Adnexal torsion is a surgical emergency that cannot be ignored in women. It is a diagnostic and therapeutic challenge. While the occurrence of adnexal torsion in pregnant women is rare, it still can present significant risks. We present the case of a 23-year-old woman, pregnant at 24 weeks of amenorrhea and consulted for an acute abdominal pain. She underwent exploratory laparoscopy, which revealed ovarian torsion caused by a functional cyst along with epiploic appendigitis. During the procedure, we punctured the cyst, detorsed the adnexa and resected the epiploic appendigitis. The postoperative follow-up was favourable. Ultrasound at 2 weeks showed continued pregnancy.
Adnexal torsion, Pregnant women, Laparoscopy
Adnexal torsion in pregnancy is a rare surgical emergency, with an incidence of 1 to 5 per 10000 pregnancies [1]. It is defined by partial or complete rotation of the adnexal mass around its vascular axis. This rotation may be favoured by the presence of an adnexal mass or, more rarely, may occur in healthy adnexa [2]. It is a surgical emergency whose clinical diagnosis remains difficult due to the non-specificity of the clinical picture, the sympathetic signs of pregnancy that may complicate the diagnosis, and the increased size of the uterus that makes the examination difficult. We present a case of adnexal torsion and epiploic appendigitis in a pregnant woman in the second trimester.
A 26-year-old woman, gravida 1, para 0, pregnant in 24 weeks of amenorrhea, presented to our emergency department with sudden onset of severe abdominal pain and vomiting. The patient had no particular medical history. She had no other gynecologic or urinary symptoms.
