Background: Congenital malformations of the uterus vary in frequency according to studies throughout the world. They may be discovered antenatally, at birth or during childhood. Some remain unrecognised and are discovered later by chance during radiological investigations or surgery. We report two cases of uterine malformations, one case of a unicervical bicornuate uterus and one case of a unicornuate uterus discovered incidentally during emergency caesarean sections.
Cases presentation
Case 1: An 18-year-old pregnant woman, housewife, primigravida consulted the obstetrics and gynaecology department of the Bogodogo University Hospital for abdomino-pelvic pain with uterine contractions in a full-term pregnancy. On clinical examination, an emergency caesarean section was indicated for a breech fetus in a primigravida. Intraoperative exploration revealed a unicervical bicornuate uterus. The right hemi-uterus was gravid with a well-formed lower segment. The second, on the left, was only slightly enlarged, comparable to a pregnancy of around 07 weeks.
Case 2: A 29-year-old pregnant woman, housewife, 4th gesture and 2nd pare was referred to us for premature rupture of membranes in a scarred uterus. A caesarean section was indicated for the same diagnosis. Intraoperatively we found a uterus with a single uterine horn and a healthy-looking right homolateral ovary and fallopian tube.
Conclusion: Congenital malformations of the uterus are relatively common. Many of these anomalies remain unrecognised because they are often silent. Pregnancies with a malformed uterus can sometimes progress asymptomatically to term, but the risk of caesarean section is even higher than in the general population because of the high risk of abnormal presentation.
Congenital malformations are generally discovered antenatally, at birth or during childhood. Some remain unrecognised and are discovered later by chance during radiological investigations or surgery [1-3]. Among these are congenital malformations of the uterus, which include several entities such as bicornuate, unicornuate, didelphic, arched, septate uteri and other forms.
These congenital anomalies of the uterus vary in frequency depending on the study, and are often a source of miscarriage and infertility. They have a prevalence of approximately 0.5 to 6.7% in the general population [4,5], 7.3% in the infertile population and approximately 16.7% in cases of recurrent miscarriage [4]. We report two cases of uterine malformations, one case of a unicervical bicornuate uterus and one case of a unicornuate uterus discovered incidentally during emergency caesarean sections at the Bogodogo University Hospital. The interest of these clinical observations is to show the obstetrical prognosis in women with these uterine malformations.
An 18-year-old parturient housewife consulted the obstetrics and gynaecology department of the Bogodogo University Hospital for abdomino-pelvic pain with uterine contractions due to a full-term pregnancy.
History taking revealed that these pains had started the day before her admission. Her medical and surgical history was unremarkable.
Mrs. SB was primigravida nulliparous. She had only had one prenatal consultation. The date of her last menstrual period could not be determined. She also had no early obstetric ultrasound. She had in her possession a late ultrasound carried out 04 days before her admission estimating the gestational age at 38 weeks of amenorrhoea and 05 days, which gives an amenorrhoea of approximately 39 weeks and 02 days.
Her general condition was good and her physiological vitals normal.
Obstetrical examination revealed a gravid uterus with a measured uterine height of 34 centimetres. Fetal heart sounds were heard in the upper right quadrant and measured at 135 beats per minute. The contractions were regular, close together and of long duration. Examination with a speculum revealed non-partitioned vaginal walls and a single, healthy-looking cervix. Vaginal examination revealed an effaced cervix dilated to 3 centimeters, a bulging water sac and a breech presentation.
An emergency caesarean section was indicated for a breech fetus in a primigravida. This caesarean section enabled a live male newborn to be extracted through the podalic pole, who screamed immediately and weighed 3500 grams.
Post-extraction examination revealed two distinct hemi-uteri, separated and comprising two uterine bodies which joined at the lower end to form a single cervix. The junction zone was covered by the mesocolon. Each of these two hemi-uteri carried the homolateral adnexa (ovary, fallopian tube and means of fixation) which were normal in appearance. The right hemi-uterus was gravid with a well-formed lower segment. The second, on the left, was slightly enlarged, comparable to a pregnancy of around 07 weeks.
