Mullerian or paramesonephric ducts form the female genital tract and any deviation from the normal can lead to Mullerian anomalies. Depending on the type of Mullerian anomaly; the presentations, required investigations and treatment options vary considerably and so does the counseling regarding the condition. Due to the highly varied profile of patients with Mullerian anomalies, a number of classification systems have been proposed to aid in their diagnosis and management. A thorough knowledge of the development of female genital tract and its associated anomalies is necessary to diagnose these disorders and an adequate workup is imperative before planning the treatment. This case series comprises of 17 cases of Mullerian anomalies, diagnosed through clinical history, physical examination, radiological scans or surgery. The case series is multiparametric in design and focuses on multiple parameters of an individual case. Through the present case series we aim to evaluate the various clinical presentations of the Mullerian duct anomalies, classify them as per ESHRE classification system, assess the other congenital anomalies associated with them and also study the optimum mode of management used for the respective cases.
Mullerian or paramesonephric ducts form the female genital tract and any deviation from the normal can lead to Mullerian anomalies. These anomalies represent a rather common benign condition with prevalence being 6.7% in the general population, 7.3% in the infertile population and 16.7% in recurrent miscarriage population [1]. The prevalence of various Mullerian anomalies is reported to be as follows [2]: Arcuate- 20%; Septate- 35%; Bicornuate Uterus- 25%; Unicornuate- 10%; Didephic- 8% and others- 3%. Depending on the type of Mullerian anomaly; the presentations, required investigations and treatment options vary considerably and so does the counseling regarding the condition. Due to the highly varied profile of patients with Mullerian anomalies, a number of classification systems have been proposed to aid in their diagnosis and management. The European society of human reproduction and embryology (ESHRE) and the European society for gynaecological endoscopy (ESGE) have developed a system of classification in 2013 - Congenital uterine anomalies (CONUTA) for a more effective way of classifying and managing mullerian anomalies [3].
A thorough knowledge of the development of female genital tract and its associated anomalies is necessary to diagnose these disorders and an adequate workup is imperative before planning the treatment. This case series comprises of 17 cases of Mullerian anomalies, diagnosed through clinical history, physical examination, radiological scans or surgery. The case series is multiparametric in design and focuses on multiple parameters of an individual case. Parameters like age, clinical presentation, hormonal profile, Ultrasonography (USG), Magnetic resonance imaging (MRI), Computed tomography (CT) scan, IVP (Intravenous pyelogram) findings & mode of treatment were analyzed. Through the present case series we aim to evaluate the various clinical presentations of the Mullerian duct anomalies, classify them as per ESHRE classification system, assess the other congenital anomalies associated with them and also study the optimum mode of management used for the respective cases.
A 15-year-old girl presented as a case of primary amenorrhoea. On examination her secondary sexual characteristics were found to be well developed. Uterus was 14 weeks size, mobile firm and non tender. Local examination revealed a thick transverse septum while on per rectal examination uterus, along with a mass in right fornix, could be palpated. USG and MRI findings confirmed hematocolpos, hematometra and transverse vaginal septum. She was taken up for laparotomy with vaginoplasty. Per operatively a high up transverse septum was resected followed by drainage of the collected fluid. On opening the abdomen hemi uterus with right cornua not communicating with cavity was discovered. An incision was given over right cornua to drain the fluid followed by cornual resection. Serial dilatation by Hegar's dilators followed by vaginal moulds insertion was done.
A 17-year-old girl who presented with primary amenorrhoea, had well developed secondary sexual characteristics on examination. Abdomen was soft, with no palpable mass and local examination revealed a blind vagina. No masses suggestive of uterus could be palpated on per rectal examination. Her hormone status was unremarkable. However on USG, right sided ectopic malrotated kidney with absent uterus and tubes-mullerain agenesis were found. IVP (Figure 1) and contrast enhanced CT abdomen confirmed a solitary ectopic pelvic kidney, non-visualized uterus consistent with Meyer rokitansky kuster hauser (MRKH) syndrome. Patient was counselled for vaginoplasty.
