Background: Bladder flap hematoma is an unusual complication after cesarean section, where a hematoma forms between the bladder and the lower uterine segment. While small hematomas can be managed conservatively, large bladder flap hematomas are usually managed by drainage, laparoscopy or laparotomy.
Case presentation: We report a case of a 32-year-old lady who presented in labour, with a previous cesarean section 3 years back. Lower segment caesarean section was performed due to scar dehiscence and uterus was sutured, leaving peritoneal layers open. On the third post-operative day, she developed severe abdominal pain and ultrasound showed a large hematoma in the vesicouterine space. She was conservatively managed with antibiotics, analgesics and iron infusion. Her vital signs remained stable and repeat sonograms showed reduction in size of the hematoma. She had no further complaints and was subsequently discharged.
Conclusion: There is currently very little evidence regarding conservative management of large bladder flap hematomas. In our experience, conservative management is a safe and effective method with less patient morbidity, even for large bladder flap hematomas, provided the patient is clinically stable.
Bladder flap hematoma, Pelvic hematoma, Conservative management, Cesarean section, Obstetrical complication
Cesarean section (CS) is one of the most commonly performed operations on women worldwide. It accounts for 21% of all childbirth globally and likely to further rise to 29% by 2030 [1]. Early complications arise within 30 days after CS delivery, commonly, infections like endometritis or wound infections, hematomas or abscesses [2]. Hematomas after CS can be bladder flap hematomas which occur in the space between the bladder and the lower uterine segment or subfascial hematomas, which is an extraperitoneal collection in the prevesical space posterior to rectus muscles [3].
Bladder flap hematoma (BFH) is an unusual complication after CS performed without peritoneal closure and more common after CS with visceral peritoneal closure [4].
Usual presentations include a palpable mass, suprapubic pain, signs of hypovolemia and fever [5]. No standardized protocols exist for management of post CS BFH [6].
The various options for treatment include conservative medical management, percutaneous or transvaginal drainage and laparoscopy or laparotomy for significant collections [7]. Conservative management is usually employed for pelvic abscesses responding well to antibiotics and with size < 8 cm, while for larger collections surgical management with laparoscopy or laparotomy is preferred [7]. We describe a case of a large bladder flap hematoma post CS of size 13 cm that was treated by conservative medical management with complete resolution.
A 31-year-old G2P1L1 with a previous CS 3 years back and having an uneventful antenatal course, was admitted at 40 weeks of gestation with mild labour pains. Vitals were stable, cervix was soft and 50% effaced. Oxytocin infusion was started for augmentation of labour. Subsequently, in view of fetal distress and scar tenderness, she was taken up for emergency CS under spinal anaesthesia. Partial thickness dehiscence of old CS scar was found. Lower segment CS with Kerr’s incision was done and fetus was delivered. Newborn weighed 3.1 kg, female, alive and cried at birth. Uterus was sutured in two layers and peritoneal layers were left open. The procedure was uneventful.
On the third postoperative day, patient developed persistent lower abdominal pain and features of paralytic ileus. A transabdominal ultrasound showed the presence of a large pelvic hematoma between lower uterine segment and the bladder measuring 10.8 × 13.3 × 4.8 cm, with a volume of 366 ml (Figure 1). A complete blood count (CBC) showed a hemoglobin of 9.3 g/dL, hematocrit 28.3% and leukocytosis (16150 cells/mL).
