Transversus abdominis plane (TAP) block is an important component of multimodal analgesia after abdominal hysterectomy to help with postoperative pain control. Our study evaluates 24-hour postoperative opioid consumption after TAP block in abdominal hysterectomy.
Retrospective study of 174 women who underwent abdominal hysterectomy at a single institution. Statistical analyses compared demographic variables, compared opioid consumption and pain score distributions, assessed the association between covariates and opioid consumption, and examined opioid consumption in non-patient controlled analgesia (PCA) users.
93 (51.1%) women received a TAP block. TAP block patients consumed 50% fewer opioids than No-TAP block patients (48 MME vs. 96 MME, P < 0.01). After exclusion of PCA patients, TAP block patients were between 2 and 8 times as likely as No-TAP block patients to be in the lower morphine usage group vs. the medium and higher usage groups, respectively (P < 0.01).
TAP block is an effective modality for postoperative pain control after abdominal hysterectomy.
Transversus abdominis plane block, TAP block, Hysterectomy, Postoperative pain
Hysterectomy is one of the most common surgical procedures in women. Between 2010 and 2013, there were 386, 226 hysterectomies in the United States [1]. Although the proportion of minimally invasive hysterectomies has increased over the last decade, the abdominal technique comprises of almost one-third of all hysterectomies [1].
Opioids remain one of the main analgesic treatments after abdominal hysterectomies, as well as abdominal surgeries in general. The side effect profile includes sedation, nausea, vomiting, constipation and ileus, all of which theoretically can prolong a patient's hospital stay. Opioid use disorder has increased costs not only of the health care system but also of the justice courts and workplaces. Such associated costs have increased from $11.8 billion in 2001 to $78.5 billion in 2016 [2,3].
One of the most feared consequences of opioid use is its potential for dependence and addiction. Our institution is located in Connecticut, which is among the top ten states with the highest rates of opioid-related overdose deaths. In the early 2000s, the death rate in Connecticut bordered near the national average. Through 2016, there was a fourfold increase, from 5.7 deaths per 100,000 persons to 24.5 deaths per 100,000 persons. This is in stark contrast to the national average of 13.3 deaths per 100,000 persons [4].
In order to optimize patient recovery, multimodal, opioid-sparing analgesic regimens have been established. One of the components of such regimens is a peripheral nerve block, including transversus abdominis plane (TAP) block. The abdominal wall sensory afferent nerves travel through the plane superficial to the transversus abdominis muscle, which contributes to the postoperative pain from the abdominal wall incision after hysterectomy [5].
The efficacy of the TAP block has been demonstrated in women undergoing abdominal wall surgeries, including cesarean delivery, open inguinal hernia repair, cholecystectomy, bowel resection and hysterectomy [6-12]. Published studies have evaluated TAP block efficacy in controlling postoperative pain as measured by pain scores and analgesic consumption, including opioids, as well as by presence and intensity of side effects.
With the TAP block becoming more ubiquitous in recent years, its utilization at our institution for gynecologic surgery started in 2015. We reviewed and analyzed our experience with management of postoperative pain control in gynecologic surgery since the inception of TAP block at our hospital. We hypothesized that women who received a TAP block following abdominal hysterectomy will have lower post-operative opioid consumption and pain scores compared to women who did not receive a TAP block.
This was a retrospective cohort study of women who were treated at a single institution between April 2015 and December 2016. Our institution is a 456-bed teaching hospital. Any woman at least 18 years of age who underwent an abdominal hysterectomy during this time period was included. Women were excluded if they had a chronic pain disorder, current or history of opioid dependence as documented in the medical record. Inpatient electronic medical records were queried for demographic and clinical data. Data was recorded in an encrypted, password-accessible only database. Author A.S.M. performed the data collection, and author E.P. validated the accuracy of database through a separate, second review.
Recorded patient demographics included age, body mass index (BMI), whether TAP block was used, type of surgery, whether staging was performed, incision type (Pfannenstiel, vertical), duration of surgery, pathology, epidural, and patient controlled analgesia (PCA). Total postoperative opioid consumption up to 24 hours as calculated in oral morphine milligram equivalent (MME) were recorded. Pain scores postoperatively based on a 10-point visual analog scale at 1 hour, 2 hours, 4 hours, 8 hours, 12 hours, 24 hours were also recorded.
