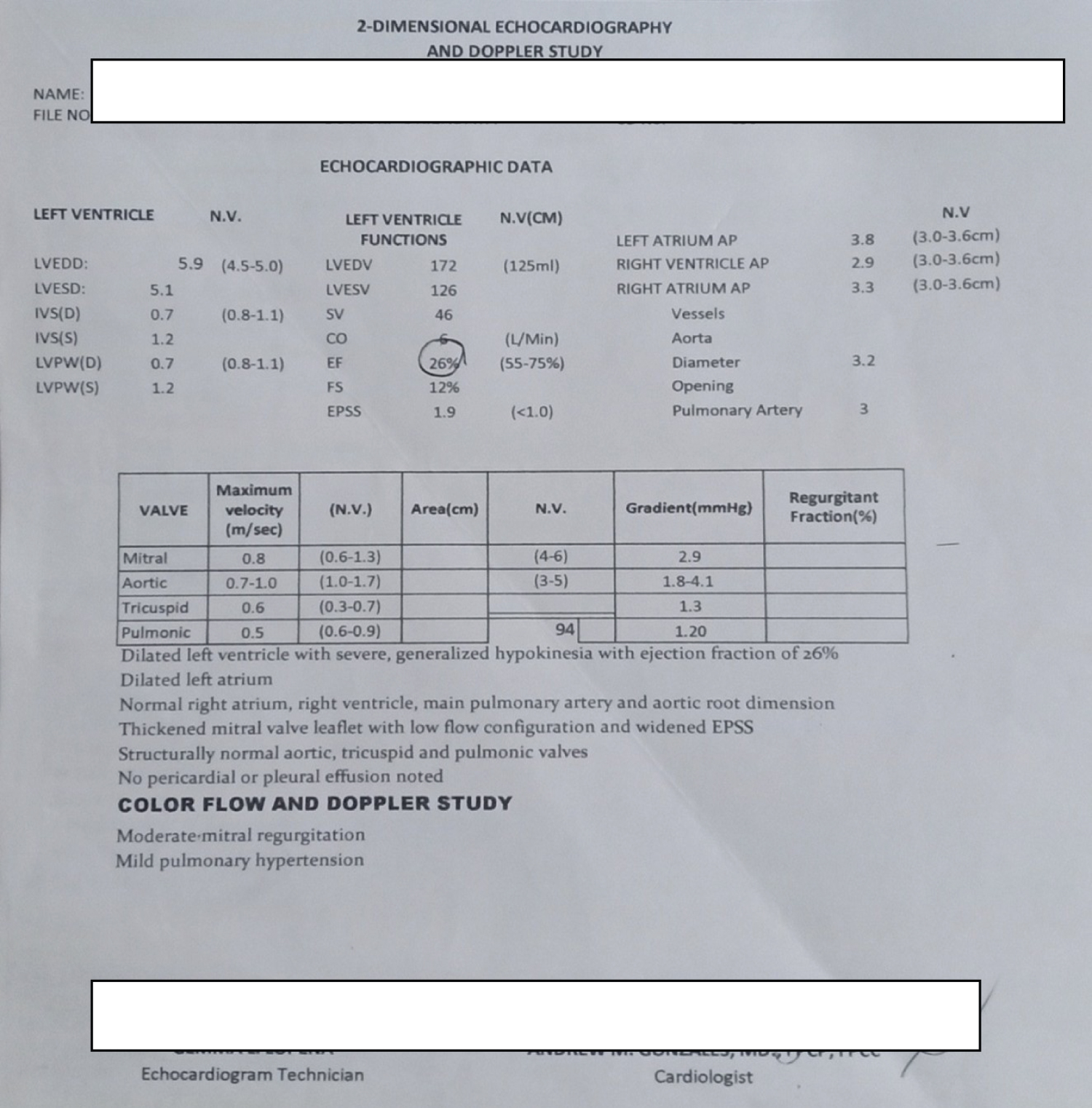 Figure 12: Shows the official two dimensional echocardiogram.
View Figure 12
Figure 12: Shows the official two dimensional echocardiogram.
View Figure 12
Table 1: Postpartum status and medications. View Table 1
Table 2: Postpartum status and medications. View Table 2
The management of supraventricular tachycardia in a woman in labor is a challenge to obstetricians. Each step in the management is critical because both maternal and fetal conditions should be considered.