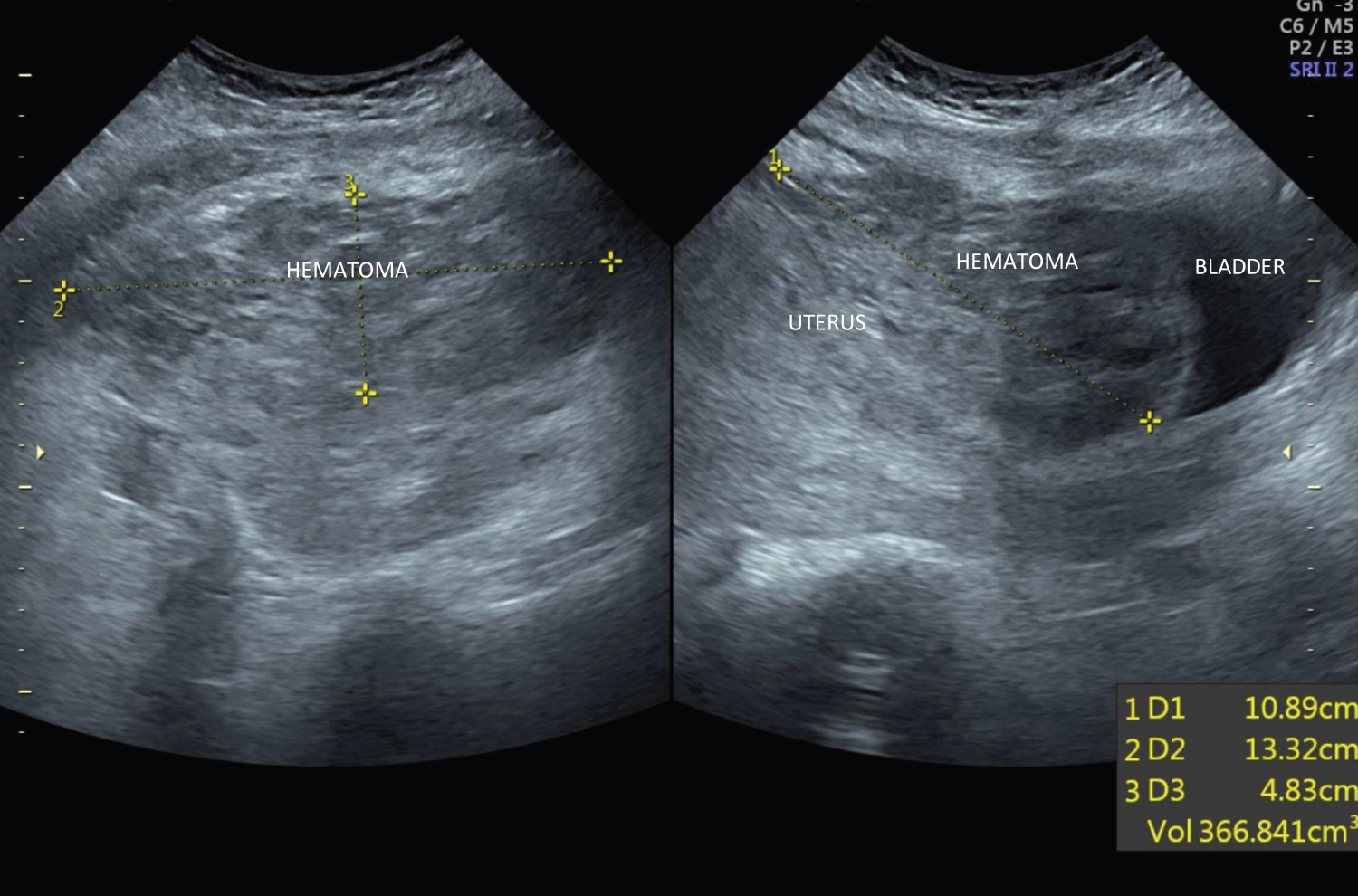 Figure 1: Bladder flap hematoma at presentation.
View Figure 1
Figure 1: Bladder flap hematoma at presentation.
View Figure 1
She was started on parenteral antibiotics - Ceftriaxone and Metronidazole intravenously for 5 days. She was also given parenteral iron infusions and oral Serratiopeptidase and Diclofenac for inflammation and pain, once bowel functions returned to normal.
On the sixth postoperative day, she developed two isolated fever spikes and a CBC showed hemoglobin of 9.4 g/dL, hematocrit 27.9% and a declining leukocyte count (12000 cells/mL). Coagulation profile, platelet counts and renal function were in the normal range with an elevated C-reactive protein (26.7 IU/Litre). A repeat ultrasound on 7 th postoperative day showed an organising hematoma in utero-vesical space with a reduction in size, measuring 9.9 × 5.5 × 7.8 cm.
A repeat CBC on 9 th postoperative day showed an increase in hemoglobin (10.4 g/dL) and hematocrit (30.9%).
Conservative management was continued and she remained afebrile with stable vitals and no further complaints.
She was subsequently discharged, with regular follow up sonograms that showed a serial reduction in size of the hematoma. The last ultrasound was done 5 months after CS, which showed a small, ill defined, hypoechoic lesion between the uterus and bladder, measuring 2 × 1.7 cm, indicating a residual or chronic hematoma (Figure 2).