Post-operative recovery was straightforward for the mother and child, and they were discharged on the 3 rd day post-caesarean section.
Mrs. SB did not report any urinary or sexual problems. An appointment was given to the patient for an exploration in search of other associated malformations, but she was lost to follow-up (Figure 1 and Figure 2).
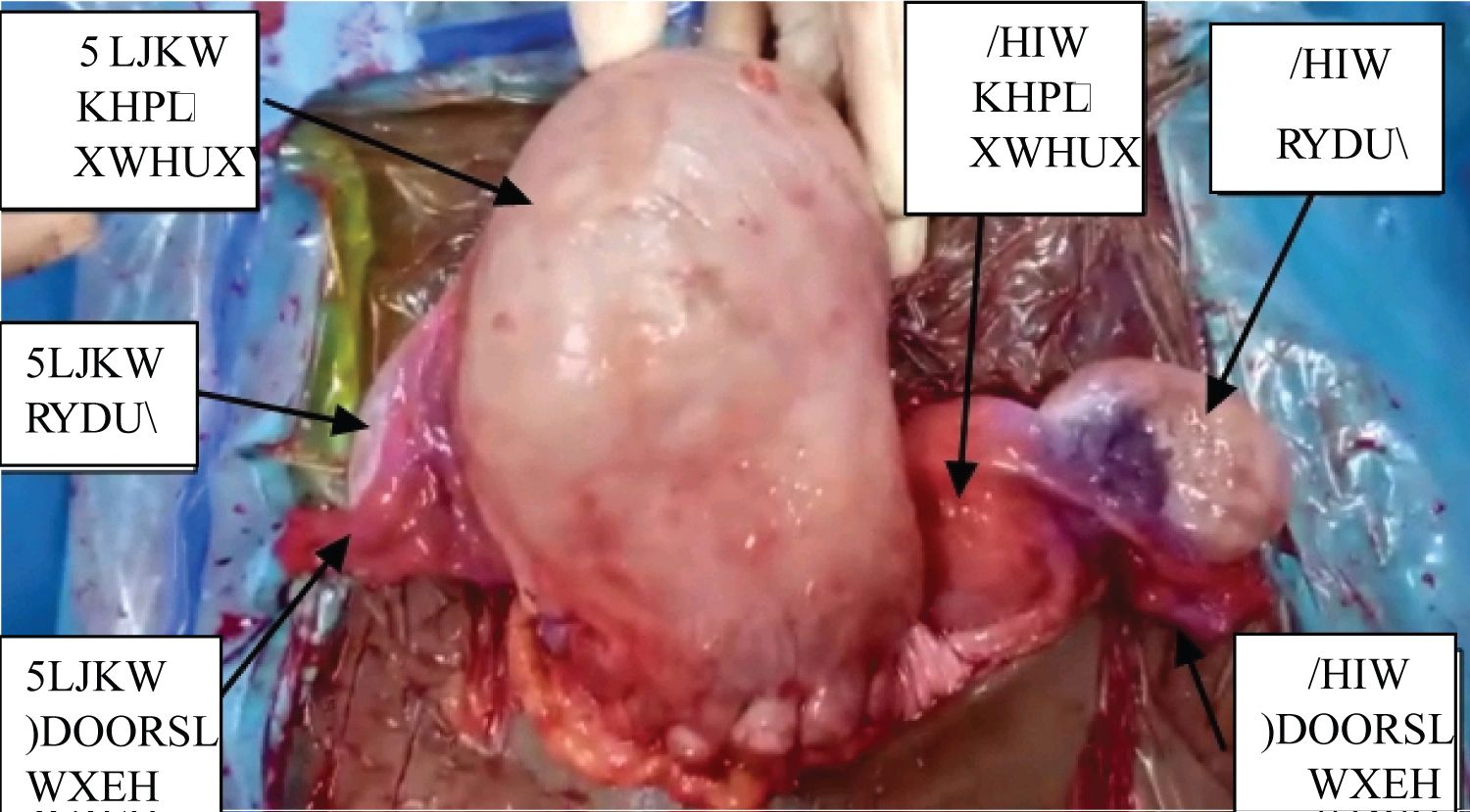 Figure 1: Two hemi-uteri (right and left), each carrying the homolateral adnexa.