Pregnancy has a dramatic effect on the cardiovascular system. The mechanism of the increased incidence of arrhythmias is due to the increased sympathetic activity during pregnancy. It begins at 5 weeks of pregnancy when there is an increase in cardiac output and heart rate with concomitant decrease in systemic vascular resistance. Approximately, there is an increase of 10 beats per min in the resting pulse rate during pregnancy. Marked changes in the maternal heart rate occur in the second trimester of pregnancy and the increase in gravidity imposes an increased risk of cardiac disturbances [3,4]. The blood volume increases by an average of 50% markedly from the latter half of the first trimester. This causes stretching of the atrium which is significant in arrhythmogenesis [4].
Paroxysmal supraventricular tachycardia is the most common arrhythmia seen in reproductive-aged women and during pregnancy. It has a prevalence of 24 cases per 100,000 hospital admissions and 20% experiences symptomatic exacerbations during pregnancy. The mean heart rate of a pregnant woman with supraventricular tachycardia is 184 beats per minute [5]. In a retrospective series done by Cordina, et al., it was found that only 0.17% of hospital admissions during pregnancy were due to cardiac arrhythmias and only 24 for every 100,000 pregnant women will be admitted for the management of supraventricular tachycardias. Based on Australian statistics, 36 pregnant women died from causes not directly related to pregnancy and one of those deaths is of cardiac pathology specifically arrhythmia which equates to 1.3 per million women who give birth [4].
Ventricular tachyarrhythmias are non-sustained and sustained forms of tachycardia originating from myocardial foci or reentrant circuits. Tachycardia is defined as a rhythm with a ventricular rate of more than 100 beats per minute. Our patient presented with symptoms of palpitations, and hemodynamic compromises such as dizziness or syncope due to a decrease in cardiac output and breathlessness due to a marked increase in cardiac filling pressures which started at 28 weeks AOG and persisted until the day of consultation. The primary diagnostic evaluation used is electrocardiography to confirm the presence of tachyarrhythmias.
Tachycardias originate from abnormalities of impulse formation and/or abnormalities in impulse propagation. In the presence of supraventricular tachycardias, immediate intervention is warranted. Giving intravenous Adenosine blocks AV node conduction which is a safe and effective agent for hemodynamically stable patients. However, in hemodynamically unstable gravidas whose pharmacologic management is contraindicated, synchronized electro cardioversion is recommended by the American College of Cardiology and American Heart Association. In some cases, it may cause sustained uterine contractions and fetal bradycardia. Moreover, if electro cardioversion were unsuccessful, long-term management with anticoagulants and heart rate control medications is necessary [5]. In our index case, the tachycardia might have originated from abnormalities in impulse propagation due to a structural cardiac entity. When she presented with unappreciated blood pressure, electro cardioversion was the treatment of choice over medical management. She had five synchronized cardioversions with increasing shock intensity from 50 to 200 Joules before delivery and one 200 Joules immediately postpartum. There were neither sustained uterine contractions nor fetal bradycardia during the acute management of this case.
There is a reported case of a 33-year-old at 37 weeks AOG with palpitations and tachycardia. Conservative measures such as carotid massage and Valsalva maneuver failed to correct her arrhythmia. She was medically cardioverted with Adenosine, Metoprolol, and Verapamil during labor and spontaneously delivered vaginally [6]. Another case of SVT in 26 weeks of pregnancy presented with palpitations and tachycardia. Synchronized electro- cardioversion was given because of failed medical cardioversion [7]. Management of such cases is individualized and depends on the presence of underlying structural or non-structural abnormalities in atrioventricular nodal conduction. It starts with a thorough history, physical examination, and an electrocardiogram to measure the electrical activity of the heart [8,9]. The decision to treat a woman depends upon the frequency, duration, and tolerability of the arrhythmia [2].
The management of supraventricular tachycardia in pregnancy is the same as for the non-pregnant population [10]. The first line of treatment is conservative management with vagal maneuvers. The second line is medical cardioversion with anti-arrhythmic to reduce the ectopic activity or modify impaired conduction. Medical cardioversion in pregnancy is imperative in case of hemodynamic instability and/or diminished uteroplacental blood flow.