The surgeon was either a general gynecologist or a gynecologic oncologist. An anesthesiologist administered all TAP blocks postoperatively in a bilateral two-quadrant manner under ultrasound guidance.
Demographic variables were compared by study group (TAP block and No-TAP block). The independent samples t- test was used to compare mean values for age, BMI, and surgery duration. Pearson's chi-square tests were used to compare proportions for surgery type, malignancy, incision type and PCA status.
For our primary outcome of opioid usage in morphine milligram equivalent (MME) and secondary outcomes of pain scores at 1, 2, 4, 8, 12 and 24 hours postoperatively, we used Wilcoxon rank-sum test to compare the distributions by study group and PCA status. We also calculated a 24-hour average pain score for each patient and compared using the Wilcoxon rank-sum test.
Multivariate analysis was conducted using multinomial logistic regression (generalized logit) model to assess the association between the opioid usage and the covariates. All variables were considered for inclusion in the model. Final covariates were TAP block, malignancy, PCA usage, and the 24-hour average pain score.
The significance criterion was set at P < 0.05. Statistical analyses were performed using SAS 9.4 (SAS, Inc., Cary, NC, USA) programming language.
BRANY Institutional Review Board File #17-08-62-337(c17) was approved on February 16, 2017.
A total of 174 women were included in this study with 93 (51.1%) who received a TAP block. Among the demographic and clinical variables assessed, only PCA status was statistically significantly different between the TAP block and No-TAP block groups (p < 0.01) (Table 1). Eight out of 93 women who received a TAP block also had a PCA device compared to 40 out of 81 women who did not receive a TAP block had a PCA device. Surgery type, duration of surgery, pathology (benign vs. malignancy) and incision type were not statistically significantly different between TAP block and No-TAP block groups. The majority of all patients had a midline vertical incision (75.9%) compared to Pfannenstiel incision (24.1%).
Table 1: Demographic and clinical information: TAP block and No-TAP block. View Table 1
For the primary outcome of 24 hours postoperative opioid consumption, TAP block patients had a 50% reduction in opioid usage compared with the No-TAP block patients (median of 48 MME vs. 96 MME, respectively; P < 0.01). For the secondary outcome of pain scores, there was no statistically significant difference between TAP block and No-TAP block groups in the 24-hour average pain score (4 vs. 3, respectively; see Table S1 for hourly data). Women in the PCA group tended to have high morphine use over 24 hours postoperatively compared to non-PCA users (median 134 MME vs. 52 MME respectively; P < 0.01, data now shown).
Table s1: Detailed pain scores by tap block and PCA status. View Table S1
Since the distribution of opioid usage was skewed, tertiles of MME equivalents were formed by consecutively ordering the MME for all patients and dividing into thirds: Higher usage, medium usage, and lower usage were examined by study group. Univariate comparisons show statistically significant differences between groups across tertiles (Figure 1). We fitted multivariate models to check the association between opioid consumption and TAP block status while adjusting for pathology, 24-hour average pain score, use of PCA, which showed significant marginal associations with opioid consumption (Table 2). Compared to No-TAP block patients, TAP block patients were 4.5 times more likely to be in the lower morphine usage group vs. the higher usage group, and almost 3 times as likely to be in the medium usage group as the higher usage group (P = 0.01).