View Figure 1
Figure 1: Two hemi-uteri (right and left), each carrying the homolateral adnexa.
View Figure 1
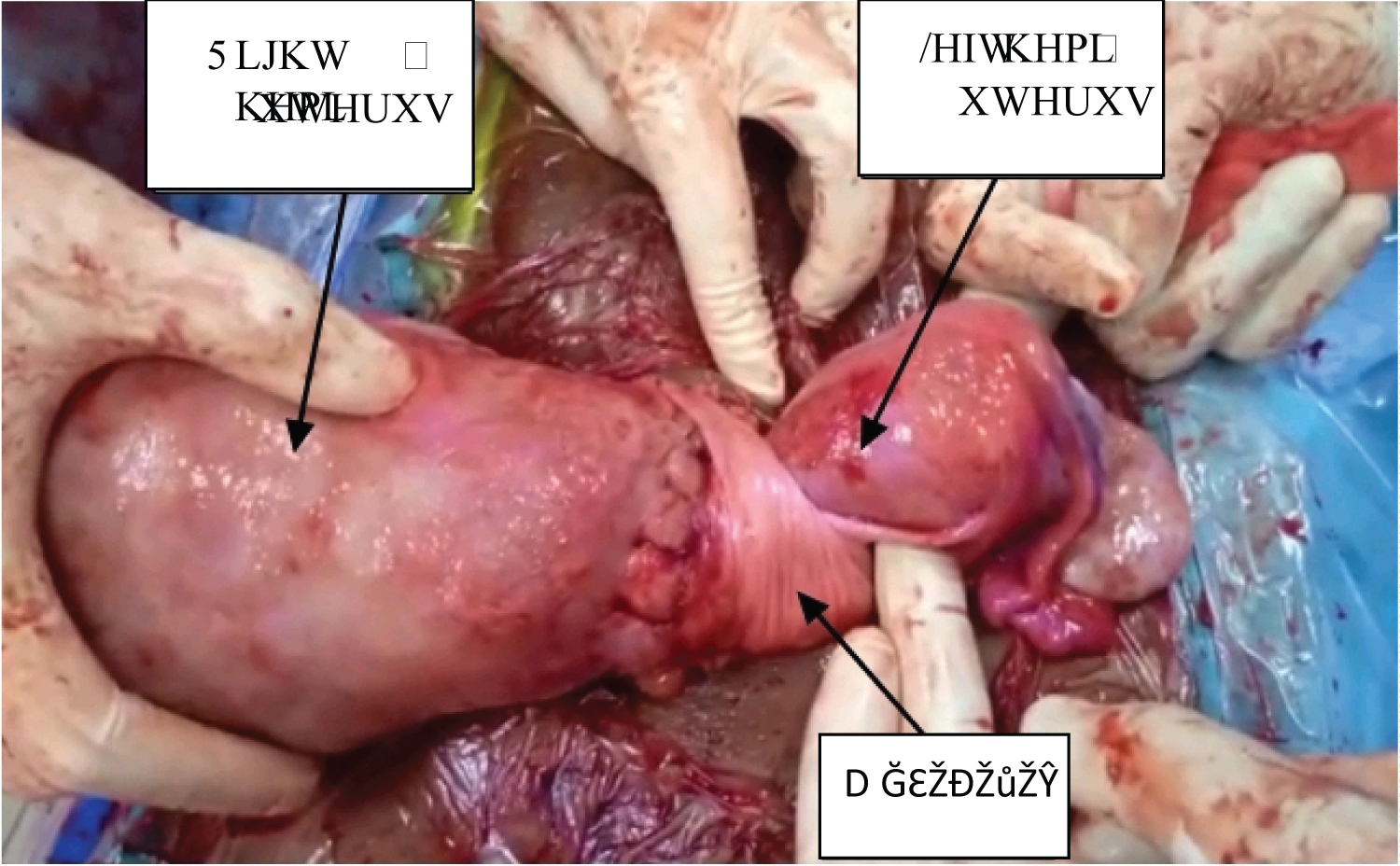 Figure 2: The two hemi-uteri crossed by the mesocolon at the junction zone.
