Herlyn-Werner-Wunderlich syndrome (HWHS) is a rare developmental anomaly of Mullerian ducts, characterized by the presence of a uterus didelphys with longitudinal vaginal septum obstructing the hemivagina and the presence of ipsilateral renal agenesis. It is a very rare syndrome with only a few cases that have been reported.
We describe, In this report, the clinical presentation and the successful surgical management of an 11-year-old girl who presented with acute lower abdominal pain and palpable tender mass in the lower abdomen. The diagnosis of Herlyn-Werner-Wunderlich syndrome was suspected by the ultrasonography and confirmed by the Magnetic resonance imaging (MRI). Successful management was done by resection of the vaginal septum using the Ligature device through the hymen opening. Awareness is necessary in order to diagnose and treat this disorder properly before the occurrence of complications.
Uterus didelphys, Vaginal septum, Renal agenesis, Herlyn-Werner-Wunderlich syndrome
The incidence of Mullerian duct anomalies in the literature is estimated to be from 0.5 to 5.0% in the general population [1,2]. Crosby and Hill in 1962 firstly described the theory of the development of Mullerian ducts [3]. During the embryonic period, The Mullerian ducts (paramesonephric) develop from the coelomic epithelium and grow caudally along the Wolffian ducts (mesonephric) toward the urogenital sinus forming the two uterovaginal canals. At the 11 weeks of gestation, the Mullerian ducts fused laterally to form a single canal which becomes the uterus and the upper tow third of the vagina [4]. Meanwhile, the sino-vaginal bulbs invaginate from the urogenital sinus and meet the caudal end of the fused Mullerian ducts to form the vaginal plate. Finally, the vaginal plate is reabsorbed and being canalized to form the lower part of the vagina. This process of resorption is completed by the 24 weeks of gestation. Defective of fusion, or failure of resorption of the inferior portions of the Müllerian ducts during early embryological life results in uterus didelphys (double uterus) or septated uterus. The vagina may be septated as well [5,6]. Uterus Didelphys occurred in about 0.16% of fertile women [7]. The coincidence of Renal agenesis on the same side of the obstructed vagina can be explained by an embryologic arrest at 8 weeks of pregnancy, simultaneously affecting the two neighbors: The Mullerian (paramesonephric) and Wolffian (metanephric) ducts [8,9].
Purslow CE in 1922, firstly described a case of a young woman with regular menstruation had gradually increasing pelvic pain and appearance of a pelvic mass after menarche [10]. MOSTYN P. and EMBREY B. in 1950 described a case of obstructed Hemi-vagina and a uterus didelphys as well as an ipsilateral renal anomaly [11]. While Herlyn and Werner in 1971 initially described the syndrome as blind hemi-vagina with ipsilateral renal agenesis [12], finally, Wunderlich in 1976 added the bicornuate uterus as a feature of the syndrome [13].
Nowadays, Herlyn-Werner-Wunderlich syndrome (HWW), represents a complex female genital malformation with uterus didelphys, unilateral low vaginal obstruction, and ipsilateral renal agenesis.
An 11-year-old girl, admitted to the pediatric surgery department complaining of an increasing lower abdominal pain. There was no associated symptom of vomiting, fever or diarrhea.
History revealed that the menarche had started 5 months back, the menses were regular every 30 days and the menstrual bleeding usually lasted 4-5 days. The last cycle was associated with mild lower abdominal pain.
On physical examination: Patient general conditions were stable, the pulse: 84 /m., BP: 110/80 mg and RR 20/min. Abdominal examination revealed tenderness on palpation of the lower abdomen with a vague tender mass occupying mainly the hypogastrium and the left lower quadrant of the abdomen. The mass was tense, cystic, regular arising from the pelvis and reaching to the umbilicus. Rectal examination revealed a tense, cystic mass was felt anteriorly and to the left side. Vaginal examination showed that the vulva are apparently normals and that the posterior vaginal wall is bulged through the left side by the swelling. Routine hematological and biochemical profile were normal.
Abdominal ultrasonography showed 5.7 × 8.0 cm mass posterior to the bladder connected to the uterus, filled with turbid fluid... Another uterine corn like a mass was seen along the right side of the pelvic mass. Features are suggestive of hematometra/hematocolpos with bicornuate uterus, two uterine bodies, and absence of the left kidney.
Pelvic MRI showed uterus Didelphis with two hemi-uteri and two hemi-vaginas, the left hemi-vagina was blind, (Figure 1), left hematometro-colpos, and hematosalpinx overlying the dome of the urinary bladder (Figure 2 and Figure 3), Also, it showed left renal agenesis (Figure 4).