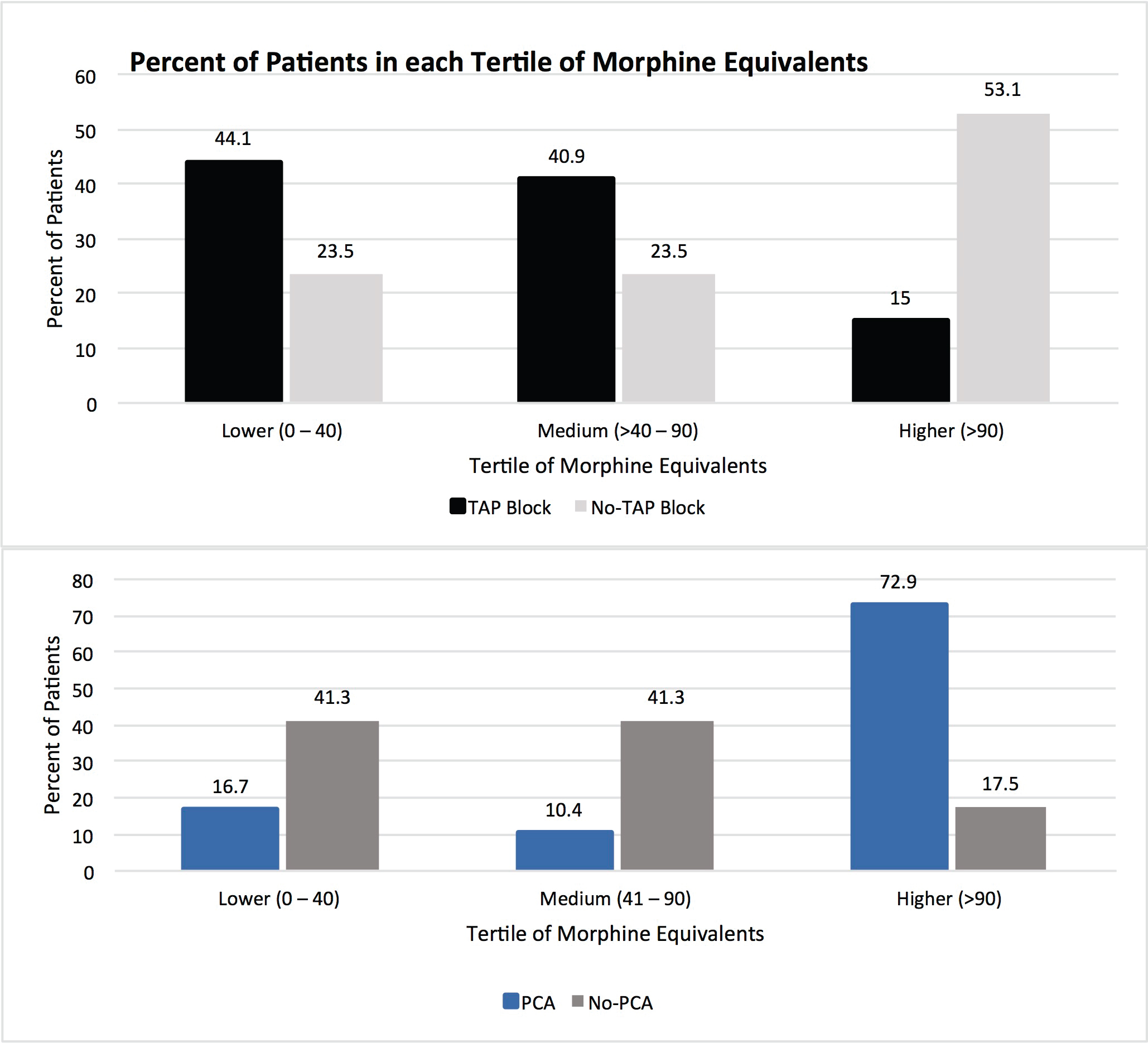 Figure 1: Percentage of women in each tertile of morphine equivalents.
View Figure 1
Figure 1: Percentage of women in each tertile of morphine equivalents.
View Figure 1
Table 2: Multinomial logistic regression predicting usage of morphine milligram equivalents. View Table 2
Women who experienced more pain over the 24 hours postoperatively were more likely to use morphine. For each point higher on the pain scale (average pain over 24 hours), patients were approximately half as likely to be in the lower morphine usage group (OR = 0.42). For PCA patients, the odds of being in the group of high morphine usage vs. low morphine usage was 25 times higher than the non-PCA users (OR = 1/.04 = 25, P < 0.01).
Given that there was a statistically significant difference in PCA between TAP block and No-TAP block patients, a second analysis examined opioid usage among non-PCA users. After excluding the 48 PCA patients, the opioid usage by study group was assessed using multinomial logistic regression (generalized logit) with covariates malignancy and 24-hour average pain score (Table 3). Among the non-PCA users, TAP block patients were between 2 and 8 times as likely as No-TAP block patients to be in the lower usage group vs. the medium and higher usage groups, respectively (P < 0.01).