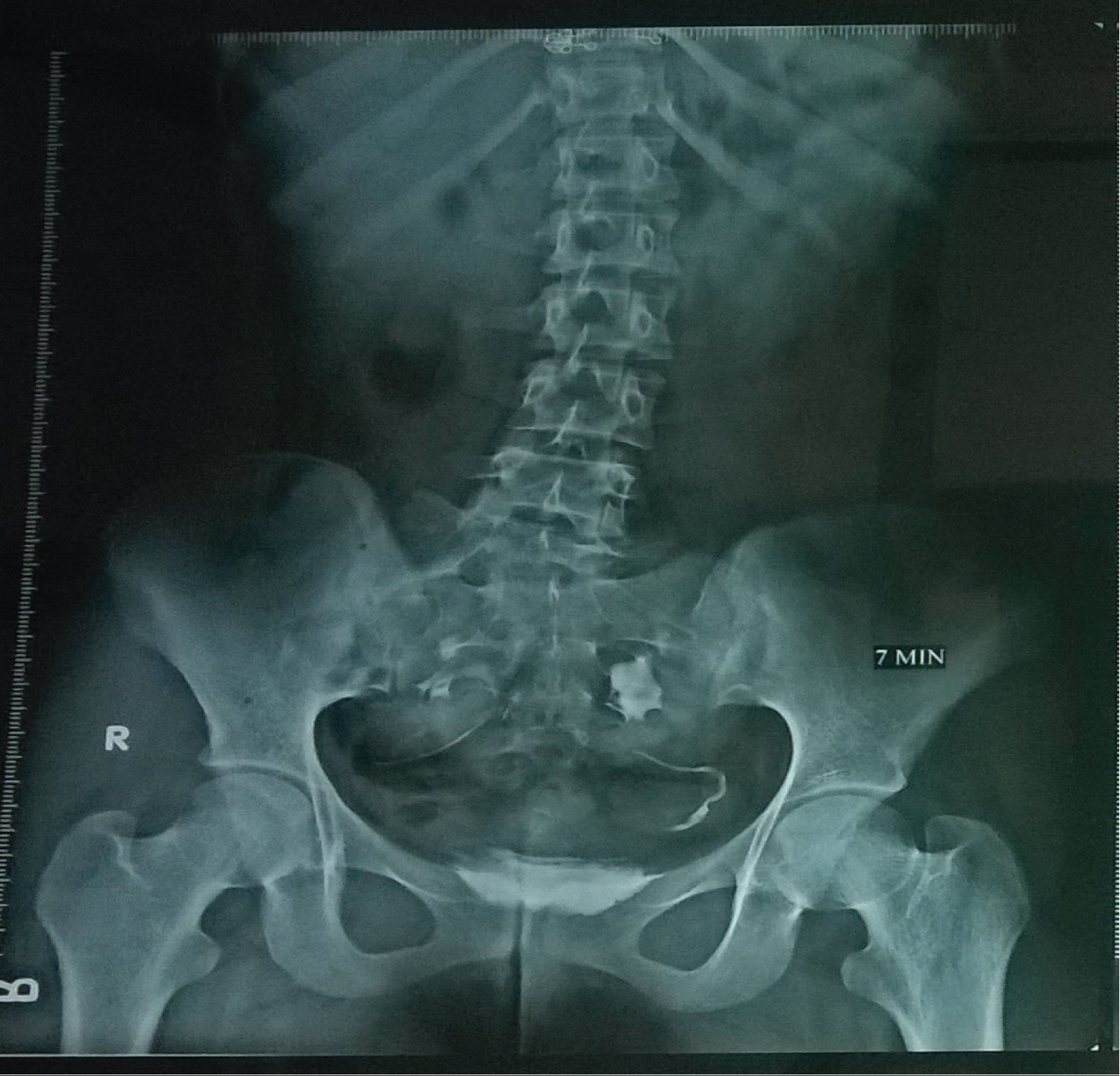 Figure 1: IVP showing solitary ectopic pelvic kidney. View Figure 1
Figure 1: IVP showing solitary ectopic pelvic kidney. View Figure 1
A 28-year-old nulliparous female, married for 7 years came with complaints of lower abdominal pain for 7-10 days. She also gave history of dysmenorrhoea, and oligomenorrhoea since 6 years. Eight years back patient had complaints of primary amenorrhoea for which she had undergone vaginoplasty with skin graft. She had undergone repeated cervical dilatations, following which she started having menses. Per abdominally a mass of 12-14 weeks was palpable in the suprapubic region with restricted mobility, vague tenderness and variegated consistency. On per speculum examination skin grafted vagina, with fibrosed tough vault was visualized. USG showed that the uterus was 8.2 × 4.5 × 5.5 cm with 14 mm thick endometrium. Both ovaries were not visualized separately. Fluid collection of 180 cc in left side of uterus and in right iliac fossa measuring 90 mm × 90 mm × 92 mm visualized with gut