Endometriosis is a chronic inflammatory disease defined as the presence of endometrium-like tissue outside the uterus. It is mostly found in women of reproductive age. Depending on the involved site, women can present with various symptoms. We report a case of rare, atypical site of endometriosis - primary inguinal cutaneous endometriosis. A 27-year-old woman presented to our Deparment with a history of a painful, firm, movable, subcutaneous nodule 1 × 1 cm of size in the right inguinum. She experienced flares of pain with her menstrual cycle and dysmenorrhea. Ultrasound revealed hypoechoic nodule with vascular flow. Punch biopsy of the nodule was performed. The biopsy results showed adipocytes and cell inclusions partially positive on epithelial membrane antigen. After surgical excision of nodule with wide margins, tissue was consisted from endometrial glands with encompassing fibrotic stroma. No additional signs of endometriosis were found. Because the condition is rare and can mimic presentations of other diseases, such as lymphatic nodule, keloid, dermatofibroma protuberans, cutaneous metastasis of cancer or dermatofibroma, cutaneous endometriosis can be difficult to diagnose.
Inguinal cutaneous endometriosis, Primary endometriosis, Epithelial membrane antigen
Endometriosis is a chronic inflammatory disease defined as the presence of endometrium-like tissue outside the uterus [1]. It is mostly found in women of reproductive age, within the general female population from 2 to 10%, up to 50% in infertile women [1]. Endometriosis lesions can be classified as ovarian, exclusively extra-ovarian or mixed [1-3]. The common sites of endometriosis are the ovaries, fallopian tubes, pelvic peritoneum and uterosacral ligaments, whereas the atypical sites include the gastrointestinal tract, urinary tract, soft tissues, chest etc [1-4]. Depending on the involved site, women can present with various symptoms. Most common are deep pelvic pain, dyspareunia and dysmenorrhea, but can be bowel obstruction, melena, hematuria, dysuria, dyspnea and swelling in soft tissues [1-4]. The average between onset of symptoms and diagnosis is between 8-12 years [1]. Diagnosis of extra-pelvic endometriosis can be demanding.
We report a case of rare, atypical site of endometriosis - primary inguinal cutaneous endometriosis. It is relatively uncommon and occurs when endometrial glands and stroma reside in the skin. Cutaneous endometriosis can be divided into primary and secondary endometriosis, depending on past medical history. A 27-year-old woman, gravida 0, para 0, presented to our Gynecology Deparment with flares of sharp, focal pain in inguinal region and connected it with her menstrual cycle. Her past gynecological medical history revealed dysmenorrhea. Results of laboratory evaluation and of tumor markers were within the reference values. She was able to palpate a tender mass arising from her right inguinum. On physical examination, a firm, painfull, movable subcutaneous nodule 1 × 1 cm of size with slight erythema of the overlying skin was observed. Ultrasound revealed hypoechoic nodule with vascular flow. Punch biopsy of the nodule was performed. The biopsy results showed adipocytes and cell inclusions partially positive on epithelial membrane antigen. After surgical excision of the nodule with wide margins, histopathological analysis demonstrated that the tissue was consisted from endometrial glands with encompassing fibrotic stroma. A routine gyecologic examination was unremarkable. Abdominal and transvaginal ultrasond showed no abnormalities, as well as pelvic magnetic resonance imaging. No additional signs of endometriosis were found.
Cutaneous endometriosis represents 0.5-1.0% of patients with atypical site of endometriosis [1,4]. It is often associated with prior surgical medical history [1,4]. If it presents without it, it is known as primary spontaneous cutaneous endometriosis [1-6]. From all extrapelvic endometriosis, umbilical occupies over 40%, followed by the inguinal area, perineal region and abdominal wall [4,6]. The mean age at presentation is 34 years [7]. The clinical diagnosis relies mostly on the recognition of the cyclic symptoms of pain and swelling of the lesion [1-6]. Almost 25% of women with cutaneous endometriosis also experience intrapelvic endometriosis [6], although our patient did not have any signs of it. Originates due to reflux of menstrual tissue through the oviducts, mechanical placement of endometrial tissue post-abdominal operation, presence of embryonic rests, peritoneal mesothelial cells becoming metaplastic (celomic metaplastic theory) or lymphatic and vascular spread [1,7]. The most commonly accepted pathogenesis are lymphatic or vascular migration due to migration of endometrial tissue from retrogression of menstruation [1,4,6]. A punch biopsy is not commonly used to diagnose endometriosis, however, if performed the results may show the presence of epithelial membrane antigen, CD 10, estrogen, progesteron receptors or Ki67 [7,8]. Cutaneous endometriosis is treated with surgical resection [1,4,6]. Histopathological examination is crucial and major discovery is that the tissue is consisted from endometrial glands with encompassing fibrotic, spindle-cell apperance stroma [7,8]. Primary cutaneous endometriosis can be differentially diagnosed with lymphatic nodule, keloid, dermatofibroma protuberans, cutaneous metastasis of cancer or dermatofibroma [2,6] (Figure 1, Figure 2 and Figure 3).