View Figure 2
Figure 2: The two hemi-uteri crossed by the mesocolon at the junction zone.
View Figure 2
Mrs. N.M aged 29, a housewife, was referred to us from a 1st level health facility for premature rupture of membranes in a scarred uterus.
History taking revealed that she had been discharging fluid through her genital tract for 14 hours prior to admission, with no symptoms of pain or other associated signs. Her medical history was unremarkable. The surgical history was marked by a caesarean section in September 2020 for a double circular cord with a breech fetus.
The parturient was in her 4 th gesture, 2 nd pare including a vaginal delivery in September 2017, two live children and a miscarriage in 2016. The pregnancy was monitored by four antenatal consultations during which three obstetric ultrasounds were performed and no uterine anomalies were reported. Gestational age, estimated on the basis of the date of the last menstrual period, showed a pregnancy with an extended term of 41 weeks of amenorrhoea.
Her general condition was good and physiological vitals were normal.
Obstetrical examination revealed a gravid uterus with a uterine height of 34 centimetres. Fetal heart sounds were heard in the right lower left quadrant and counted at 158 beats per minute. The contractions were regular but spaced out and of short duration. Speculum examination revealed healthy-looking vaginal walls and cervix. Bonnaire's sign was positive. Vaginal examination revealed a short, soft, median cervix, dilated to 02 centimetres, a ruptured water sac and cephalic presentation. Tarnier's sign was positive.
Fetal heart rate recordings showed deep and late decelerations.
An emergency caesarean section was indicated and allowed extraction through the cephalic pole of a live male newborn weighing 2975 grams with a good APGAR.
After fetal extraction, we found a uterus with a single uterine horn and a healthy-looking right homolateral ovary and fallopian tube.
At the end of the operation, Mrs. N.M revealed that she had never been informed of the particular condition of her uterus, including at the time of her first caesarean section in September 2020.
The post-caesarean period was unremarkable and the mother and child were discharged on the 3 rd day (Figure 3).
