Condyloma acuminata or genital warts are the clinical expression of infection from certain types of human papillomavirus (HPV) that are considered to have low oncogenic risk (No. 6 and No.11). They are currently considered one of the most common sexually transmitted diseases with increasing incidence among most populations [1].
The lesions present and extend in numerous forms (from very localized forms and limited disease to very extensive forms with multi-focal involvement of the anogenital tract). Sometimes, the lack of a single effective treatment for all patients means that we have to choose from the different available procedures (excisional, destructive, topical, etc.). Let's not forget the high post-treatment relapse rate, as new lesions appear in treated or untreated areas [2].
Genital infection by HPV is one of the most common sexually transmitted infections. However, condyloma acuminata are not included in surveillance systems in most countries, so worldwide epidemiological data is limited. According to systematic reviews, the incidence of new cases (among men and women) ranges between 118 and 205 per 100,000 inhabitants. The highest incidence rate is observed from 20 to 24-years-old for women, and 25 to 29-years-old for men [2,3].
A 26-year-old patient visiting our office in CIMEG MADRID (Vithas La Milagrosa) in August 2020 due to presenting multiple vulvar condyloma lesions that had already been evaluated and treated in a dermatology center using local cryotherapy and sinecatechins (Veregen) ointment twice a day at home. The patient mentions experiencing intense stinging when applying the ointment, as well as continuous symptoms of local itching and discomfort, so in the absence of visual improvement, she decided to seek out another medical opinion.
Ethnicity: Latin American.
Personal disease history: No chronic diseases of interest
Smoker: Yes (3-5 cigarettes a day)
First sexual relations: 16-years-old
No. of sexual partners stated: 4
Long-term sexual partner: Not presently (but she had one until the lesions appeared)
Pregnancies: No
Contraceptive method: No
Family disease history: None of interest
Cytology provided with benign cell changes, dated June 2020
HPV vaccination: No
In the standard lithotomy position (for gynecology), a thorough vulvar examination was performed (vulvoscopy) using a colposcope and staining with acetic acid at 2% across the entire vulvar area in order to detect other smaller-sized lesions in the affected area. We observed protruding condylomas on an extensive plaque base, some of which were reddish and others with more pigmentation, almost brown (due to the evolution time and aforementioned treatment). Other smaller lesions approximately 1 mm in size were detected on the clitoris hood, the external zone of the lower lips, and the vaginal vestibule.
A vaginoscopy and colposcopy were also performed, ruling out the presence of condylomas (inside the vaginal channel and the cervix). Perianal condylomas on the patient are ruled out, despite mentioning a lack of anal coitus and symptoms of anal itching or rectorrhagia.
The physical examination is the "gold standard" when diagnosing this disease. Biopsies on the lesions is not standard procedure; they are only performed if the treatment response is not as expected, the lesions are suspicious, or the patient is a girl (due to suspected sexual aggression) [4].
There are dissimilar differential diagnoses for these lesions that we could mention. I found this clinical case very clear, as can be seen in the attached photos. However, I propose some pathologies or lesions that could cause confusion and should be differentiated.
Vestibular papillomatosis: Finger-like proliferations of mucosa centered around a connective-vascular axis. They are located on the internal face of the lower lips, sometimes extending throughout the vestibule. Not HPV-related. It is a benign condition with no pathological correlation.
Fordyce spots: These are heterotopic sebaceous glands. They present in the form of white-yellowish pimple-like structures 1-3 mm in diameter, either isolated or grouped into plaques, mainly on lower lips and the internal face of upper lips.
Molluscum contagiosum: A viral lesion (poxvirus), specifically Molluscum contagiosum virus. It presents as pink or skin-colored pimple-like structures, with a smooth surface and with a characteristic central thread.
Malignant tumors: They should be suspected if there are any exophytic, hard, ulcerative lesions with fleshy borders and a bleeding surface.
Prior to starting a treatment plan, a suitable explanation needs to be provided to ensure that the patient understands: The evolution of the process, the purpose of the treatment, the potential adverse effects that may appear, and the healing and relapse percentages.
