Case report of a 33-year-old G5P3+1SA diagnosed with an intrauterine foetal death at 36 weeks gestation and induction of labour started with 400 ug of misoprostol vaginally, which was complicated by a uterine rupture with subsequent referral and management in our facility. Intra-operative findings during laparotomy revealed uterine rupture with a macerated still birth intra-abdominally and moderate hemoperitoneum.
Uterine rupture in an unscarred uterus following unsuccessful induction is an adverse effect that needs to be monitored and also requiring high index of suspicion to be diagnosed. A missed diagnosis of a uterine rupture during induction of labour could result in maternal mortality due to shock from severe hemoperitoneum.
Incidence of uterine rupture following misoprostol induction is rarely recorded due to its use in gynaecological practice which has been off label, hence there is need to document this occurrence experienced in our facility.
Unscarred uterine rupture, Uterine rupture, Abdominal pregnancy, Stillbirth, Hemoperitoneum, Induction of labour
Induction of labour is a common obstetric intervention and world-wide, 20-30% of deliveries are induced [1]. Options for pharmacological induction are prostaglandin E1, E2, F2 analogues and oxytocin drips. Misoprostol a prostaglandin E1, has been a long-standing agent for induction with lack of sufficient statistical evidence to measure its rare and serious side effects such as uterine rupture, bleeding, failure and uterine hyper-stimulation. Indications for induction of labour include hypertensive disease in pregnancy, prolonged pregnancy of more than 41 completed weeks, prelabour rupture of amniotic membranes and intra-uterine foetal deaths [2].
Uterine rupture may be primary occurring in a previously intact or unscarred uterus or secondary with an associated pre-existing myometrial incision, injury or anomaly [3]. Uterine rupture following induction with misoprostol is a rare side effect and its development is not dose related since even the use of small doses on an unscarred uterus can lead to uterine ruptures. Incidence of uterine rupture varies from 0.3/1000 to 7/1000 deliveries in India accounting for 5% to 10% of all maternal deaths and a perinatal mortality of 75% to 93% [4,5]. In developed countries, increased risk of uterine rupture and perinatal death are common among women with previous caesarean section and rarely in unscarred uteruses. The situation is however different in developing countries as the major causes of uterine rupture are obstetric complications, teen-age mothers with cephalo-pelvic disproportion, unsupervised labour and poor socio-economic status. Other risk factors for uterine rupture include grand multi-parity, use of uterotonic drugs to induce or augment labour, obstructed labour, malpresentation, placenta percreta and rarely intrauterine manipulations such as internal podalic version and breech extraction. In developing countries the incidence ranges from 1 in 250 to 1 in 5,000 deliveries often originating from rural areas with poor antenatal care, socio-economic factors, and cultural practices. Incidence of uterine rupture recorded in Ghana is 1 in 124 (0.8%), comparable to data from Uganda (0.76%), Pakistan (0.74%), Nepal (0.9%) and Ethiopia (2.8%). Sites of uterine rupture may be areas of previous scars but for an unscarred uterus either lateral, fundal or posterior [6].
Signs and symptoms of uterine rupture post-induction are nonspecific which makes diagnosis difficult and sometimes delays definitive surgical management thus identifying high-risk pregnancies and timely referral is important in secondary prevention [7]. In high risk patients, continuous cardiotocograph monitoring is useful to detect rupture as the earliest sign to be picked up is abnormal foetal heart rate pattern in addition abdominal ultrasound can also detects breach in uterine layers, hemoperitoneum and extrusion of foetus and placenta outside uterine cavity [5]. Very few patients may present with the classical onset of severe abdominal pain, cessation of uterine contractions, absence of foetal heart rate, vaginal bleeding, palpable foetal parts on abdominal exam and maternal shock and therefore uterine rupture should be looked for with a high index of suspicion [4].
A study conducted by Nguefack, et al. in a hospital in Cameroon, recorded uterine ruptures in 71% of cases of labour induced by misoprostol [8-12]. Management of the Uterine rupture involves resuscitation, rapid transfer to theatre for exploratory laparotomy with hysterectomy or repair of the rupture depending on the clinical circumstances and condition of the patient.