She described intermittent severe abdominal pain, cramping, that had started four hours earlier in the right iliac fossa, followed by two episodes of vomiting. Her pain score was 9/10.
On examination, the patient's temperature was 37 °C, her blood pressure was 110/70 mmHg, and her pulse rate was 88 bpm. Abdominal examination revealed tenderness to superficial palpation with a smooth uterus over the umbilical region. Pelvic examination showed no bleeding, no abnormal vaginal discharge.
Ultrasound revealed a fetus with good vitality, eutrophic. The right ovary was covered with a pure anechogenic cyst, non-vascularized on Doppler, measuring 15 * 9 cm. The left ovary was normal.
When we were faced with a patient who was in severe pain, we decided to perform a diagnostic laparoscopy. Exploration revealed a large functional cyst measuring 15 * 10 cm (Figure 1). The fallopian tube was twisted with three turns of the spiral (Figure 2) and an epiploic appendigitis (Figure 3). After evacuation of the cyst, a detorsion was performed. Yellow fluid was obtained, confirming the functional origin of the cyst, followed by resection of the epiploic appendigitis. Postoperative follow-up was favorable and the patient was discharged one day later. The ultrasound after 2 weeks showed an evolving pregnancy.
 Figure 1: Ovarian cyst.
View Figure 1
Figure 1: Ovarian cyst.
View Figure 1
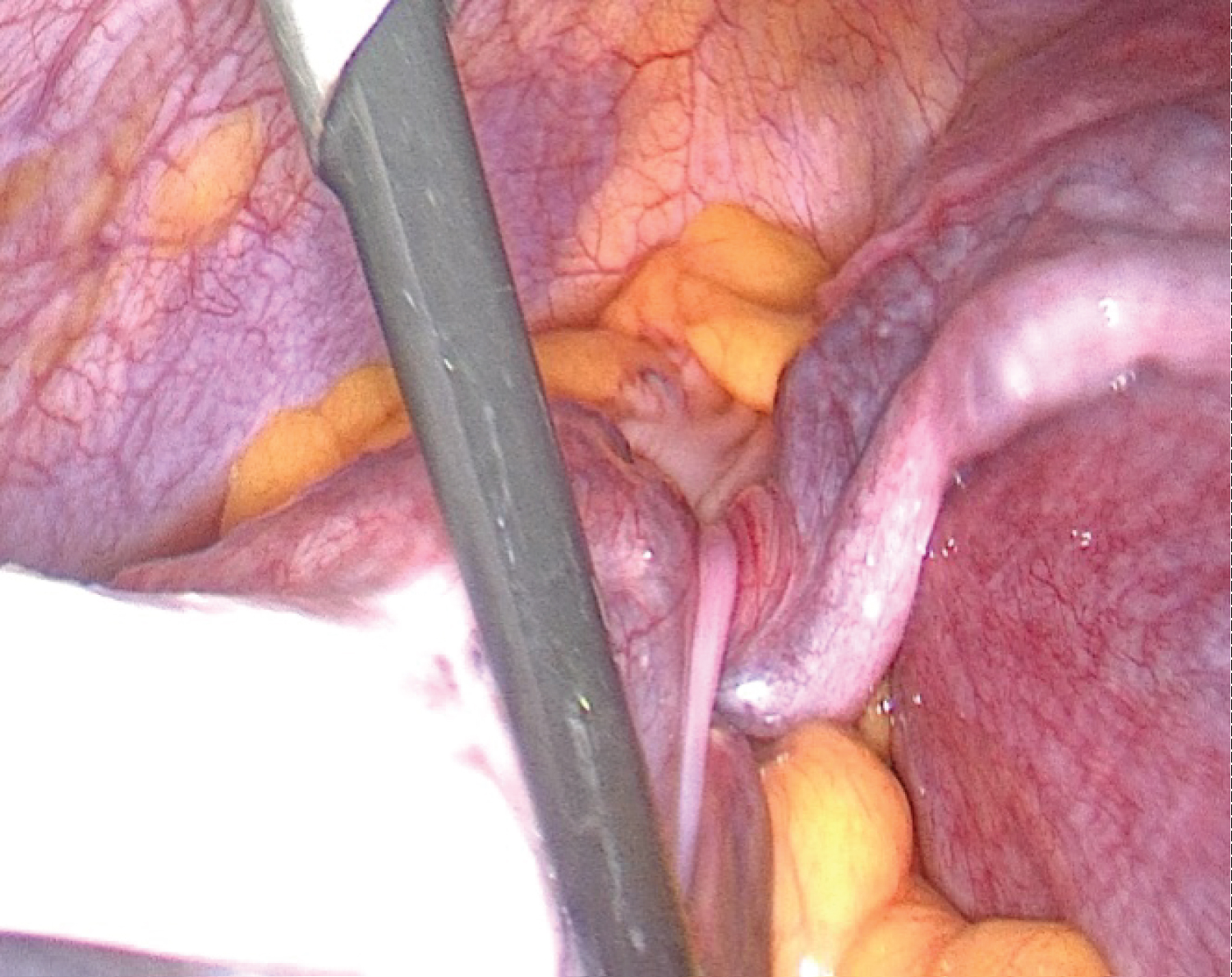 Figure 2: The twisted fallopian tube.
View Figure 2
Figure 2: The twisted fallopian tube.
View Figure 2
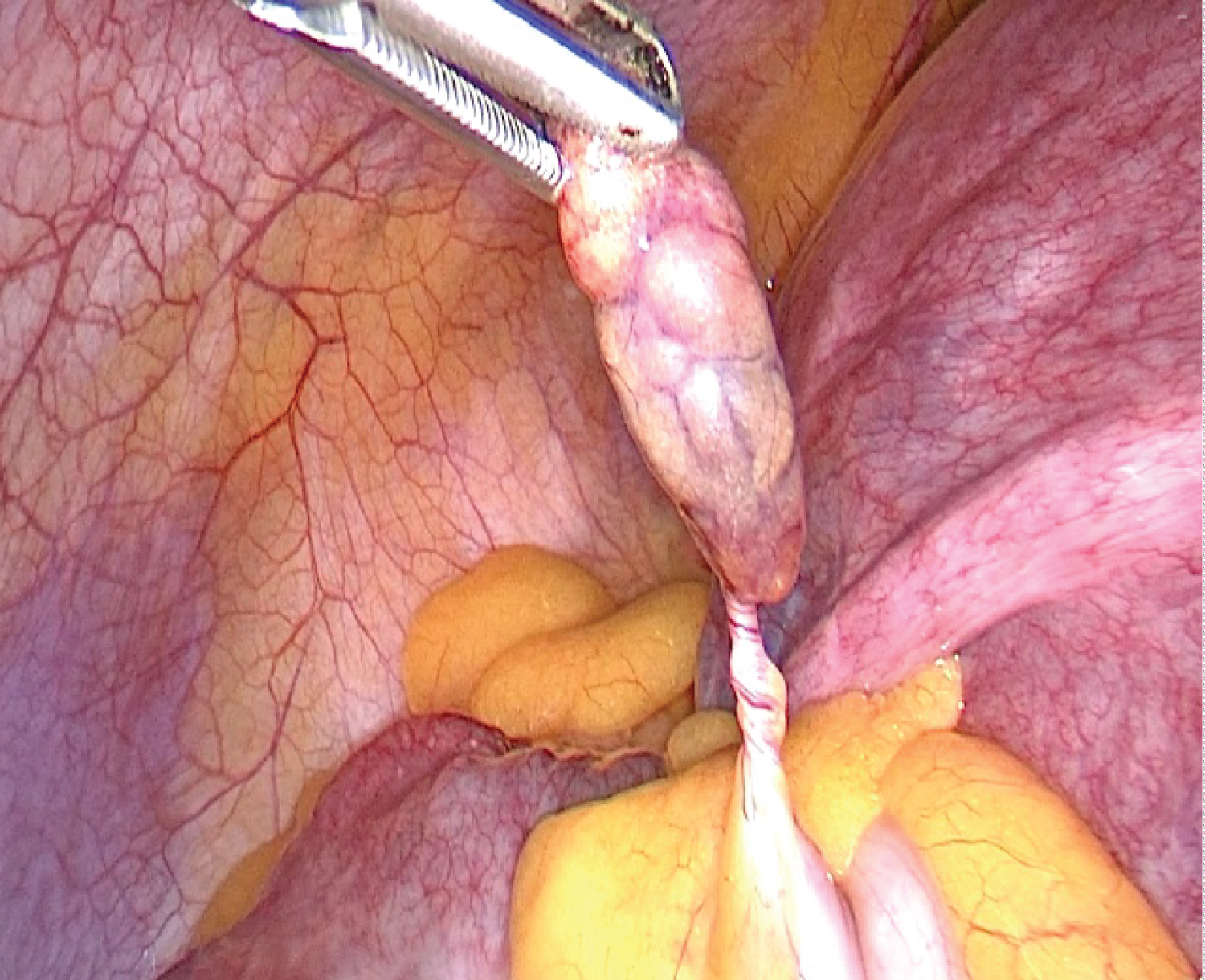 Figure 3: Epiploic appendigitis.