For this patient, we started the first session by using a laser on the vulvar region (with condylomas), type Er: YAG with a wavelength of 2940 nm. This laser enables us to perform accurate ablation without heating the surrounding tissue. Water - the chromophore representing the main objective with skin treatments - absorbs Er: YAG energy very well, thus allowing skin vaporization with micrometer-guided precision and very little heat conduction [5].
We then prescribed a home co-adjuvant treatment for the region treated for condylomas to be administered for 42 nights (apart from during the period). The Papilocare vulvar gel helps to re-epithelialize and hydrate that zone due to its composition:
-Hyaluronic acid niosome, providing hydration and elasticity.
-Antioxidant β-glucan niosome to maintain a suitable skin and mucosa structure.
-Healing and repairing Centella Asiatica phytosomes.
-Bioecolia: Balances the genital region flora.
-Aloe vera: Hydrates and re-epithelializes.
-Coriolus Versicolor: Re-epithelializes genital lesions.
Neem extract: Moisturizer, relieving itching and redness.
This gel does not contain parabens or scents and has a pH of 5 [6,11].
At the end of the 6th week (42 days), a second local vulvar laser session is performed, and vulvar gel co-adjuvant treatment is indicated again (21 nights each month) for a total of 6 months.
She is re-evaluated clinically after the 2nd session and 42 days of treatment, with fewer lesions observed and the patient asymptomatic.
We explain to the patient that the final evaluation would take place at the 6th month since the treatment protocol started. She visits in March 2021 (6th month check-up) for evaluation:
Another vulvoscopy with acetic acid to 2% was performed, as no lesions are observed macroscopically. Vulvoscopy with no lesions. We observed a complete lack of lesions and scars as shown in the photo. The patient is currently asymptomatic, not on treatment, with healed lesions.
She is encouraged and recommended to do the following as part of her treatment (Figure 1):
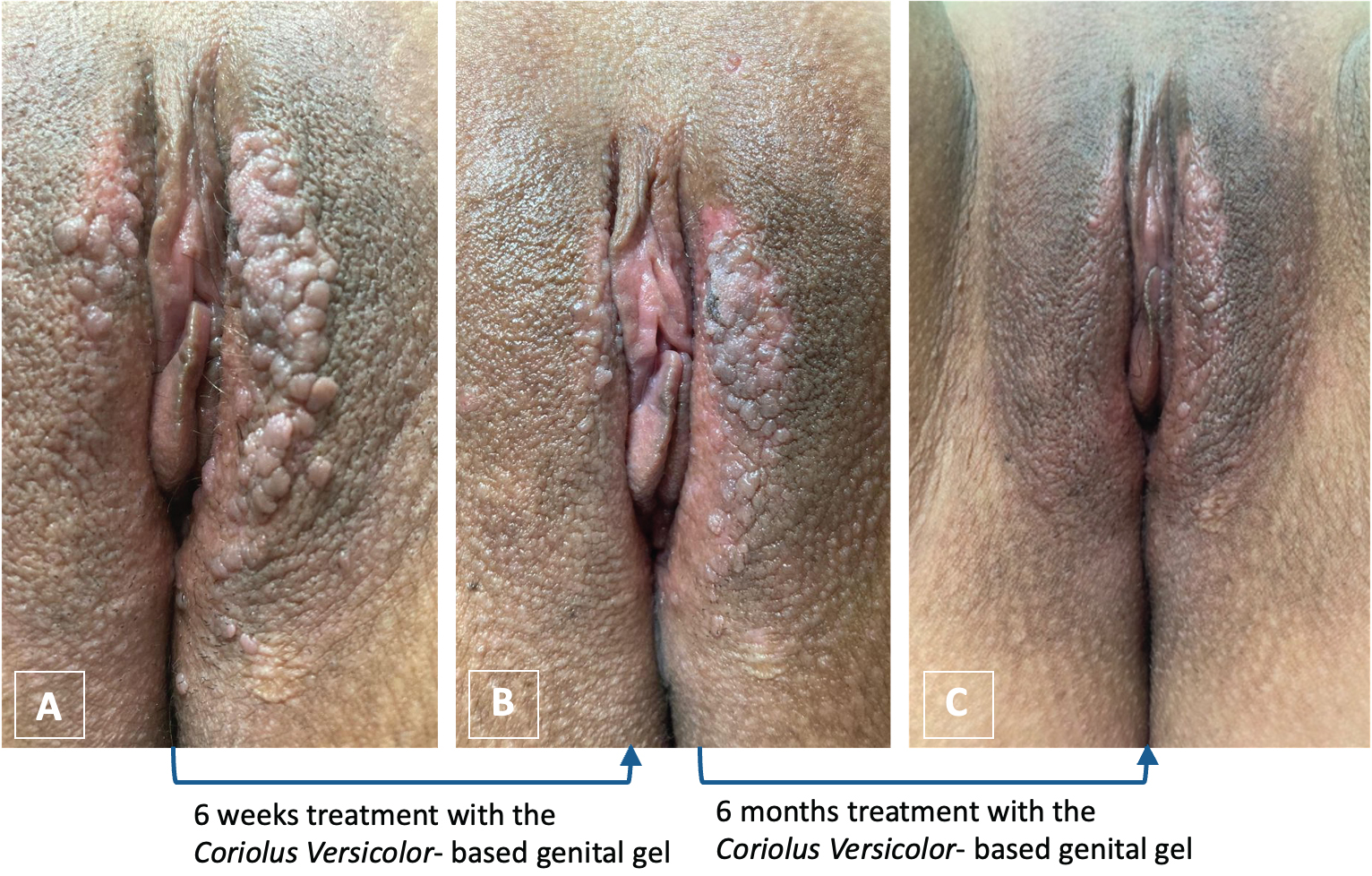 Figure 1: Volvuscopy observations, (A) after the first laser session, (B) after the second laser session and 6 weeks treatment with the Coriolus
Figure 1: Volvuscopy observations, (A) after the first laser session, (B) after the second laser session and 6 weeks treatment with the Coriolus
Versicolor- based genital gel, and (C) the result after 6 months of treatment with the Coriolus