A 29-year-old female G5P3+1SA was referred from a peripheral hospital on account of foetal death at 36 weeks of gestation. The Patient who lives in a farming community, was not a regular attendant to Antenatal clinic, booked at 34 weeks in her usual state of health till her third visit when she presented with inability to perceive foetal movements. Examination revealed a SFH of 28 cm with absent foetal heart rate, breech presentation and cervical 1 cm dilated. On admission to the peripheral hospital, labour was induced with 400 ug misoprostol per vaginum with initiation of labour within 4 hours. However, after 36 hours, patient had still not expelled and complained of contractions aborted, palpitations, fever, chills, dizziness, vomiting, absolute constipation but no bleeding per vaginum hence referred as a case of intestinal obstruction in cyesis.
On reporting to our facility, patient was febrile with a temperature of 37.8, pale but well hydrated, normal chest findings, pulse 142 bpm and Blood pressure of 151/98 mmHg. Abdominal examination revealed a distended abdomen, soft and generally tender. Uterus was not well palpable and foetal heart sound absent.
Bedside ultrasound scan findings are shown below of an empty uterus with thickened endometrium, a foetus about 21 weeks 4 days without cardiac activity seen within the abdominal cavity. A diagnosis of a uterine rupture post-misoprostol induction was made and patient was optimised for a laparotomy.
A plain abdominal radiograph done showed central and peripheral dilated loops of bowel with a facial imprint of the foetus. A rare finding given that abdominal radiographs are not routinely done during pregnancy (Figure 1).
 Figure 1: Abdomino-pelvic ultrasound scan showing intra-abdominal foetal death.
View Figure 1
Figure 1: Abdomino-pelvic ultrasound scan showing intra-abdominal foetal death.
View Figure 1
Laparotomy was carried out with intra-operative findings of 1,200 mls of altered blood intraperitoneally with a 1.5 kg macerated female stillbirth. Inspection of the bulky uterus revealed a 6 cm laceration of the left lateral uterine wall with disruption of the left broad ligament. Repair of uterine laceration was done followed by copious lavage of abdomen and layered closure (Figure 2).
 Figure 2: Plain abdominal radiograph showing facial imprint.
View Figure 2
Figure 2: Plain abdominal radiograph showing facial imprint.
View Figure 2
The post-operative period was uneventful and patient was discharged on the 5th post-operative day. She was subsequently reviewed postnatally and had no complaints, subsequently scheduled and consented for a bilateral tubal ligation as permanent contraception due to the weak uterine scar which predisposes her to spontaneous ruptures in subsequent pregnancies (Figure 3).
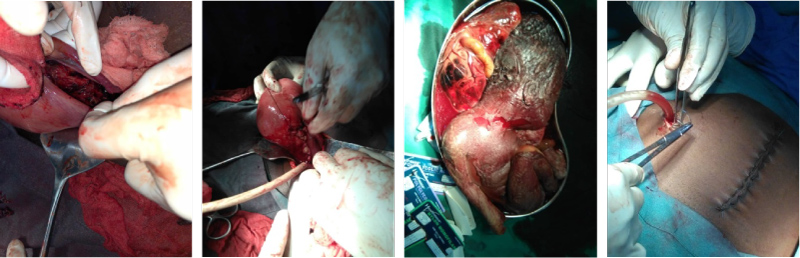 Figure 3: Intra-operative findings.
View Figure 3
Figure 3: Intra-operative findings.
View Figure 3
A key factor for averting mortality following uterine perforation after induction with misoprostol is early detection due to high index of suspicion. In a case report by Jonathan P, et al. where a maternal death was recorded, avoidable factors identified were delay and difficulty making the diagnosis due to the absence of risk factors for uterine rupture. Fortunately in our case maternal mortality was prevented due to early detection and intervention. Strict monitoring and high index of suspicion is required to detect and promptly intervene during uterine ruptures. Ultrasonography is a useful tool in antenatal diagnosis of spontaneous uterine rupture with sonographic findings of extra-peritoneal hematoma, intrauterine blood, free peritoneal blood, an empty uterus and a large uterine mass with gas bubbles suggestive of rupture [13].