loops adherent within the fluid. There was also evidence of fluid in the pouch of Douglas. Patient underwent laparotomy. Per operatively uterus was found to be of 12 weeks size, left hydrosalphinx and adherent ovarian cyst. Right ovary was adherent to uterus & bowel with chocolate cyst. There was evidence of extensive endometriosis. Subtotal hysterectomy with bilateral salpingoopherectomy was done. Histopathology report confirmed myohyperplasia with predominant fibrous elements, Cystic glandular hyperplasia and bilateral ovarian endometriosis. Postoperatively patient was given Leuprolide acetate 3.75 mg subcutaneously every month for three doses followed by hormone replacement therapy (Figure 2).
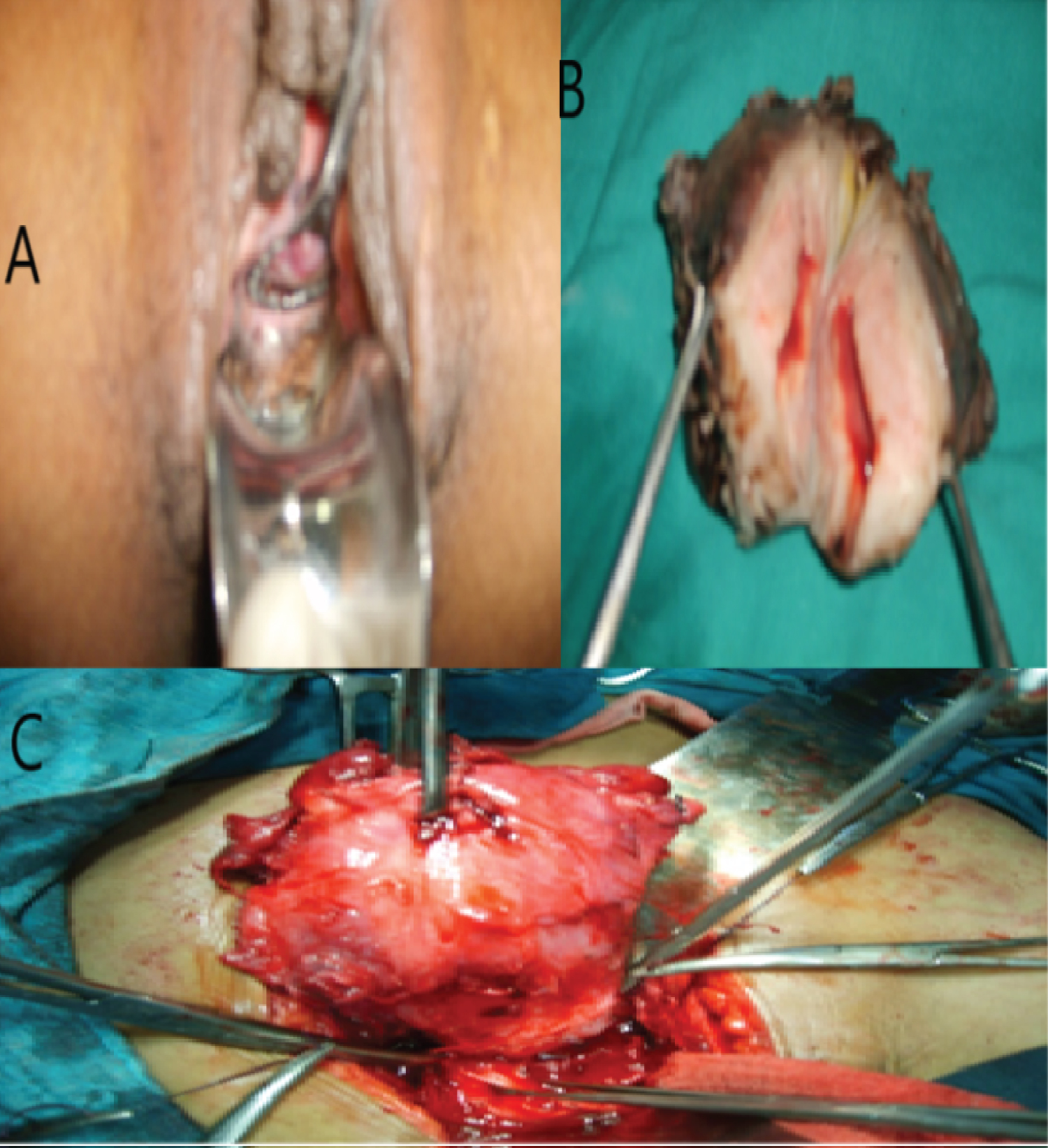 Figure 2: A) Per speculum examination showing skin grafted vagina; B) Uterus showing myohyperplasia; C) Peroperative; Uterus with multiple adhesions. View Figure 2
Figure 2: A) Per speculum examination showing skin grafted vagina; B) Uterus showing myohyperplasia; C) Peroperative; Uterus with multiple adhesions. View Figure 2
A 35-year-old nulliparous female presented with complaints of lower abdominal pain and dysparuenia of 3-4 months duration. She had not attained menarche and her marital stay was 2 years. On examination a mobile and firm mass of 14-16 weeks was palpable in suprapubic region. She has a 2 inches long blind vagina. Per vaginally a mass of 16 weeks size arising from the vagina could be palpated and per rectal findings were also consistent with it. USG showed a bulky uterus with a collection of 180 cc in vagina. IVP done was within normal limits. A diagnosis of high transverse vaginal septum with haematometra and haematocolpos was made. Per operatively a cruciate incision was given on septum with drainage of about 150 ml of collection. Cervical Os was not seen; instead a small dimple was visualized. A probe was inserted, followed by Hegar's dilator and around 20 ml collection from the uterus was aspirated. Mallecot's catheter was inserted and fixed in the tract thus created. Vaginal mould was inserted and patient instructed to use it regularly (Figure 3).
