A 25-year-old nulligravid was consulted due to inability to have sexual intercourse accompanied by chronic urinary hesitancy, dribbling, and dysmenorrhea. On gynecologic pelvic examination, she presented with complete, adult-onset fusion of the labia minora.
This paper describes a stepwise management of a reproductive-age woman with complete labial fusion. Treatment goals include etiological determination, anatomic correction, restoration of normal sexual function, improvement of genitourinary function, and improved quality of life. She underwent vaginoscopy with incision of labial agglutination and repair. Corrective surgery has led to full exposure of the normal vaginal introitus. Post-operatively, topical antibiotics, petrolatum gel, and estrogen cream were applied resulting in a normal anatomy after 2 months. Healthy sexual function was achieved and, six months later, she conceived.
Labial fusion during reproductive years should be carefully investigated as this is exceedingly rare and unexpected in reproductive-age women with normal hypothalamic pituitary ovarian (HPO) function. Issues of underlying predisposing factors need to be addressed and are necessary to prevent recurrence.
Labial adhesion, Labial agglutination, Labial fusion, Synechiae vulvae
Labial agglutination is a clinical condition seen in the hypo-estrogenic state such as in pre-pubertal and post-menopausal females. Thus, extremely rare in reproductive-age women [1]. This may result from numerous existing etiological and contributing factors in older adult women such as the presence of local inflammation, senile vaginitis, hypoestrogenism, lack of sexual activity, local trauma, sexual abuse, vaginal laceration following childbirth and recurrent UTI (UTI) [2,3]. In this regard, having a past medical history of recurrent urinary tract infection should not be dismissed.
Moreover, the inability to start a family due to sexual dysfunction with other gynecologic symptoms could raise the suspicion of unusual entities in the reproductive years.