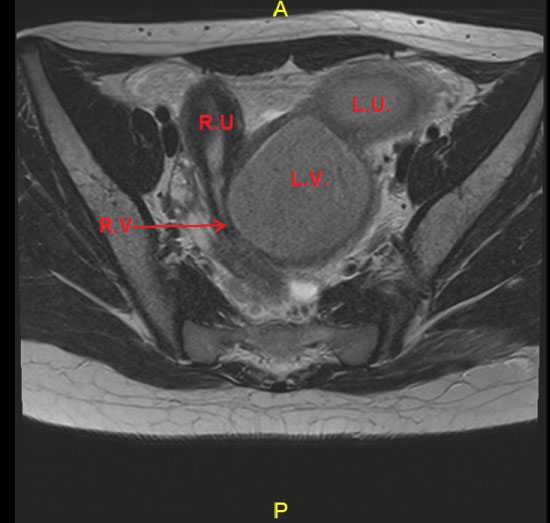 Figure 1: MRI image transverse cut.
Figure 1: MRI image transverse cut.
LU: Left uterus horne, Dilated; LV: Left vagina, Dilated; RU: Right uterus horne; RV: Right patent hemivagina.
View Figure 1
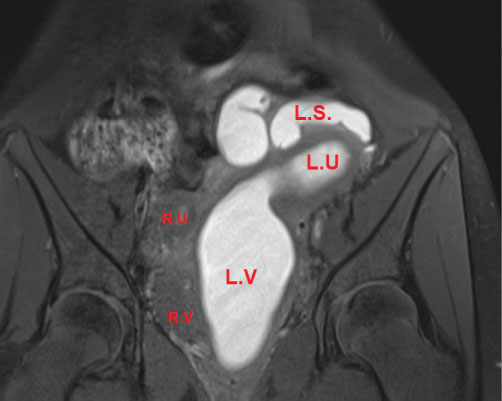 Figure 2: MRI image coronal view.
Figure 2: MRI image coronal view.
LU: Left uterus horne, Dilated (metrocolpos) >; LV: Left vagina, Dilated (Hematocolpos); LS: Left salpinx (hematosalpinx); RU: Right uterus horne; RV: Right vagina.
View Figure 2
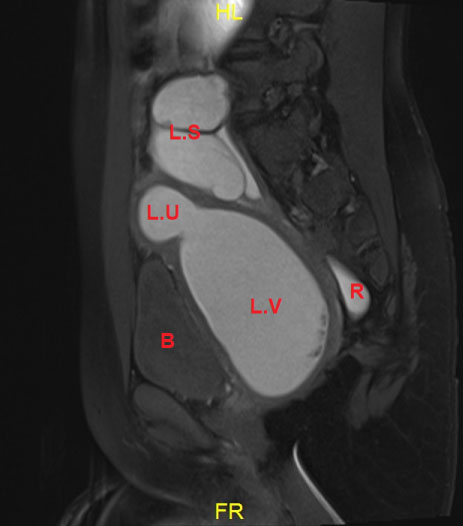 Figure 3: MRI image sagital view.
Figure 3: MRI image sagital view.
Showing the hemato metro-colpo-salpinx.
B: Bladder; R: Rectum.
View Figure 3
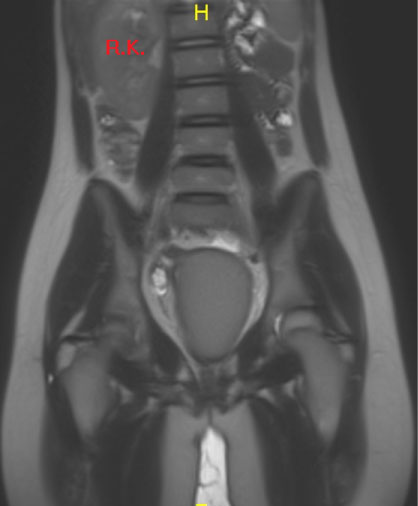 Figure 4: MRI image coronal view.
Figure 4: MRI image coronal view.
Demonstrating the absence of left kidney.
View Figure 4
The presence of associated renal agenesis conformed the diagnosis of Herlyn-Werner-Wunderlich (HWW) syndrome. The condition was explained to the family and the decision was made to perform a laparoscopic exploration followed by a vaginal exam under anesthesia followed by resection of the obstructed vaginal septum. Laparoscopic exploration showed the uterus Didelphis, the left-sided uterus and the left tube were significantly dilated, the right-sided uterus, tube, and both ovaries were normals (Figure 5) laparoscopic Peritoneal toilet with aspiration removal of the accumulated blood from the pelvis.
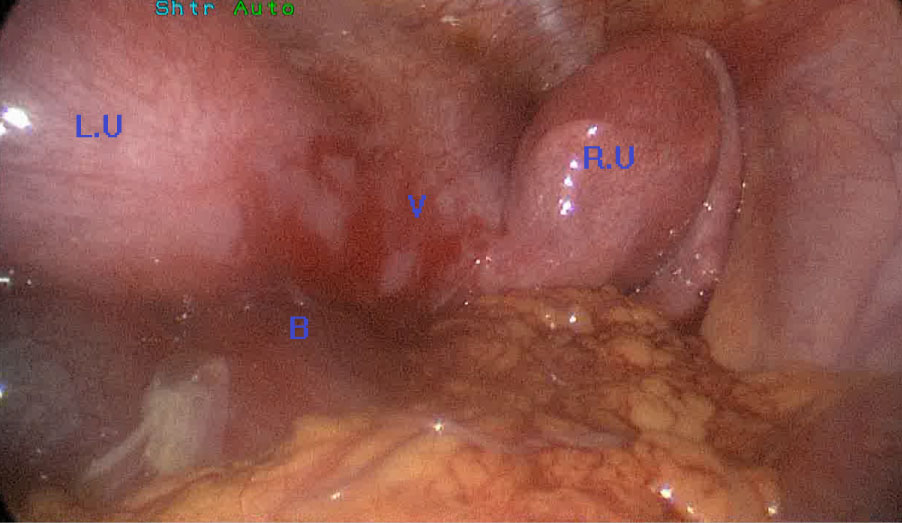 Figure 5: Laparoscopic view.