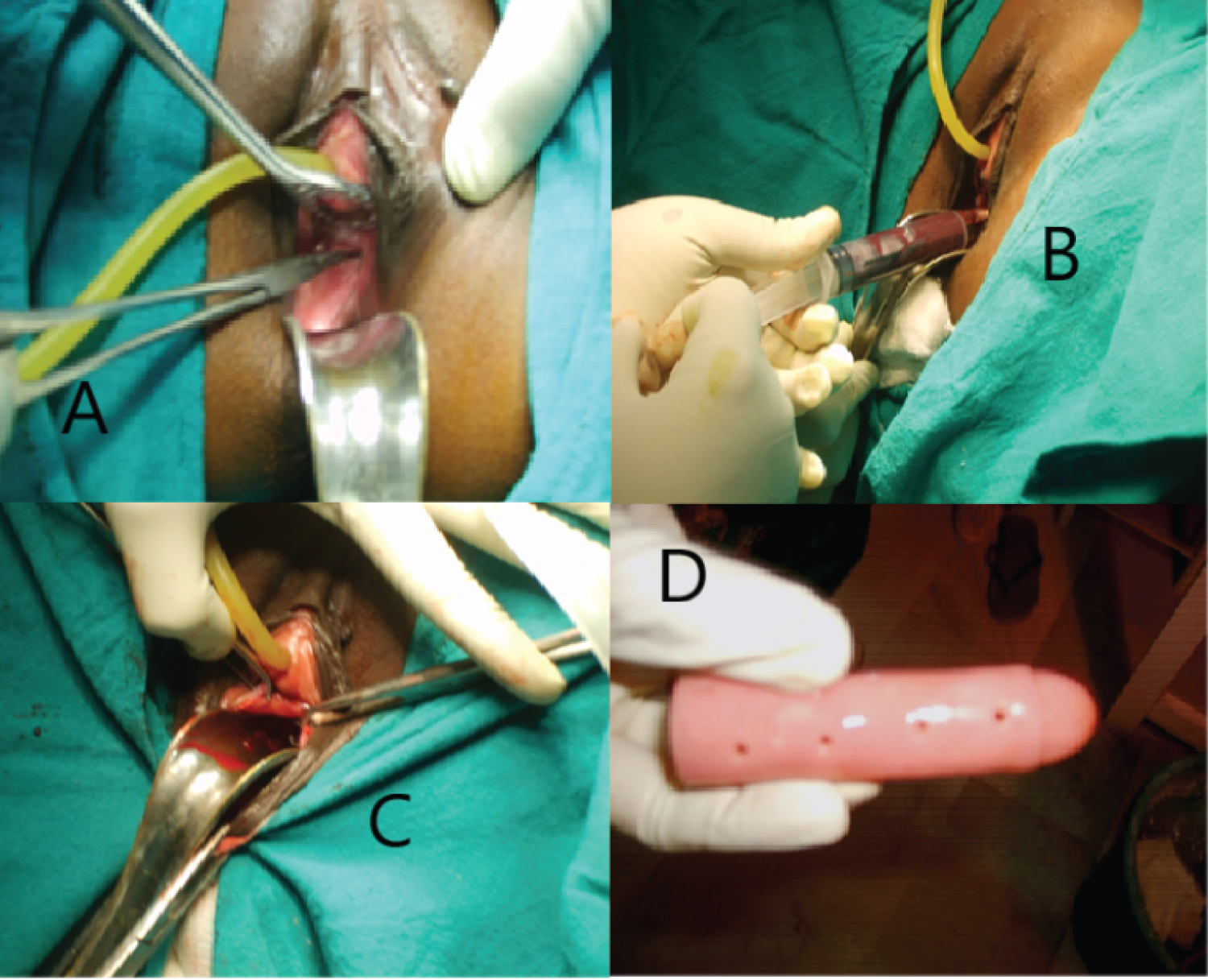 Figure 3: A) Per speculum examination showing blind vagina; B) Chocolate like material being aspirated from the hematocolpos; C) Excision of vaginal septum; D) Vaginal mould. View Figure 3
Figure 3: A) Per speculum examination showing blind vagina; B) Chocolate like material being aspirated from the hematocolpos; C) Excision of vaginal septum; D) Vaginal mould. View Figure 3
A 21-year-old nulliparous female, a case of primary amenorrhoea was found to have well developed secondary sexual characteristics. Her per abdominal examination was unremarkable, however she was found to have a blind vagina with a vaginal length of 3 cm on further examination Per rectally uterus and cervix could not be felt. A transverse band could be palpated. USG revealed a rudimentary uterus (24.6 × 10.3 × 16.7 mm) and normal bilateral adnexa. Diagnostic laparoscopy was done and per operatively bilateral ovaries and tubes were found to be present but the uterus could not be visualized.