Anti-arrhythmic agents have potential teratogenic effects on the fetus because of most pass through the placenta. These drugs can cause fetal tachyarrhythmia, hydrops fetalis, premature delivery, and fetal death [11]. The Food and Drug Administration categorized anti-arrhythmic medications as to the potential of the drug to cause birth defects if used during pregnancy. We used Adenosine and Verapamil which are Category C, Digoxin which is Category A, and Amniodarone which is Category D as anti-arrhythmogenic agents in this case.
Adenosine is the first-line drug in the treatment of arrhythmias as per its safety and effectivity. In 1994, seven pregnant women were given adenosine for the treatment of supraventricular tachycardia without adverse or fetal effects [12]. It was used in our index case but her dysrhythmia was resistant to Adenosine. Verapamil, a prototype calcium channel blocker is limitedly used during pregnancy due to its effects on fetal heart activity and uterine contractions. In a case of a digitalized hyperthyroid pregnant patient, dysrhythmia was successfully treated with Verapamil. She was hooked to continuous electronic fetal monitoring and there was no adverse effect noted during the management [13]. In the index case, Verapamil was used as the second line of medical treatment because our patient came in with unappreciated blood pressure. Before its administration, it was first assured that the patient was normotensive to avoid hypotension, one of its side effects. With the blood pressure was 110/80 mmHg, Verapamil was given but still, her dysrhythmia persisted. Digoxin was given next. It has a good safety profile but can cause miscarriage and fetal death in toxicity. It only provided a decrease in 19 beats/min. Amniodarone was also given to our patient and should only be used for short-term use. If used for prolonged periods, it can cause fetal hypothyroidism or fetal hyperthyroidism, goiter, IUGR, and prematurity [2]. It provided a gradual decrease in the maternal heart rate of our patient to 180's beats per minute.
Another treatment for supraventricular tachycardias is synchronized electro cardioversion. It is an effective treatment in the management of arrhythmias. In patients with unstable hemodynamics, an initial of 50-100 joules is given and can be given up to 400 joules. In 1965, 44 case reports described the use of electro-cardioversion during pregnancy with varying energy use from 50 to 400 Joules and with a success rate of 93.2%. Two maternal deaths were reported after electro cardioversion but secondary to the severity of underlying cardiac pathology. According to the literature, there were reported cases of preterm delivery and fetal distress with electro-cardioversion. The trajectory of energy transmitted by electro-cardioversion usually spares the uterus and only a minimal amount of current reaches it with little effect on the fetal heart due to the high fibrillation threshold of a small heart. The index patient was given a total of six electro cardioversion with increasing intensity from 50 to 200 Joules with anti- arrhythmogenic medications in between. The attempt to cardiovert the patient was maximized but her supraventricular tachycardia was intractable despite the conservative measures, medical management, and electro cardioversion given. The plan was to continue stabilizing the mother and deliver vaginally. Indications for an emergency cesarean section will be non-reassuring fetal status or bradycardia.
In the case of a pregnant woman at 37 weeks AOG who had supraventricular tachycardia resistant to medical cardioversion using Adenosine following the Spanish Society of Cardiology, electric counter shock and termination of pregnancy by cesarean section was performed [14]. However, in our case, we managed her with the combination of electro-cardioversion and medical cardioversion. The probability of cesarean delivery was also entertained as a mode of delivery specifically when there were fluctuations in maternal blood pressure, the presence of intractable supraventricular tachycardia despite the interventions, and considering the effects of all those measures on the fetus. The events were simultaneous and the plan changes from time to time. This patient was closely monitored by the team. At the OR table, the patient was persistently bearing down, forceps were not applied and she eventually delivered spontaneously by vaginal delivery under epidural anesthesia.
As presented, our index patient is not just an ordinary case of supraventricular tachycardia. The management done was indeed a medical challenge and a success.
The management of tachyarrhythmias in pregnancy poses a great challenge to clinical practice. It is critical and individualized. A thorough evaluation in a multidisciplinary approach is warranted to arrive at the right diagnosis, best judgment, and management. Decision-making is challenged by transient changes in fetal and maternal status as presented in this case.