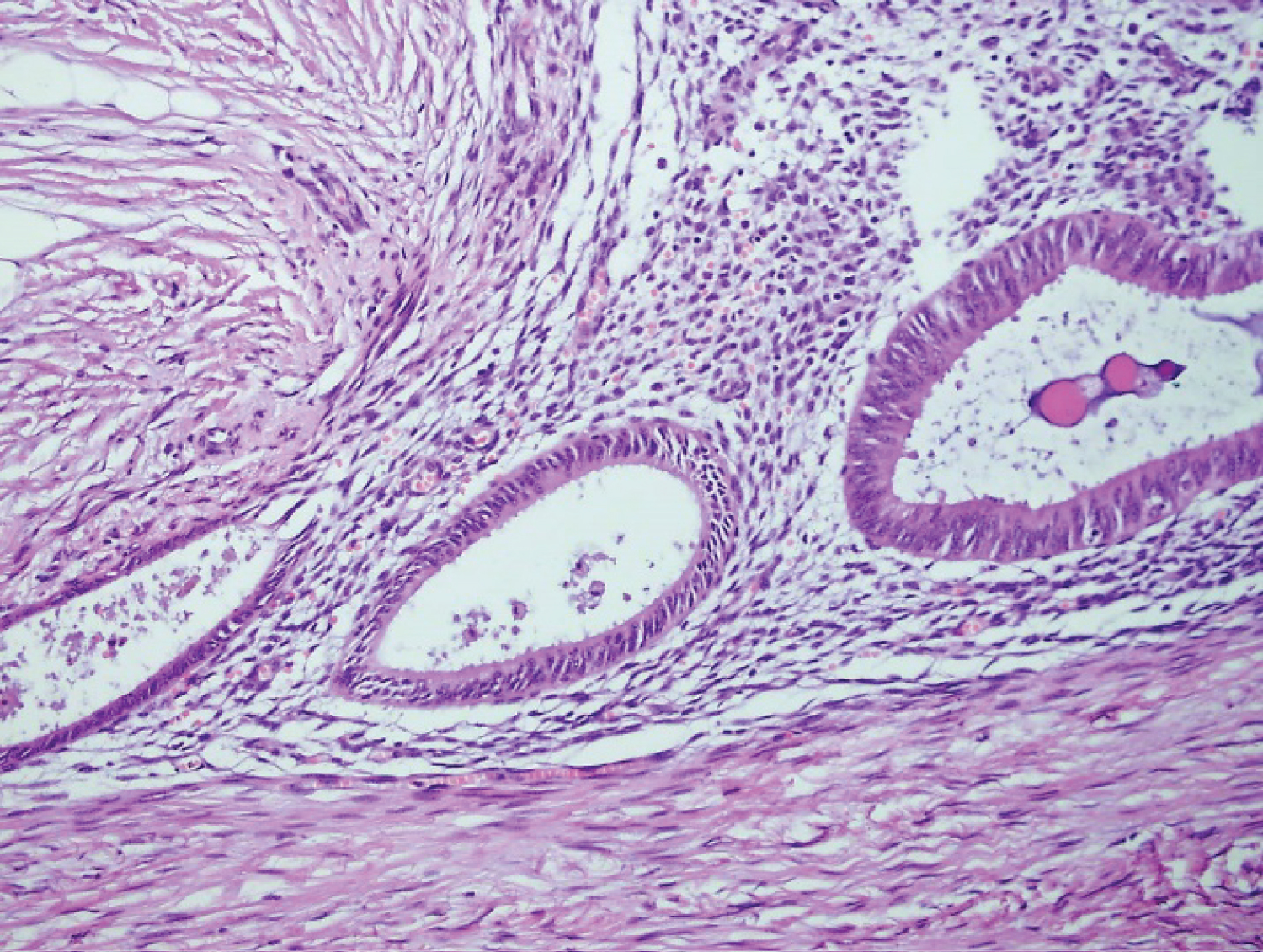 Figure 1: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (H&E x20).