A 17-year-old female presented with complaints of heavy menstrual bleeding since menarche. Per abdominal examination was unremarkable and per speculum/per vaginal examination was not done. On per rectal examination 2 separate masses were felt. However on USG patient was found to have uterus didelphys. She was treated symptomatically and counseled regarding evaluation to rule out other associated anomalies, but the patient did not come for follow up.
A 24-year-old female presented as a case of primary infertility. Examination findings and all investigations done for the evaluation of infertility were within normal limits. On USG she was discovered to have a uterine septum. She was taken up for hysteroscopy, where she was found to have a partial septate uterus and subsequently septoplasty was done. The patient is being followed up.
A 15-year-old girl presented with primary amenorrhoea. She had well developed secondary sexual characteristics on examination. Abdomen was soft, with no palpable mass and local examination revealed a blind vagina. No masses suggestive of uterus could be palpated on per rectal examination. Her hormone status was unremarkable. USG revealed absent uterus and tubes-mullerain agenesis. MRI confirmed MRKH syndrome with no other associated anomalies. Patient counselled for vaginoplasty.
A 56-year-old post menopausal female came with complaints of 2 episodes of bleeding per vaginum. No other significant past history or examination findings were found. Her evaluation for cancer cervix and cancer endometrium was unremarkable. When she did not respond to medical management, she was planned for hysterectomy. Per operatively left unicornuate uterus with absent right horn was found.
A 22-year-old female presented as a case of primary infertility. Examination findings and all investigations done for the evaluation of infertility were within normal limits. On USG she was discovered to have a uterine septum. She was taken up for hysteroscopy, where she was found to have a complete septate uterus and subsequently septoplasty was done. The patient was lost to follow up.
A 13-year-old girl presented with acute pain abdomen. She had attained menarche 1 year back and had her last menstrual period 6 weeks back. On examination a suprapubic lump of 22 weeks size was felt. It was bilobed, firm in consistency, non-tender and more on the right side. The same mass was felt vaginally, it was cystic, smooth, non-tender, and in direct communication with a bulge seen on the right side of the vagina. USG showed hematocolpos with hematometra. She was taken up for examination under anaesthesia. Old vaginal blood was aspirated followed by formation of a long window by excising a portion of the thick septum on the right side. Right sided cervical os was visible through the window. A final diagnosis of obstructed uterus bicornis bicollis with septate vagina was made.
24-year-old G2 P0 + 1L0 with 35 weeks 4 day pregnancy, presented at term with complaints of decreased fetal movement since 1 day. On examination fundal height was around 34 weeks, longitudinal lie, breech presentation, mild uterine contractions and fetal heart rate of 130 beats per minute. USG showed a Single live intra-uterine fetus (SLIUF) of 33 Weeks 2 Days gestation with breech presentation, severe oligohydramnios with posterior, upper uterine segment, grade II placenta and no obvious congenital anomaly. Patient underwent Lower segment caesarean section (LSCS). Per operatively the fetus was found to be in one horn and placenta in other with subseptate uterus and single cervix (Figure 4).