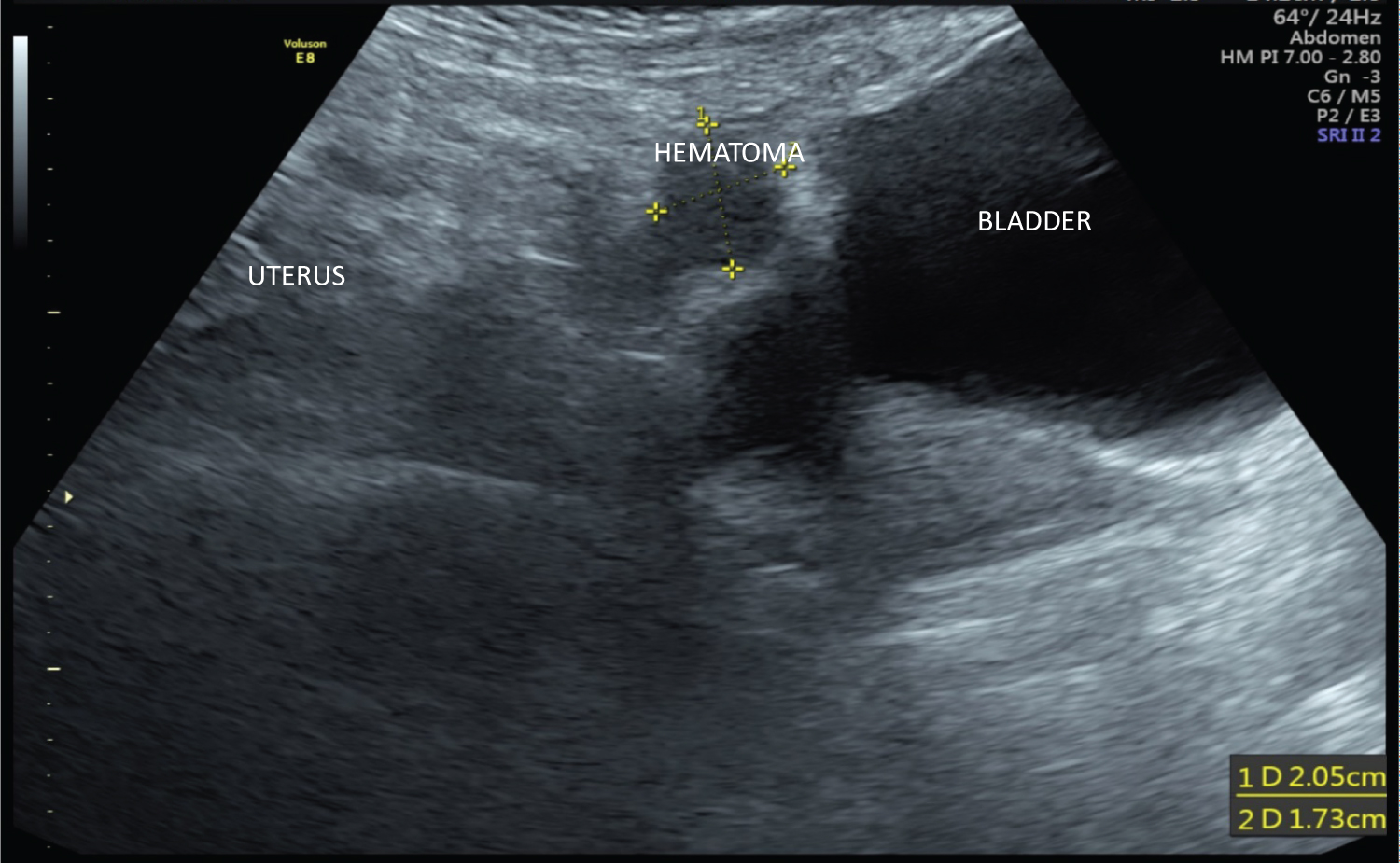 Figure 2: Residual hematoma after 5 months.
View Figure 2
Figure 2: Residual hematoma after 5 months.
View Figure 2
Cesarean section (CS) is the most frequently utilized intraperitoneal obstetric surgical event, and the two most common techniques used are the Misgaw Ladach technique (or Stark CS) and the traditional method [8]. The difference between these methods is in the closure of the peritoneum: Stark method does not utilize peritoneal closure while the traditional method sutures the visceral and parietal peritoneum.
An unusual complication of CS is the bladder flap haematoma (BFH). During CS, if hemostasis is not achieved after closure of uterine incision, bleeding at the incision site can lead to formation of a hematoma in the potential space between the bladder and lower uterine segment (vesicouterine space), called BFH. CS with closure of peritoneal layers is found to be associated with higher rates of hematoma formation, which leads to prolonged hospital stay and increased rates of puerperal complications in these patients [9,10]. Conversely, CS without suturing the visceral peritoneum is thought to be associated with reduced incidence of BFH [4,5]. Large hematomas arising after CS without peritoneal closure can also enter into the open peritoneal cavity causing hemoperitoneum [4].
