A vaginal adhesion is an uncommon complication of vaginal surgery. While treatment options for radiation-induced vaginal stenosis and vaginal septum have been well-characterized, there is little to guide surgeons providing care to patients with intravaginal adhesions. This report presents a multigravida with history of anterior and posterior colporrhaphy and perineoplasty referred from an outpatient abortion clinic for a dense longitudinal adhesion obstructing the cervix. A multidisciplinary approach under general anesthesia with Complex Family Planning and Urogynecology allowed for dissection of the adhesion, vaginal patency, and safe abortion. This is the first case study outlining the multidisciplinary management of a dense, obstructing longitudinal adhesion to allow for safe abortion. This report may serve as a preliminary reference for surgeons encountering similar obstructive vaginal lesions.
The development of vaginal adhesion is an uncommon postoperative complication. In a small, single-institution study, 10.9% of patients developed vaginal adhesions after transvaginal pelvic reconstructions; however, this tissue was easily separated on pelvic examination at the first postoperative visit without lasting effect [1].
While treatment options for radiation-induced vaginal stenosis and vaginal septum have been well-characterized, there is little to guide surgeons providing care to patients with intravaginal adhesions. Literature outlining management for patients with obstructing longitudinal vaginal adhesions or septum, particularly in pregnancy, is limited to case reports, and recommendation has generally involved clamping and sharp resection of the adhesion or maneuvering around it [1-5].
This report presents a multigravida with history of anterior and posterior colporrhaphy and perineoplasty referred from an outpatient abortion clinic for a dense longitudinal adhesion obstructing the cervix. This case demonstrates a successful multidisciplinary approach to the abortion procedure.
Written consent was obtained from the patient prior to publication. As a case report, this manuscript was exempt from IRB approval.
A 29-year-old G6P3023 presented to a hospital-affiliated outpatient family planning center at 10 weeks 1 day gestational age for pregnancy termination. She was referred from an outpatient abortion clinic for patient-described "scar tissue on her cervix". She reported having a "vaginal rejuvenation surgery" for stress urinary incontinence two years prior with subsequent recurrent dyspareunia. On review of her records and previous operative report, she was found to have history of uncomplicated anterior and posterior colporrhaphy and perineoplasty using Vicryl and Monocryl suture with estimated blood loss of 160 milliliters. Of note, no previous post-operative cervical exam was documented; a two-week postoperative vaginal examination only noted well-healing vaginal tissue. The patient's medical and surgical history was otherwise unremarkable. On examination, we noted a thick, longitudinal adhesion approximately 4 centimeters from the introitus measuring 3 centimeters transversely and completely obstructing the cervix (Figure 1). Pelvic ultrasound revealed an intrauterine pregnancy and an anterior uterine fibroid measuring 3 × 4 × 5 centimeters. In the setting of this prominent vaginal adhesion and undesired pregnancy, we coordinated both Complex Family Planning and Urogynecology involvement.
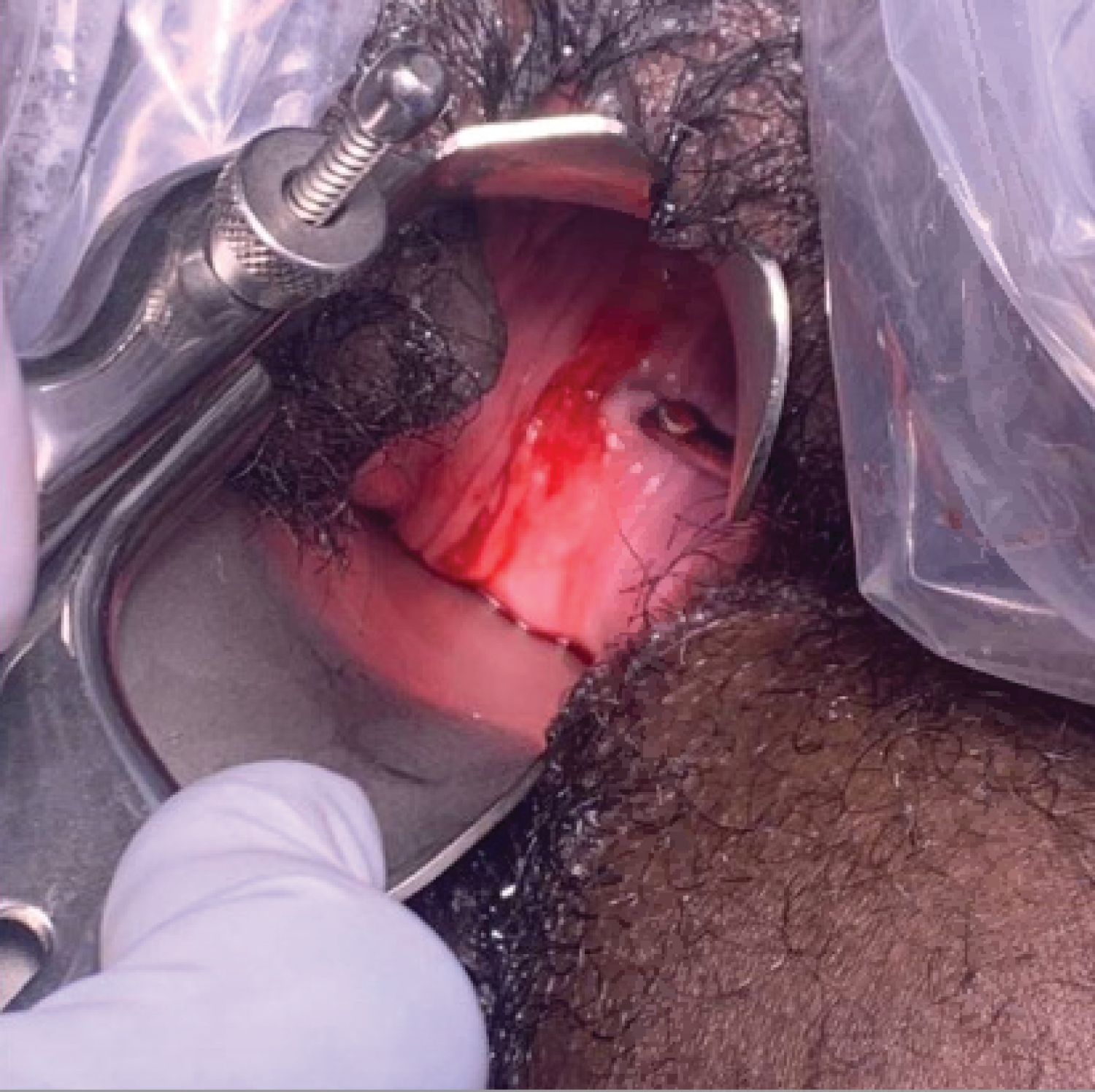 Figure 1: Dense vaginal adhesion obstructing view of distal vagina and cervix (small defect revealed by the placement of the uterine sound on the left side of the adhesion).
View Figure 1
Figure 1: Dense vaginal adhesion obstructing view of distal vagina and cervix (small defect revealed by the placement of the uterine sound on the left side of the adhesion).