View Figure 1
Figure 1: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (H&E x20).
View Figure 1
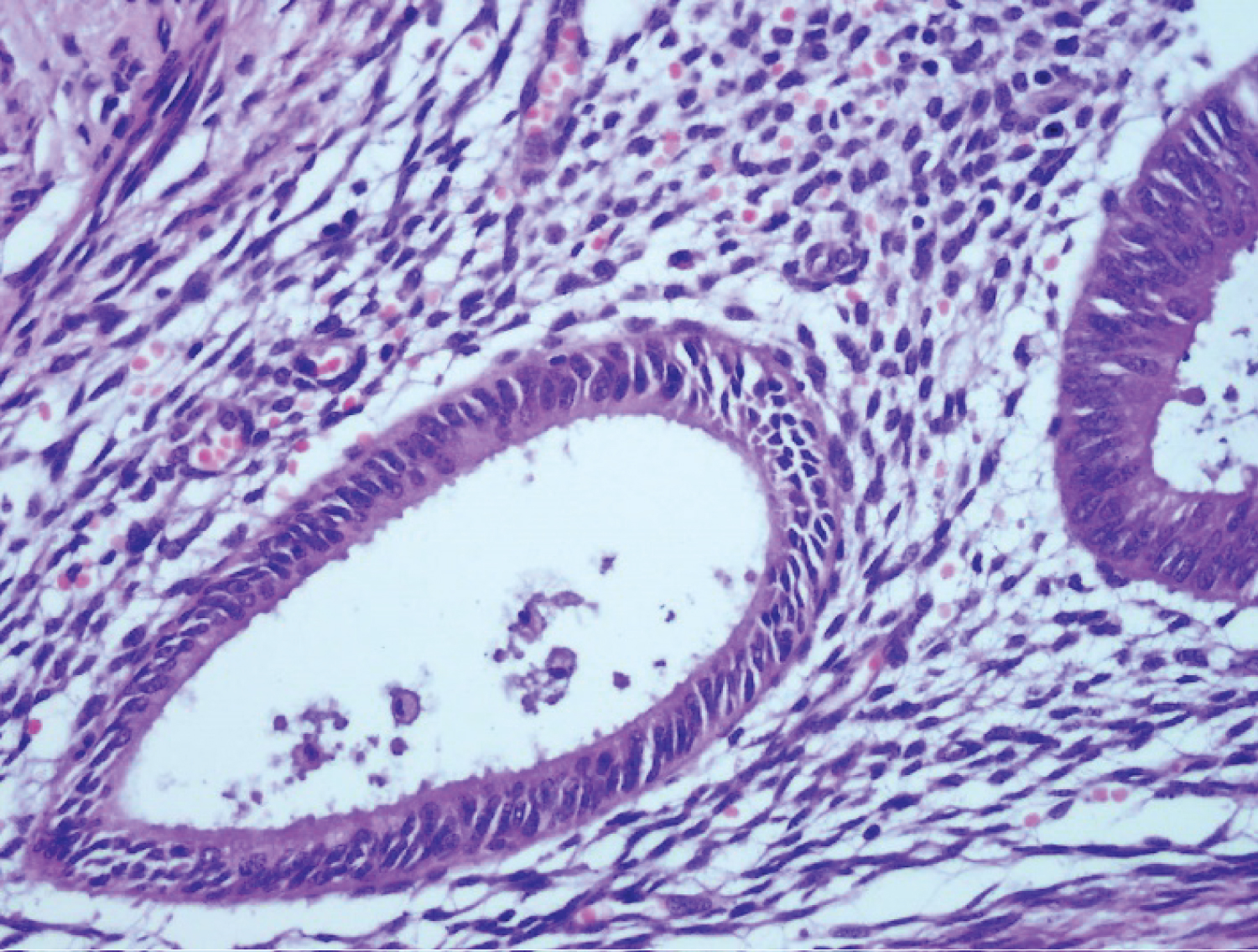 Figure 2: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (H&E x40).
View Figure 2
Figure 2: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (H&E x40).
