The purpose of this study was to review the current challenges that the diagnosis and clinical management of hyperextension of the fetal neck represent and to describe the clinical significance and differential diagnosis of this entity, detected by ultrasound prior to the onset of labour.
A case of hyperextension the fetal neck is presented. The key points in the diagnosis and management of fetuses with these sonographic finding are reviewed. Hyperextension of the fetal neck is a sonographic finding amenable to prenatal ultrasound diagnosis. The initial finding is a hyperextension, referred to the persistence of the cervical spine in extreme extension, with an extension angle of at least 150 degrees persisting for the duration of the scan.
The patient was referred to a reference hospital where an intrauterine septum was described and confirmed in week 21, with a less marked fetal hyperextension. After birth the Neonatal Pediatric service had difficulty passing nasogastric tube and a loop at the level of the upper third of the esophagus was observed in the chest radiography. She was transferred to a reference hospital for suspected oesophageal atresia that was confirmed and treated with surgery. Long term outcome was favorable.
The identification of a fetus with HFN should prompt a detailed search for structural abnormalities, although these may not all be identifiable prior to delivery. After birth, an oesophageal atresia was confirmed and treated with surgery with a favorable long term outcome. Persistent HFN can be associated with normal outcome as in this case. Prenatal counseling should be offered in case of suspected diagnosis.
Hyperextension, Fetal neck, Esophageal atresia, Prenatal diagnosis, Attitude
Hyperextension of the fetal neck (HFN) is among the various fetal attitudes detected by prenatal ultrasound. If the fetal head is presenting part, hyperextension leads to a face presentation. There are various etiologies for HFN. These include fetal anomalies such as structural abnormalities, conjoined twins, fetal neck masses and iniencephaly and nuchal cords. Polyhydramnios is probably secondary to either impaired swallowing or heart failure. Abnormal uterine factors, such as leiomyomata and uterine malformations may also lead to this finding. However, there is no etiologic factor identified in 75% of the cases. The importance of the precise prenatal diagnosis of this condition relates not only to delivery concerns but also to the detection of associated conditions, as noted above.
Diagnosing HFN is vital due to the increased risk of injury to the cervical spinal cord during delivery, especially when a vaginal breech delivery is anticipated [1-4]. Historically, it was not diagnosed until after the onset of labor [5]. With the advances in ultrasound technology, a hyperextended head or neck can be easily identified and the potentially associated fetal structural abnormalities as well as the intrauterine environment (amniotic fluid volume and placental position) can be evaluated.
Reports on the clinical significance of the antenatal diagnosis of HFN prior to labour are scarce [1,2]. The purpose of this study was to present a case and review the clinical significance, associated findings, and perinatal outcome.
We present the case of a primigesta after 3 cycles of in vitro fertilization (IVF) with normal first trimester ultrasound and 1.3 mm of nuchal translucency, no septum was observed. In week 19 a HFN was observed (187º), without other anomalies (Figure 1). The patient was referred to a reference hospital where an intrauterine septum was described and confirmed in week 21, with a less marked fetal hyperextension (Figure 2). At week 26 she maintained a fetal position in cervical hyperextension, although less obvious and early onset of intrauterine growth restriction (IUGR) with an estimated fetal weight (EFW) of 769 g (7 percentile). The uterine pulsatility index (Ut API) and the morphological tracking were normal. In placentation of normal pregnancies, the spiral arteries are invaded by endovascular trophoblast, resulting in extensive remodeling of these arteries. Because of this change, the uterine artery Doppler in normal pregnancies is characterized by low resistance and a high-flow pattern. However, in hypertensive pregnancies, incomplete trophoblast invasion results in an abnormal uterine artery Doppler pattern, which is characterized by an increased pulsatility index (PI) and an early diastolic notch.
 Figure 1: Hyperextension of the fetal neck observed at week 19 by 2D ultrasound.
View Figure 1
Figure 1: Hyperextension of the fetal neck observed at week 19 by 2D ultrasound.
View Figure 1
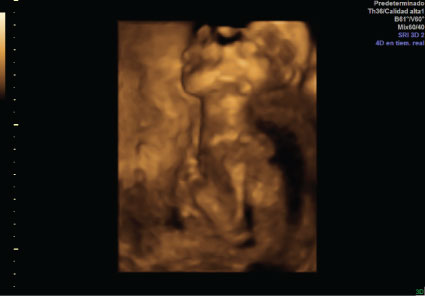 Figure 2: Hyperextension of the fetal neck observed at week 21 by 3D ultrasound.
View Figure 2
Figure 2: Hyperextension of the fetal neck observed at week 21 by 3D ultrasound.