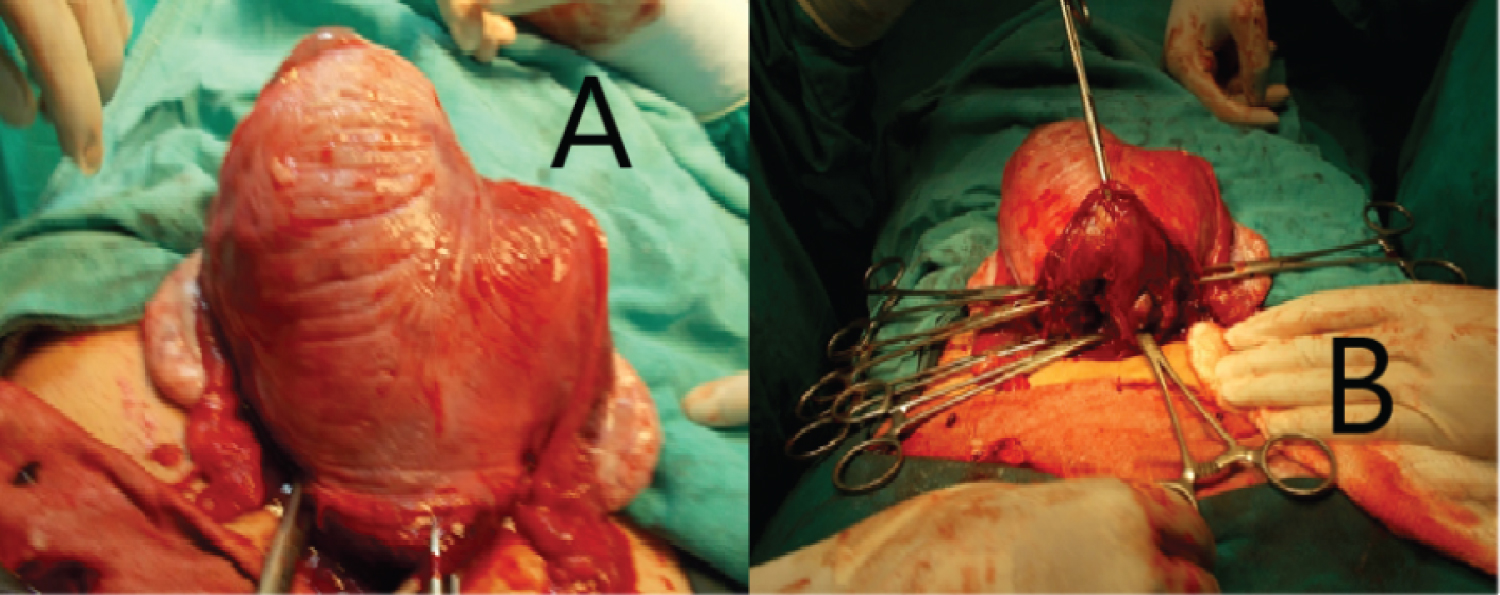 Figure 4: A) Sub-septate uterus; B) Septa. View Figure 4
Figure 4: A) Sub-septate uterus; B) Septa. View Figure 4
A primigravida with 16 weeks pregnancy came with complaints of acute pain abdomen. Her blood investigations were within normal limits however the USG showed ruptured ectopic pregnancy with fetus lying in the abdomen. She underwent laparotomy and per operatively a macerated fetus was found in the abdominal cavity, with a bicornuate uterus and ruptured cornua of left horn. Placenta was adhered to the cornua. Subsequently cornual resection was done following removal of the fetus.
A 25-year-old primigravida at 27 weeks 4 days of gestation came with uncontrollable bleeding per vaginum with central placenta previa (grade iv) with oligohydramnios. On examination her fundal height was 28 weeks with cephalic presentation and a fetal heart rate of 126 beats per minute. USG finding showed SLIUF of 22 weeks pregnancy with placenta completely covering the os with reduced liquor, and no congenital anomaly in the fetus. She underwent emergency surgery and per operatively a unicornuate uterus was present. Placenta seen anterior, adhered to upper and lower uterine segment and was delivered in bits. Baby delivered through placenta.
A 26-year-old female, G2 P1 L0 with 7 months period of gestation presented with complaints of leaking per vaginum since 18 hours. She gave history of previous preterm vaginal delivery at 30 weeks of gestation, 7 months back. Baby expired immediately after birth. On examination she had a fundal height of 24 weeks with oblique lie and breech presentation. Fetal heart rate was 150 beats per minute. USG showed a SLIUF with nil liquor. Patient was taken up for caesarean section in view of anhydraminos. Per operatively right sided unicornuate uterus with absent left horn with normal tubes & ovary was seen.
A 26-year-old G1 P0 L0 with 37 weeks 6 days pregnancy, presented at term with complaints of pain abdomen since 1 day. On examination fundal height was full term, oblique lie, with moderate uterine contractions and fetal heart rate of 138 beats per minute. USG showed SLIUF of 37 weeks 2 days gestation with oblique lie and no obvious congenital anomaly. Patient underwent Lower segment caesarean section (LSCS). Per operatively a unicornuate uterus with no horn was found with bilateral normal ovaries.