Versicolor- based genital gel after the 2nd laser session.
View Figure 1
-Give up smoking.
-Start HPV vaccination.
-Always use a barrier method.
-Visit for check-up at 12 months since starting the treatment.
HPV is the causal agent for condyloma acuminata. Genotypes 6 and 11 are responsible for 95% of condyloma acuminata. Other genotypes involved less often are: 8, 13, 30, 32, 42, 43, 44, 54, 55 and 70. Up to 20-30% of cases present co-infection by high-risk oncogenic types of HPV [4,12].
The incubation period ranges between 3 weeks and 8 months, and the average time for lesions to appear after infection is 2 months, making condyloma acuminata the first clinical marker of sub(acute) infection by HPV18 [4]. Sexual contact is the main route of transmission. The main risk factors are the number of sexual partners and the early onset of sexual relationships. It is a very common disease among immuno-compromised patients.
If left untreated, condyloma acuminata can resolve unaided, remain unchanged, or increase in number and/or size. Physiological immunosuppression states, such as pregnancy, favor condyloma progression [6-8]. There is no scientific evidence to show one treatment is clearly superior to another. Treatment must always be personalized, as there isn't one that is more suitable for all patients and all types of condyloma acuminata.
Multiple variables need considering when choosing the most suitable treatment, such as: The number and size of lesions, the area of the lesions, whether or not keratosis is present, the doctor or therapist's personal experience, the potential for treatment adherence, toxicity, side effects, prices, etc [7-9].
For this clinical case, the combination or synergy of laser therapy with the locally administered vulvar Papilocare gel turned out to be suitable for this patient with a satisfactory evolution, the complete elimination of lesions, and no relapses 6 months after treatment. Vaccines containing viral genotypes 6 and 11 (tetravalent and nonavalent) are currently the most effective primary prevention method for condyloma acuminata, with efficaciousness highest when administered before the first sexual relationship [8-10]. The nature of the disease and the fact that it is linked to sexual transmission causes a major physical, emotional, and psychosexual impact among affected patients, so we should insist that the adolescent population is fully vaccinated.