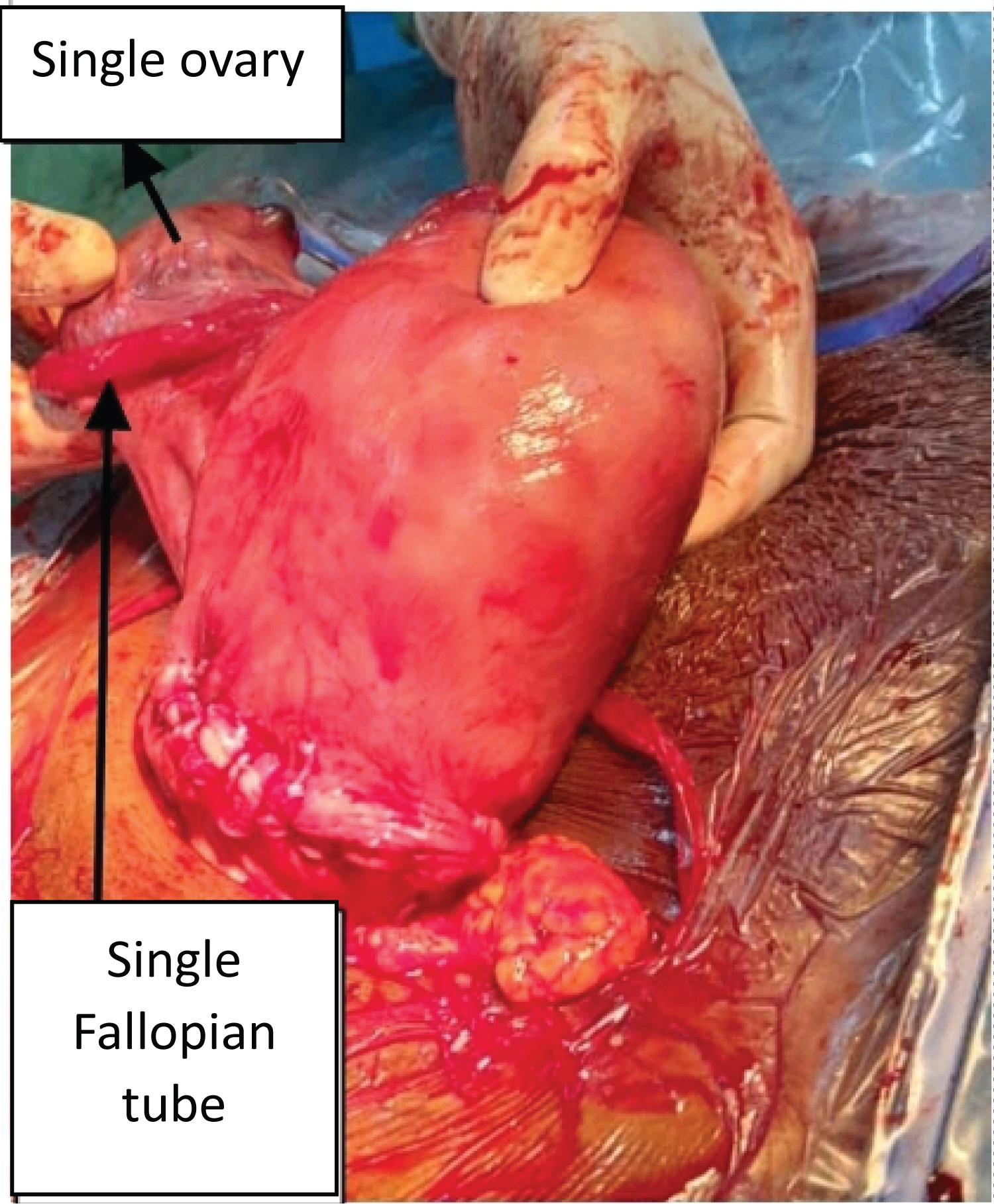 Figure 3: Unicorn uterus.
View Figure 3
Figure 3: Unicorn uterus.
View Figure 3
Congenital malformations of the uterus result from a structural anomaly during embryogenesis [6,7]. Their frequency varies according to studies and they are often the cause of infertility and repeated miscarriages [5]. However, they can be asymptomatic and are discovered by chance during radiological investigations or surgery [3,5,8], as in the case of our two parturients who were diagnosed during caesarean section. Pregnant women with uterine malformations can asymptotically carry their pregnancy to term and give live births in variable proportions depending on the type of anomaly. This represents 37 to 40% for unicornuate uteri and 62% for bicornuate uteri [9]. This is also the case for our pregnant women, whose pregnancies were carried to term.
They are subject to a higher risk of caesarean section because of the higher frequency of anomalies in foetal position [10]. The same applies to our parturients. Mrs. N.M, a carrier of a unicornuate uterus, underwent caesarean section for a breech fetus in a primigravida. Mrs. S.B, a carrier of a bicornuate unicervical uterus, underwent a caesarean section in 2020 for a double circular cord with a breech foetus. Low vaginal delivery is also possible [10]. This was the case for Mrs. S.B, who gave birth vaginally during her first delivery in September 2017. Certain types of congenital malformations interfere with a woman's sexual and reproductive life, requiring surgical management. Our two cases did not report any sexual problems. However, their obstetrical prognosis remains reserved because of the higher risk of miscarriage and dystocic presentation compared with the general population.
Congenital malformations of the uterus are relatively common, but many remain unrecognised because they are often silent. They can be a source of infertility and recurrent miscarriage. Pregnancies with a malformed uterus can sometimes progress asymptomatically to term. Delivery by the vaginal route is possible, but the risk of caesarean section is even higher than in the general population due to the high risk of abnormal presentation.