A 28-yrs-old female G2 P1 L0 with 8 months period of gestation presented with complaints of pain abdomen since 12 hours. She gave history of previous preterm vaginal delivery at 8 months of gestation, 2 years back. On examination she had a fundal height of 34 weeks with transverse lie and mild uterine contractions were present. Fetal heart rate was 140 beats per minute. Patient was taken up for caesarean section in view of transverse lie in labour. Per operatively right sided unicornuate uterus with left rudimentary horn with no cavity with normal ovaries was seen.
Table 1 summarizes the clinical picture, associated Mullerian anomaly and subsequent management of the respective cases.
Table 1: The clinical picture, associated Mullerian anomaly and subsequent management of the respective cases. View Table 1
The series comprises of 17 cases of Mullerian anomalies, diagnosed through clinical history, physical examination, radiological scans or surgery. Out of the 17 cases, 11 cases presented with gynaecological problems and remaining 6 were patients with obstetrical complaints.
The most common age presentation in obstetric cases was 24-26 years and 14-17 years in gynaecology cases. In literature the average age at diagnosis of Mullerian anomalies is reported to be from 10-18 years [4].
Primary amenorrhoea was the most common complaint among the gynaecological cases while others presented with primary infertility. Similar to the findings by Vyas, et al. who reported primary amenorrhea as the most common symptom in a study conducted in India in 2018 [5].
Amongst obstetrical cases, main problem encountered were ectopic pregnancy, recurrent pregnancy loss, abortion and preterm labour. Poor obstetric outcomes are mainly attributed to those anomalies which involve the uterus and include increased rate of recurrent pregnancy loss, pre-term delivery, malpresentations, fetal growth restriction and increased caesarean delivery rates [6].
In the present study the most common anomaly encountered in obstetric cases was unicornuate uterus, contrary to the findings by Raj, et al. who did an observational study of effect of Mullerian anomalies on pregnancy in 2019, and found that the most common anomaly complicating pregnancy was septate uterus (36.6%) [7].
Amongst the gynaecological cases the most frequent diagnosis made was MRKH. Agarwal, et al. evaluated cases of Mullerian anomaly over a period of three years and discovered MRKH syndrome was the most common diagnosis for the cases which presented with primary amenorrhoea [8].
In the current study almost all patients were worked up for other anomalies, however only one patient was found to have associated renal anomaly. According to the work done by Li S, et al. [9], the association between renal and Mullerian agenesis is around 30%. Treatment modalities in both obstetric and gynaecological cases were mostly individualized according to the case diagnosed.
A clear knowledge about the types, diagnosis, surgical management if any and the consequences of the Mulllerian anomalies and its management is important.
Mullerian anomalies of obstructive nature are atypical and frequent in adolescence therefore strong clinical suspicion is imperative for making a proper diagnosis. Investigating modalities commonly used for diagnosis are USG, HSG, MRI, CT scan and IVP. HSG is the most common investigation whereas MRI continues to be the benchmark for accurate diagnosis of Mullerian anomalies. A thorough investigation of urinary tract should also be done, as solitary ectopic kidney could be mistakenly injured or excised during surgery. Frequently encountered upper urinary tract abnormalities include renal anomalies (20-30%) such as a horseshoe or pelvic kidney or renal agenesis, duplication of the collecting system, and ectopic ureters. The priority in such cases should be fixation of obstructive symptoms and achievement of normal menstrual, sexual and reproductive functions. Psychological treatment and reconstructive surgery are the main stay of management. The female should also be made aware of the possibility of treatment failure and the counseling should focus on the severity of the malformation in question. On the contrary the anomalies which are diagnosed first time during pregnancy are usually found to be minor and management revolves around a favorable pregnancy outcome along with fixation of the anomaly where possible.
None.
None.