View Figure 2
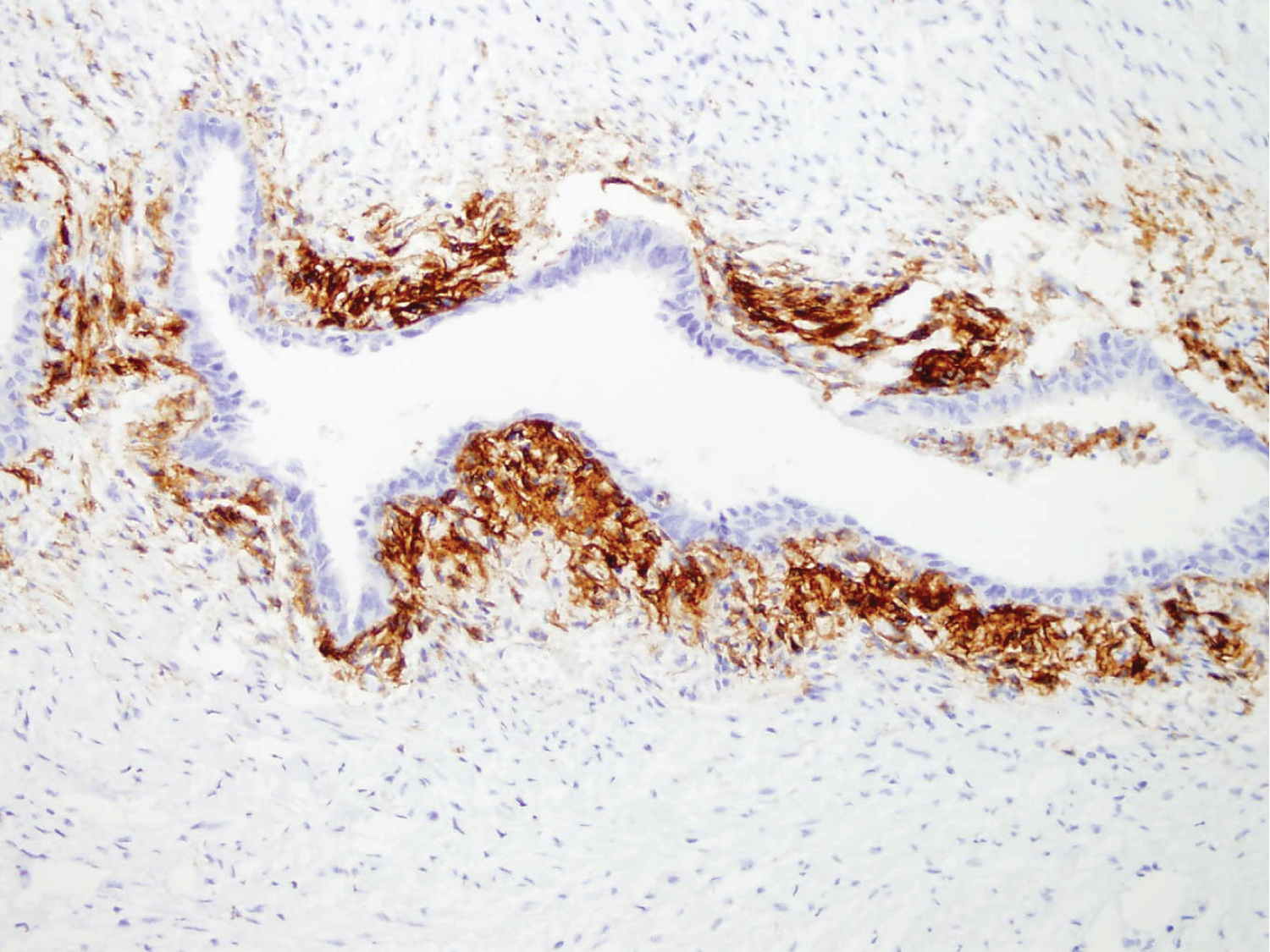 Figure 3: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (CD10).
View Figure 3
Figure 3: Microscopic picture of the lesion showing endometrial glands and stroma in the subcutaneous tissue of the skin (CD10).
View Figure 3
We conclude that primary cutaneous endometriosis is a rare disorder that can mimic presentations of other diseases. If is suspected, a punch biopsy can be performed, but surgical excision of the affected tissue and histopathological analysis is the golden standard. This implies that the diagnosis is difficult and requires a great deal of effort, skill and expertise to identify and confirm.
None.
None.
The authors declare that they equally contributed regarding the publication of this paper.