View Figure 2
There was an amniotic bridle in the upper part of the uterine cavity. Amniotic band syndrome is a rare condition caused by strands of the amniotic sac that separate and entangle digits, limbs, or other parts of the fetus. This constriction can cause a variety of problems depending on where strands are located and how tightly they are wrapped. Amniocentesis and MRI were offered but she rejected. She had a fetal echocardiogram that was normal.
In week 29, a uterine septum was still seen. However, the hyperextension was no longer displayed. In week 32 the EFW was 1735 +/- 253 g (29 percentile) and the colon was discretely distended. In the 37 week the EFW was 2464 g (9 percentile), Amniotic fluid index (ILA) was 29 and she maintained hyperextension position intermittently. Assessment for neonatology service after childbirth was recommended.
Labor was spontaneous at 37 weeks. Delivery was instrumental; using a Kielland forceps applied for a distocia in left occiput posterior (LOP). The newborn was a female of 2360 g and APGAR test 9/10. The Neonatal pediatric service describes a bad facial coloration and choking crisis due to secretions. They had difficulty passing nasogastric tube and a loop at the level of the upper third of the esophagus was observed in the chest radiography (Figure 3). She was transferred to a reference hospital for suspected oesophageal atresia that was confirmed and treated with surgery.
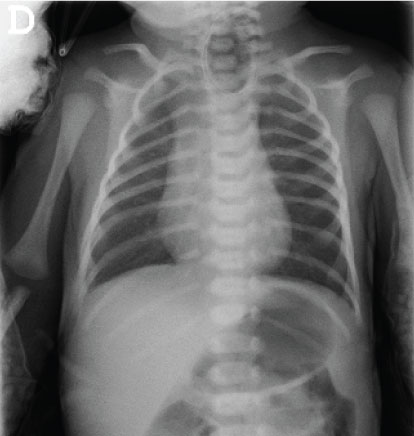 Figure 3: Type C depicts the blind pouch with gas noted in the stomach and intestine to identify a distal tracheoesophageal fistula.
View Figure 3
Figure 3: Type C depicts the blind pouch with gas noted in the stomach and intestine to identify a distal tracheoesophageal fistula.
View Figure 3
The prevalence of HFN has been noted to range from < 1 to 11%, depending on the criteria for diagnosis [1,3]. The evaluation of degree of HFN can be difficult, since a sagital view of the fetal spine is required. Ultrasound, however, allows the possibility of obtaining a lateral view of the fetal neck and head. Real time ultrasound is particularly adept at evaluating the attitude of the fetal head, and the identification of the hyperextension of the fetal head has been reported previously using this technique [4].
Although it has been reported that approximately 75% of cases of HFN have no identified etiological factor, the literature considers that cervical fetal hyperextension (> 150°) has a strong association with fetal structural anomalies and adverse neonatal outcomes. Some possible factors leading to this finding are maternal multiparity, premature delivery, placenta previa, uterine malformation or leiomyomata, abnormal presentation, multiple gestation, fetal anomaly, tumor of the fetal neck and nuchal cord [2]. Other associated etiologies are conjoined twins, anterior masses of the fetal neck (goiter, lymphangioma, teratoma, and anterior hygroma) nuchal cord, polyhydramnios, leiomimas, uterine malformations [5].
Prior literature concerning fetal head positioning primarily has been in that of assessing the singleton breech during labor. Although the positioning of the head has commonly been assessed subjectively in this population, angles of greater than either 90º from the thoracic spine to the mandible have been thought to indicate hyperextension of the fetal head [6]. It may be that the deflexed or extended head may be best represented by angles between 90º and 150º and those greater than 150º might best be represented with the term "hyperextended".
Cervical fetal hyperextension can be resolved as the pregnancy progresses and if so, it is associated with good neonatal outcomes. However, if it persists, it has a high association with structural anomalies and syndromes (Klippel-Feil syndrome with a failure in the segmentation of cervical vertebrae, Jarcho-Levin syndrome...). In most of the cases described in the literature, the Comparative Genomic Hybridization (CGH) Array study is normal, so we did not do it in our case because of the risk of fetal loss.
In our case, the new born was finally diagnosed of esophageal atresia (EA) with Tracheoesophageal fistula (TEF) after birth. Despite previous works claiming that approximately 75% of cesarean with hyperextension of the head have no identified etiological factor, Shipp, et al. found that malformations can explain approximately 40% of those with hyperextension of the head detected antenatally prior to labor [5]. The identification of a fetus with hyperextension of the head should prompt a detailed search for structural abnormalities. According to Phelan, et al., only four of the 21 fetuses with antenatally diagnosed abnormalities had abnormalities other than iniencephaly or conjoined twinning [6].