In our case, ultrasound findings of an empty uterus with an intra-abdominal foetus was confirmatory of the rupture. Jonathan P, et al. in their case report observed that the uterine rupture occurred at the low posterior aspect without expulsion of the foetus drawing conclusion that a low posterior rupture does not give sufficient space for the foetus to be expelled outside the uterus, unlike our patient who had a left lateral rupture and subsequent expulsion of foetus. Studies however show that the anterior uterine wall was the most common site of ruptures noted in 48.4% of scarred uterine ruptures and 50% of unscarred uterine ruptures in a study by Al Salem MH, et al. and in 57.4% in a study by Gessesse A, et al. and 60% of cases in a study by Rizwan N, et al. [14,15].
The dose of misoprostol associated with tachysystole and uterine ruptures has been controversial since its use in induction of labour is an off-label use since as a prostaglandin analogue is prescribed for gastric acid hyper-secretion. Chuck FJ, et al. in their study noticed that tachysystole was known to be associated with labour induction using prostaglandins and that at a dose of 50 ug there was a higher incidence of tachysystole. This occurred most commonly after the second dose with a cumulative drug effect. This hyperstimulation can result in uterine ruptures [16]. The total dose administered to the case presented was 400 ug which was several times more than the 50 ug associated with tachysystole.
In a study conducted by Sahu L in India, 73.12% of patients who had uterine ruptures were within the age group of 20-30 years whilst a study by Sunitha K, et al. observed the majority within 26-30 years [17]. Since our patient fits into the age ranges, there is no deviation from other studies and more monitoring is required for such patients if induction of labour is commenced. Moreover our index case had no other risk factors for uterine rupture but since she was administered vaginal misoprostol to effect uterine evacuation of a dead foetus, we can conclude that the uterine rupture was a complication of the induction.
The definitive management for a uterine rupture is laparotomy after resuscitation with whole blood transfusion. The decision as to whether a hysterectomy is necessary or whether the uterus can be repaired and saved is made intra-operatively, based on stability of the mother, extent of damage to the uterus and whether the mother desires to have additional children [18]. In the above case, pre-operative diagnosis was an abdominal pregnancy with intestinal obstruction hence consent hadn't been gotten for a hysterectomy and the 6 cm laceration was not actively bleeding and linear hence the option for a uterine repair was made. In a study however, it was observed that though hysterectomy was initially thought to be the best treatment for uterine rupture, most physicians now try to repair the uterus if possible [18]. The risk of a re-rupture was documented to range from 4 - 19%, therefore patients need to be counseled regarding the high risk with option of permanent sterilisation or a scheduled C-section for future term pregnancies [19-21]. In our patient, she opted for a permanent sterilisation so bilateral tubal ligation was done for her.
Induction of labour is an essential procedure in obstetric care but has its risks requiring close monitoring to promptly detect. Studies by WHO have revealed that in developed countries, up to 25% of all deliveries at term now involve induction of labour whilst the rates are generally lower in developing countries [22]. To avert these risks of uterine ruptures associated with induction of labour especially from misoprostol, it is essential to adhere to the standardised protocols of labour induction.
Evidence support the fact that oral misoprostol 25 ug 2 hourly is recommended for induction of labour but avoided in previous caesarean section patients. Commercially produced misoprostol comes as 200 ug hence it is recommended to dissolve it into 200 ml of water and 25 ml administered as a single dose instead of breaking up the tablet. As soon as the patient experiences 2 regular, moderate contractions per 10 minutes, stop the misoprostol and do a CTG for 30 minutes as well as assess the cervix if viable foetus present. If favourable for rupture, perform artificial rupture of membranes and allow labour to progress. Low doses of vaginal misoprostol 25-50 ug 6 hourly is recommended for induction of labour. Prostaglandin E2 analogues are preferred due to low risks of uterine rupture.
During induction of labour, strict monitoring is required to identify complications such as uterine rupture which would require surgical repair or hysterectomy to avert maternal mortality.