Usual presentations of pelvic hematomas include a palpable mass, suprapubic pain, signs of hypovolemia (tachycardia, drop in haemoglobin level, decreased urine output) and infections (fever, leukocytosis). A rare presentation of BFH with hematuria has also been described by Ilhan, et al. [5]. Fever in the post CS patient may also indicate the presence of a potentially life-threatening complication, like an abscess, ovarian vein thrombosis or uterine dehiscence. Imaging findings are often utilized to ascertain the presence of such complications and to differentiate between them. In a study conducted by Maldjan, et al., 50 patients with persistent low-grade fevers following CS were referred for magnetic resonance imaging (MRI), performed 3-10 days postoperatively. Bladder flap hematomas were seen in 64% of these cases [11].
Ultrasound (US) is considered the preliminary imaging modality which shows a BFH as a hyperechogenic, heterogenous collection between the bladder and inferior uterine segment [2]. US can also be utilised for clinical follow up and as a guide for further management. Presence of air in the collection, internal septations and peripheral vascularisation suggests an infected hematoma/abscess formation [2,12]. MRI is considered the best modality for evaluation of female pelvis without exposure to ionising radiation and BFH appears hyperintense in T1 and T2 weighted MRI [11,13].
No clear and defined protocols exist for management of a post CS BFH in scientific literature. Different treatment modalities include conservative medical management, percutaneous or transvaginal drainage, laparoscopy or laparotomy for significant collections. BFH’s of size < 4 cm generally do not require any therapeutic procedures [3].
Baker, et al. in 1984 described 7 patients with BFH from 1458 CS, using imaging and clinical criteria [12]. Five of them were conservatively managed with antibiotics, one had an explorative laparotomy and one patient required a hysterectomy for myometritis and uterine wound dehiscence.
Ilhan, et al. recorded a case of a small BFH measuring 86 × 77 mm presenting with hematuria, that was managed conservatively with antibiotics and showed complete resolution in 2 weeks [5].
Tinelli, et al. described two cases of BFH that developed post CS with suturing of visceral peritoneum [8]. Both were managed by laparoscopic drainage of the hematoma with postop resolution. They described laparoscopy as a safe, effective and minimally invasive method for management of BFH.
A case of BFH 11 days post CS, measuring 7 × 3 × 4 cm was described by Lata, et al., which was managed by laparoscopic drainage and patient showed good clinical recovery [7]. They recorded laparoscopy as an appropriate and feasible method for management of pelvic hematoma in both stable and deteriorating patients.
Tinelli, et al. described 10 symptomatic women with BFH who were managed by laparoscopy and drainage with no further complications [6].
Alvarez-Sarrado, et al. reported a case of 4 women diagnosed with infected bladder flap hematomas after CS. They were managed by ultrasound guided percutaneous drainage following which they showed significant improvement [14]. They concluded that ultrasound percutaneous drainage is a highly efficient and less invasive technique for management of BFH that also helps to obtain a sample for culture to guide further antibiotic treatment.
There are very few studies that mention large pelvic hematomas being managed conservatively. In our study, we describe a large BFH post CS without closure of peritoneum, measuring 10 × 13 cm, treated with conservative medical management. Patient showed good recovery with resolution of hematoma in a few months. This approach led to significantly less morbidity and reduced hospital stay in the puerperal period.
Bladder flap hematoma is a rare complication following CS where visceral peritoneum is not sutured. It can be easily and accurately identified using sonography. Conservative medical management is one of the treatment modalities that can be used for large hematomas as well, provided the patient is in stable clinical status. Scientific literature currently does not provide much evidence regarding conservative treatment of large BFH’s. Hence, several more studies are needed to establish conservative management as a safe and effective method, even for large BFH’s, with significantly less patient morbidity.
Written informed consent was obtained from the patient for publication of her data and related images, with all identifying information removed.
The authors declare that there are no conflicts of interest regarding the publication of this case report.
The authors acknowledge the patient and her family for their cooperation.
Haezel Ann Shibu contributed to conception of the case report, acquiring and interpreting the data, drafting the manuscript, undertaking literature review and revising the article; Anju Mary Varughese contributed to patient care, conception of the case report, acquiring and interpreting the data, drafting the manuscript and revising the article.
Both authors approved the final submitted manuscript.
No funding was received for conducting this study. This study was conducted in Ahalia hospital Abudhabi, and approval was obtained to publish this study.