A 25-year-old nulligravid consulted for inability to have sexual intercourse due to an absent vaginal introitus. She also reported long-standing urinary hesitancy, dribbling, and dysmenorrhea. Throughout her year-long marriage, she was unable to have intercourse. This, along with infertility, caused her significant distress.
Eight years prior to consultation, she experienced recurrent bouts of urinary tract infection - 5 episodes within a year. She was given Co-amoxiclav 625 mg/tab and Ciprofloxacin 500 mg/tablet on different occasions. Urinary symptoms resolved after antibiotic treatment. No further investigations were done. A year later, she experienced urinary hesitancy and dribbling. Shortly after, she developed mild dysmenorrhea. However, she was not overly bothered by these symptoms and did not seek medical care.
Until one year prior to consult, she developed new-onset hypomenorrhea with worsening of urinary symptoms, and dysmenorrhea which prompted consult.
Developmental history was unremarkable. Menstrual history was normal prior to the onset of hypomenorrhea. She denies any history of trauma, sexual abuse, vulvar infections, dermatitis, and poor hygiene.
On physical examination, both breast and pubic hair were fully developed. The labia minora were fused. A midline raphe was noted. A pinpoint hole was located 2 cms above the posterior fourchette where urine and menstrual blood egress (Figure 1).
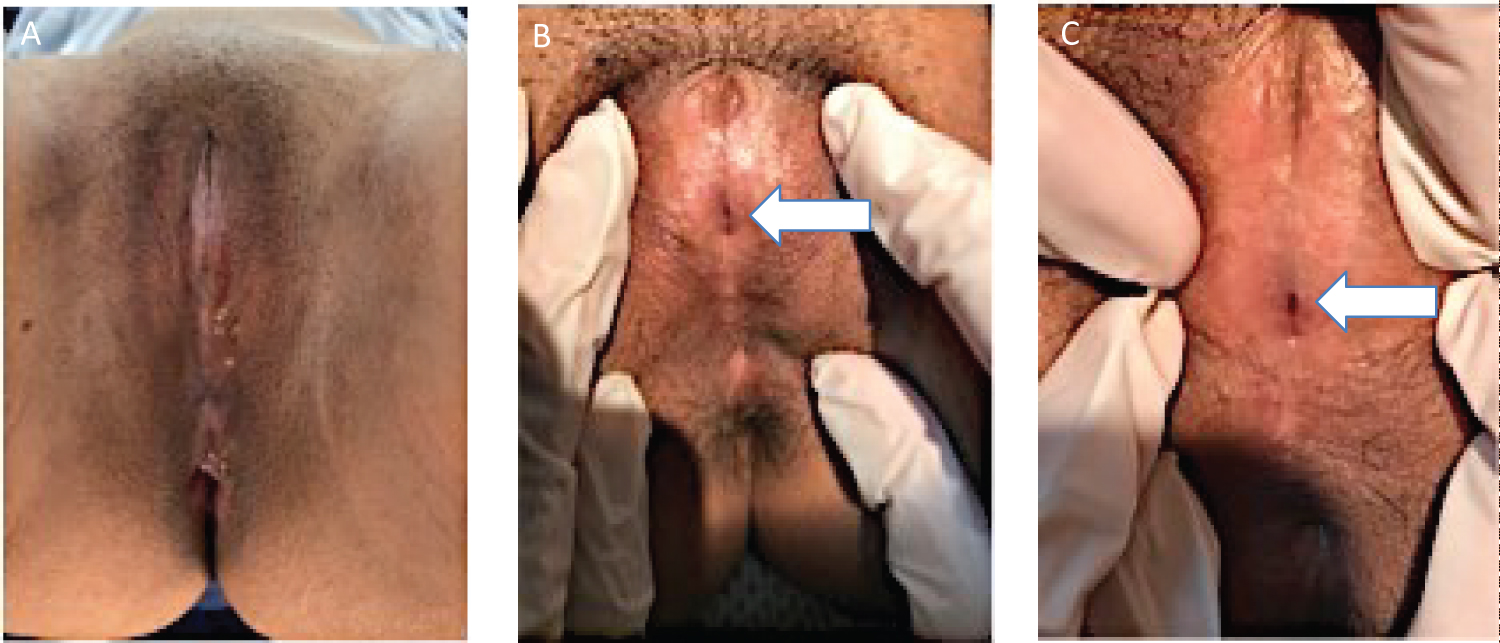 Figure 1: Pelvic examination of genitalia. A) Adhered labia completely obscuring the clitoral hood and vaginal opening; B,C) Fused labia minora with thin midline raphe as pointed by the arrow; C) A pinpoint hole located 2 cms above the posterior fourchette as pointed by the arrow.
View Figure 1
Figure 1: Pelvic examination of genitalia. A) Adhered labia completely obscuring the clitoral hood and vaginal opening; B,C) Fused labia minora with thin midline raphe as pointed by the arrow; C) A pinpoint hole located 2 cms above the posterior fourchette as pointed by the arrow.
View Figure 1
The hymen, urethra and clitoral hood were hidden. Bimanual examination was unremarkable.