View Figure 3
Figure 3: Epiploic appendigitis.
View Figure 3
Adnexal torsion during pregnancy is rare [1]. It can occur at any stage of pregnancy, but mainly in the first trimester, which can be explained by a decrease in adnexal mobility during the second and third trimesters as the uterus increases in size [2].
Adnexal torsion occurs most frequently on the right side and is favoured by benign or malignant ovarian lesions or during ovarian hyperstimulation in early pregnancy [3].
The symptomatology of torsion during pregnancy may be non-specific, but generally the patient presents with acute pelvic pain and vomiting. The diagnostic difficulty lies in the fact that the differential diagnosis, whether related to pregnancy or not, must be eliminated [4].
In ovarian cyst torsion, abdominal tenderness is the most common sign seen on clinical examination.
Ultrasound is the gold standard for ovarian cyst torsion; it eliminates differential diagnosis and identifies factors that may favor torsion, such as cyst visualization. According to the literature, the ultrasound signs that may suggest the diagnosis of adnexal torsion are: ovarian edema, adnexal mass, whirlpool sign, absent ovarian Doppler flow, pelvic fluid [5]. However, ultrasound exploration of the adnexa is difficult during pregnancy because of the increased size of the uterus and the retro-uterine position of the adnexa during pregnancy, especially during the second and third trimesters.
Nevertheless, diagnosis of ovarian torsion remains intraoperative. Treatment is generally conservative, based on detorsion with or without ovariopexy.
The approach mainly depends on the gestational age. In general, in the first and second trimesters, the approach is laparoscopic, whereas in the late second and third trimesters, the approach is laparotomy, which allows easy and direct access to the adnexa [6]. Laparoscopic surgery is recommended for pregnancies less than 17 weeks amenorrheic with the following safeguards: preference for open laparoscopic surgery, insufflation between 8- and 12- mmHg, adequate trocar position, and gentle uterine mobilization [7]. However, recent publications in the literature encourage the laparoscopic approach even in the third trimester [7].
Recent literature advises conservative treatment of the ovary even in the stage of necrosis, as there is no correlation between the macroscopic appearance of the ovary and the degree of ischemia and functional recovery capacity of the ovarian tissue [7].
Epiploic appendigitis is a benign and typically self-limiting inflammation of the epiploic appendix. The exact incidence of this condition remains unclear. Clinical manifestations commonly involve persistent localized pain, which varies depending on the location of the affected appendix [1].
The definitive diagnosis is most commonly established through CT scan imaging, with or without contrast injection. On imaging, epiploic appendigitis typically manifests as a round and ill-defined oval lesion adjacent to the colon, with a density slightly higher than that of normal fat.
The pathognomonic "ring sign" often appears as a peripheral hyperdensity corresponding to inflammation of the serosa. However, it's important to note that the absence of this sign does not necessarily exclude the diagnosis of acute epiploic appendigitis [8,9].
Treatment primarily revolves around medical management, focusing on pain control. Surgical intervention is reserved for patients whose symptoms fail to ameliorate with conservative measures or who develop complications [8,9].
The occurrence of adnexal torsion as well as Epiploic appendagitis during pregnancy remain rare , that explains why the association of these two phenomens during pregnancy has not yet been mentioned in literature , that’s why our case is interesting.
In the setting of acute pelvic pain in pregnant women, adnexal torsion is an emergency that should not be overlooked. Conservative treatment is currently the gold standard, and appropriate management is necessary to avoid potential maternal and fetal complications.