View Figure 1
We performed the procedure at 13 weeks 0 days gestational age under general endotracheal anesthesia. The interval between patient presentation and procedure was due to coordination of operating room time and physician availability. Upon speculum insertion, we again noted the above findings. A defect was identified on the left side of the adhesion, which could be manually dilated to one centimeter. We were then able to palpate the patient's cervix behind the adhesion. Uterine sound was used in the defect to elevate the adhesion away from the posterior vaginal wall and cervix. We placed Allis clamps superiorly and inferiorly along the adhesion for stabilization and mobilization. We injected the adhesion with lidocaine and epinephrine for hemostasis. We used Metzenbaum scissors for resection. The adhesion was then sharply dissected until the superior and inferior aspects of the vagina were freed and the cervix could be fully visualized (Figure 2).
 Figure 2: Cervix visualized after vaginal adhesion removed (single-tooth tenaculum is at 9 o'clock on the cervix).
View Figure 2
Figure 2: Cervix visualized after vaginal adhesion removed (single-tooth tenaculum is at 9 o'clock on the cervix).
View Figure 2
We then completed the suction dilation and curettage under ultrasound guidance. The vaginal repair was completed using interrupted sutures of 2-0 Vicryl placed along the superior aspect of the adhesion and in a circumferential manner. Hemostasis was excellent and the vagina was patent at the end of the case.
The patient tolerated the procedure well and was discharged home. She was counseled to return for follow up in 2 weeks with plan for dilator and vaginal estrogen therapy. She was contacted by phone 1 week postoperatively, at which time she was recovering well. She was subsequently lost to follow up. Pathology of intrauterine contents confirmed products of conception; the adhesion was not sent for evaluation.
To our knowledge, this is the first documented case of an abortion performed in the setting of a dense, obstructing adhesion resultant from prior surgery.
Initially, we planned for possible vaginoscopy or hysteroscopy at time of termination, as previously outlined by Setchell, et al. for abortion in a patient with uterus bicornisbicollis [6]. The report described a patient with congenital uterine and vaginal anomalies with history of previous vaginal septum repair; the authors used flexible hysteroscopy to visualize and disrupt the pregnancy.
We also considered medication abortion, given there was most likely a defect in the adhesion that allowed for conception to occur. However, given the gestational age and concern for retained products behind the adhesion, as described in a case report by E. Gibson, this was not our first choice [7]. We also considered preoperative misoprostol for cervical ripening prior to this case as previously used by Pitotti, et al. in a case of transverse vaginal septum, but did not pursue this option in case we could not complete the procedure [4]. Ultimately, cervical dilation was successful without misoprostol.
Further exploration of the long-term success of adhesion takedown is warranted. The findings of this case report may serve as a preliminary reference for surgeons encountering similar obstructive vaginal lesions.
Written consent was obtained from the patient prior to publication. As a case report, this manuscript was exempt from IRB approval.
All authors contributed to this case and its manuscript.
All data used to support the conclusions of this study are included in the above article.
The authors have no relevant conflicts of interest.
There was no source of funding for this article.