Deflexion of the fetal head has been classified into three types: Military, brow, and face presentation (mild, moderate and severe deflexion) [2]. The degree of hyperextension appears to influence the risk of birth injury to the fetus with a breech presentation delivered vaginally. Hyperextension of the neck in a fetus with a breech presentation is now considered an indication for cesarean section [7-9]. Cesarean section, however, is not completely preventative for neurological lesions. Permanent spinal cord injury has been reported for cesarea delivered via cesarean section for breech position with hyperextension of the neck [10,11]. There is also the suggestion that neurologic injury may occur prior to labour [12]. Our patient didn't have spinal cord injury.
TEF and EA are congenital anomalies in which an abnormal communication occurs between the trachea and the proximal and/or distal esophagus segments [13-15]. It is important to note that EA is a frequent anomaly and it can be present with or without a TEF [16]. There are various types of TEF/ EA based on the Gross classification, which is described below [13,17].
Type A - Pure EA: Absence of the esophagus with no fistula. Neither end of the esophagus is connected to the trachea.
Type B - EA with proximal TEF: Middle section of the esophagus is missing, and there is a fistula on the trachea from the upper end of the esophagus.
Type C - EA with distal TEF: Middle of the esophagus is missing, and the trachea is connected to the lower end of the esophagus with a fistula, as in this case.
Type D - EA with proximal and distal fistulas: Absence of a portion of the esophagus with fistula connections to the trachea from both the upper and lower portions of the esophagus.
Type E - H-type fistula: Esophagus is complete with a fistula on the trachea. There may be a narrowed area of the esophagus.
The worldwide prevalence of EA is 2.99 per 10,000 [15,17]. Sixty percent of newborns with EA will have coexisting anomalies, whereas half of those infants will have VACTERL association, which includes Vertebral anomalies (V), Anal atresia (A), Cardiac anomalies (C), Tracheoesophageal fistula (T), Esophageal atresia (E), Renal anomalies (R), and Limb anomalies (L) [18,19]. Eighty-six percent of infants with EA will have a distal TEF; 2% will have a proximal TEF; 7% will have no fistulous connection; and 4% will have TEF without atresia [20]. Infants with TEF/EA are 50% more likely to have congenital anomalies, with VACTERL being the most common association [21].
Advances in medicine and technology have made early prenatal counseling possible, which can improve postnatal outcomes. Routine fetal anatomy ultrasound scans that typically occur around approximately 20 weeks' gestation can detect congenital anomalies such as TEF and EA [21]. Polyhydramnios in the setting of small or absent stomach raises concern for TEF/EA, however, these ultrasound features can be nonspecific, subjective, and occasionally transient in nature.
The outcome of newborns with tracheoesophageal fistula (TEF) with or without esophageal atresia (EA) has improved considerably, with an overall survival rate of 85% to 95% [22]. The prognosis can significantly change when it is associated with anomalies, which can affect the quality of life. Acher, et al. [15] completed a survey to evaluate the long-term outcomes of patients with TEF/EA in a retrospective study. Regardless of the type of repair, occurrence of esophageal dysmotility, dysphagia, reflux, and strictures adversely affect the patient's quality of life [15].
While the incidence of TEF/EA may be minimal when compared to other congenital anomalies, there is a high incidence of VACTERL association, which can lead to significant morbidity. Recognizing early signs and symptoms of newborns with TEF/EA has the potential to expedite their medical management and transfer to a hospital where pediatric surgeons with expertise in and experience with TEF/EA are available. Delay in appropriate treatment can lead to poorer outcomes such as aspiration, gastric perforation, respiratory failure, and long-term complications.
With ultrasonographic advances, cervical fetal hyperextension can be easily identified and thus assess fetal structural or associated intrauterine environment anomalies as in our case the uterine septum. After birth, an oesophageal atresia was confirmed and treated with surgery with a favorable long term outcome. The identification of a fetus with HFN should prompt a detailed search for structural abnormalities, although these may not all be identifiable prior to delivery. Prenatal echography is a valuable tool in clinical decision making and treatment indications. Ultrasound allows not only prenatal diagnosis but also the detection of possible complications, that may affect management.MRI and echocardiogram should be offered.
In conclusion, the sonographic identification persistent HFN can be associated with normal outcome as in this case. It has a high association with structural anomalies and syndromes but the Comparative Genomic Hybridization (CGH) Array study is usually normal. Prenatal counseling should be offered and it remains a challenge because little information is available on the long-term development.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.