Figure 5: Laparoscopic view.
RU: Right uterus horne; LU: Left uterus horne; V: Vagina; B: Blood in the peritoneal cavity.
View Figure 5
With the patient in the lithotomy position, with speculum examination, the right hem-ivagina was compressed but patent, while there was a bulging from the left side. A puncture was made in the lower extremity of the bulging to identify the obstructed vaginal septum and aspiration was done with drainage of 200 ml of altered brown colored blood. Then the septum was incised with electrocautery, finally, The vaginal septum was widely excised until the cervix using the ligasure device. Postoperative was smooth, the patient was discharged on the 3rd postoperative day.
On OPD follow up, she was menstruating regularly, ultrasonography revealed that the size of the right uterus was reduced with the disappearance of the vaginal mass.
Patient with (HWWS) usually becomes symptomatic after menarche. Having two normal uterus and obstructed hemivagina, the patient will have regular menses through the non-obstructed vaginal side which coincides with a cyclic pelvic pain (dysmenorrhea) from the encumbered blood in the obstructed vaginal side, that leads to hematometra, hematocolpous and retrograde menstrual flow, which explains the increased prevalence of endometriosis, pelvic adhesions and retention of urine in these patients [14]. A ten years review of this anomaly showed that (73%) of patients presented with dysmenorrhea, (71%) with pelvic or paravaginal mass [15]. While In our case the presenting symptom was an acute abdominal pain resembling to acute abdomen, this type of presentation was also reported by Aydin R who stated that the acute abdomen presentation is uncommon [16].
Lan Zhu, et al. proposed New Classification of Herlyn-Werner-Wunderlich Syndrome based on a complete or incomplete obstructed hemivagina [17] according to this classification, the hemivagina in our case was completely obstructed.
Diagnosis of HWWS is usually confirmed by sonography and magnetic resonance imaging (MRI). Sonography can detect the pelvic cystic mass and may detect the uterine malformations, however Some authors now consider MRI as the gold standard for the diagnosis, as it provides more detailed information regarding the uterine contour, the shape of the intrauterine cavity and its continuity with each vaginal lumen, the character of the septum, and the nature of the fluid content, as well as the presence of the associated aspects such as endometriosis, or renal anomalies [18,19]. In our case, the ultrasonography was done in an emergency base, and then the MRI images clarified the exact uterine abnormalities and made the diagnosis of the case clear.
Many associated Urological malformations have been described with HWWS including, renal duplication, multicystic dysplastic kidney and renal agenesis which is the most commonly reported associated urologic anomaly [20,21]. In our case the absence of the right kidney in association with the other abnormalities have confirmed the diagnosis of HWWS.
The optimal treatment in such case is full excision and marsupialization of the obstructing vaginal septum allowing both uteri to drain through the patent vagina [22]. In our case we have performed a full excision of the vaginal septum using a ligature devise which could be introduced through the hymen opening without disturbing its integrity, which is an important factor for the community.
Fedele L, et al. in a report of 87 cases of HWWS revealed that 72.4% of cases were of classic variety and 27.6% of cases were variants of uterine septum or cervical agenesis [23]. In this type of variety of the syndrome, where the unilateral obstruction is at the level of cervix, Himadri Bal, performed Unilateral subtotal hysterectomy with salpingectomy [24].
Laparoscopy may not be mandatory in the treatment of HWWS, but it could be helpful in confirming the diagnosis when radiological imaging is inconclusive. Also, laparoscopy is useful in the diagnosis and treatment of endometriotic lesions and to release pelvic adhesions resulting from retrograde menstruation from the obstructed hemivagina [25], in our case the laparoscopy was useful to aspirate the intraperitoneal retrograde menstruation which was accumulated in the peritoneal cavity, and cleaning the abdominal cavity aiming to prevent future formation of endometriosis.
The potential complications of this syndrome are pyohematocolpos or pyosalpinx, which may lead to pelvic peritonitis. While long‑term complications are endometriosis, pelvic adhesions leading to chronic pelvic pain, and infertility. Which require early diagnosis and treatment of this syndrome in order to avoid theses complications and to preserve the fertility [26]. Wherefore patient affected by (HWWS) needs further follow up to predict these possible complications.
Herlyn-Werner-Wunderlich syndrome is a rare urogenital congenital anomaly. The aim of reporting this case is to highlight the entity and the importance of early management to relieve the symptoms and to prevent the complications, since timely diagnosis requires a high index of clinical suspicion and radiological confirmation.