Table 3: Multinomial logistic regression predicting usage of morphine milligram equivalents among Non-PCA users. View Table 3
At our institution, we demonstrated that opioid consumption was reduced by 50% after TAP block in abdominal hysterectomy patients 24 hours postoperatively. After excluding PCA users, women continued to experience more pain over 24 hours postoperatively and therefore were more likely to use morphine. These data coincide with prior studies evaluating opioid consumption after hysterectomy comparing TAP block with placebo. In a 2011 systematic review and meta-analysis, 11 randomized controlled studies evaluated TAP block in gynecologic surgery, and only five of these studies assessed abdominal hysterectomy. Similar to our data, 24 hours morphine consumption was reduced after TAP block [8]. One study showed TAP block reduced morphine requirement for each 12 hourly interval up to 48 hours after hysterectomy [9]. In a more recent 2019 systematic review and meta-analysis of TAP block and hysterectomy, five studies evaluated opioid consumption after abdominal hysterectomy [13]. In this subset, there was a mean difference of -9.53 mg of 24 hour morphine consumption in the TAP block groups.
In 2012, U.S. health care providers ordered more than 259 million prescriptions for opioids, twice as many as in 1998 [14]. There is an urgent need to identify new practices that help reduce the need for narcotics. Our data, combined with those of other studies, suggest that TAP block should be used as standard of care in abdominal hysterectomy as it significantly reduces the need for postoperative narcotics.
Additional approaches have also been identified as beneficial including enhanced recovery after surgery (ERAS) principles, such as scheduled non-narcotic medications and multimodal analgesics. Their benefits have been well studied in colorectal patients and are now demonstrated in gynecologic oncology patient populations [15-19]. For example, ERAS patients receive acetaminophen and gabapentin immediately preoperatively. Postoperatively, high dose acetaminophen and ibuprofen are administered on a schedule, as opposed to an as needed basis.
At our institution, TAP blocks are given with bupivacaine hydrochloride admixed with dexamethasone and performed postoperatively under ultrasound guidance. Other studies have evaluated the use of liposomal bupivacaine, which is composed of a suspension of multivesicular liposomes that carry bupivacaine. These liposomes gradually release bupivacaine in immediately surrounding tissues, allowing for analgesia over a longer period of time up to 96 hours [20,21]. Studies have demonstrated its effectiveness compared to bupivacaine alone in minimally invasive hysterectomy [22-24]. There is limited published data evaluating liposomal bupivacaine in open hysterectomy and therefore is a potential area of future research.
The observational, retrospective nature of the study presented several limitations. First, our study relied on documentation in the electronic medical record. There is an inherent selection bias with such a retrospective cohort study. However, both TAP and No-TAP block groups included benign and malignant pathology. Although many randomized controlled trials have been published since the completion of our study, our study addresses the limitations of those studies by including malignant pathology and excluding minimally invasive hysterectomy.
Second, our cohort included mostly women with vertical incisions in anticipation for potential surgical staging. Since a gynecologic oncologist performed some of the benign hysterectomy cases due to surgical complexity or suspicion of the rare leiomyosarcoma, surgical staging was planned and therefore a midline vertical incision were performed in these women. Of note, the majority of all women had a midline vertical incision (75.9%) compared to Pfannenstiel incision (24.1%). Interestingly, approximately two thirds of the studied cases were benign.
Lastly, our study did not include the preoperative or intraoperative opioid regimen, if any. Spinal and epidural anesthesia were part of the exclusion criteria of the study. By standardizing the intraoperative analgesic and sedation regimen, postoperative pain and opioid use could be interpreted to start at the same baseline.
Our future directions include conducting a prospective randomized controlled study where all included women will be scheduled to have the same type of incision or suspected pathology. A more diverse patient population will also be feasible by a multi-institutional study as opposed to our current single site study.
We acknowledge the limitations of a retrospective study in light of randomized controlled trials on this topic in the literature over the last few years. However, our study addresses the limitations of previous studies in that we include malignant pathology and excluded minimally invasive hysterectomy. By addressing these shortcomings, our study contributes to the current literature on the devastating impact of opioid abuse on our community.
TAP block is a feasible and effective analgesic option for acute postoperative pain after abdominal hysterectomy. In our overall studied patient population, opioid consumption was less in women who received a TAP block compared to women who did not. Multimodal regimens that include alternative, opioid-sparing analgesia are crucial for optimal patient recovery. ERAS protocols have become more formalized of which TAP blocks are an important component. Further research is warranted for the utilization of TAP block with different anesthetics in gynecologic surgery.
We would like to acknowledge Jim Yu, DO, Dipal Patel, Shiquan He, MS, Robert Samuelson, MD for their contributions.
All authors have contributed equally to the work.
None of authors have any financial or personal disclosures.