Baseline hormonal profile, urinalysis, creatinine, sexually transmitted infection panel, non-ionic contrast KUB and transrectal ultrasound were unremarkable. ANA titers were elevated but confirmatory testing - anti-DsDNA, anti-Smith, and anti-Ribonucleoprotein - were all negative. A trans-perineal ultrasound scan showed labial agglutination, with soft tissue measuring 0.4-0.5 mm overlying the introitus, and a concomitant incomplete vaginal septum (Figure 2).
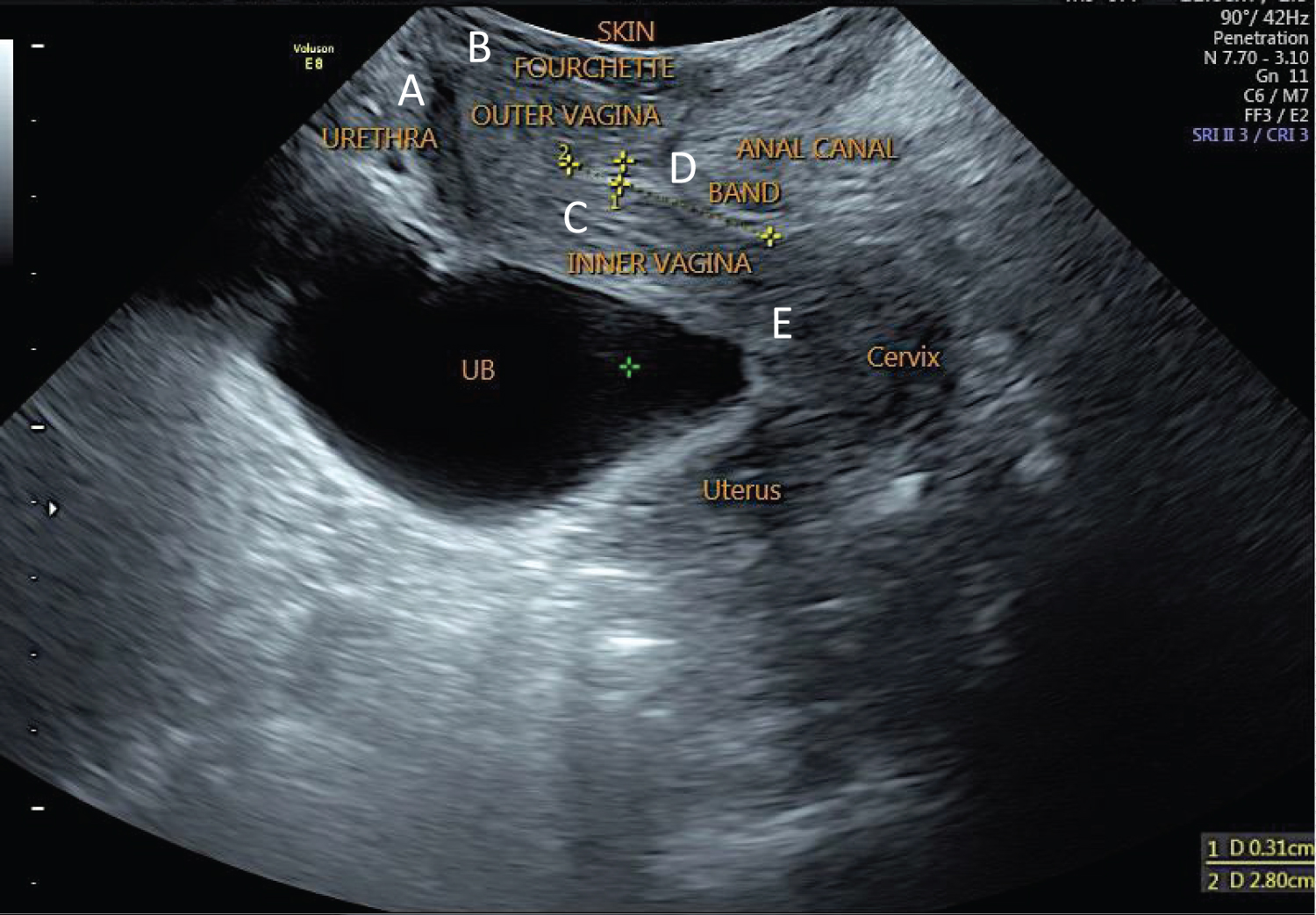 Figure 2: Transperineal scan. Symphysis pubis, urethra, vagina, cervix, uterus and anal canal were visualized clearly. A) Urethra measures 2.4 cm in length with a diameter of 0.6 cm; B) Distance between the upper tip of the urethra to the vaginal space anteriorly is 0.87 cm and urethra to the inner border of the vagina = 1.38 cm; C) Upper third of the fourchette to the inner border of the vagina = 1.52 cm; D) A transverse hyperechoic band seen on the left mid- cavity of the vaginal space extending to the inner vaginal canal, 2.8 × 0.31 cm, suspicious of incomplete vaginal septum and is 1.70 cm away from the fourchette; E) Distance from the inner vagina to the cervix = 2.87 × 1.37 cm.
View Figure 2
Figure 2: Transperineal scan. Symphysis pubis, urethra, vagina, cervix, uterus and anal canal were visualized clearly. A) Urethra measures 2.4 cm in length with a diameter of 0.6 cm; B) Distance between the upper tip of the urethra to the vaginal space anteriorly is 0.87 cm and urethra to the inner border of the vagina = 1.38 cm; C) Upper third of the fourchette to the inner border of the vagina = 1.52 cm; D) A transverse hyperechoic band seen on the left mid- cavity of the vaginal space extending to the inner vaginal canal, 2.8 × 0.31 cm, suspicious of incomplete vaginal septum and is 1.70 cm away from the fourchette; E) Distance from the inner vagina to the cervix = 2.87 × 1.37 cm.
View Figure 2
The team was cognizant of the apposition of the soft tissues and the risk for injuring the urethra and rectum; hence, an initial small incision was made followed by vaginoscopy technique - the vaginal wall was clearly visualized, normal looking with no septum appreciated, the cervix appeared smooth and grossly normal. Proceeded with incision of labial agglutination and repair (Figure 3).
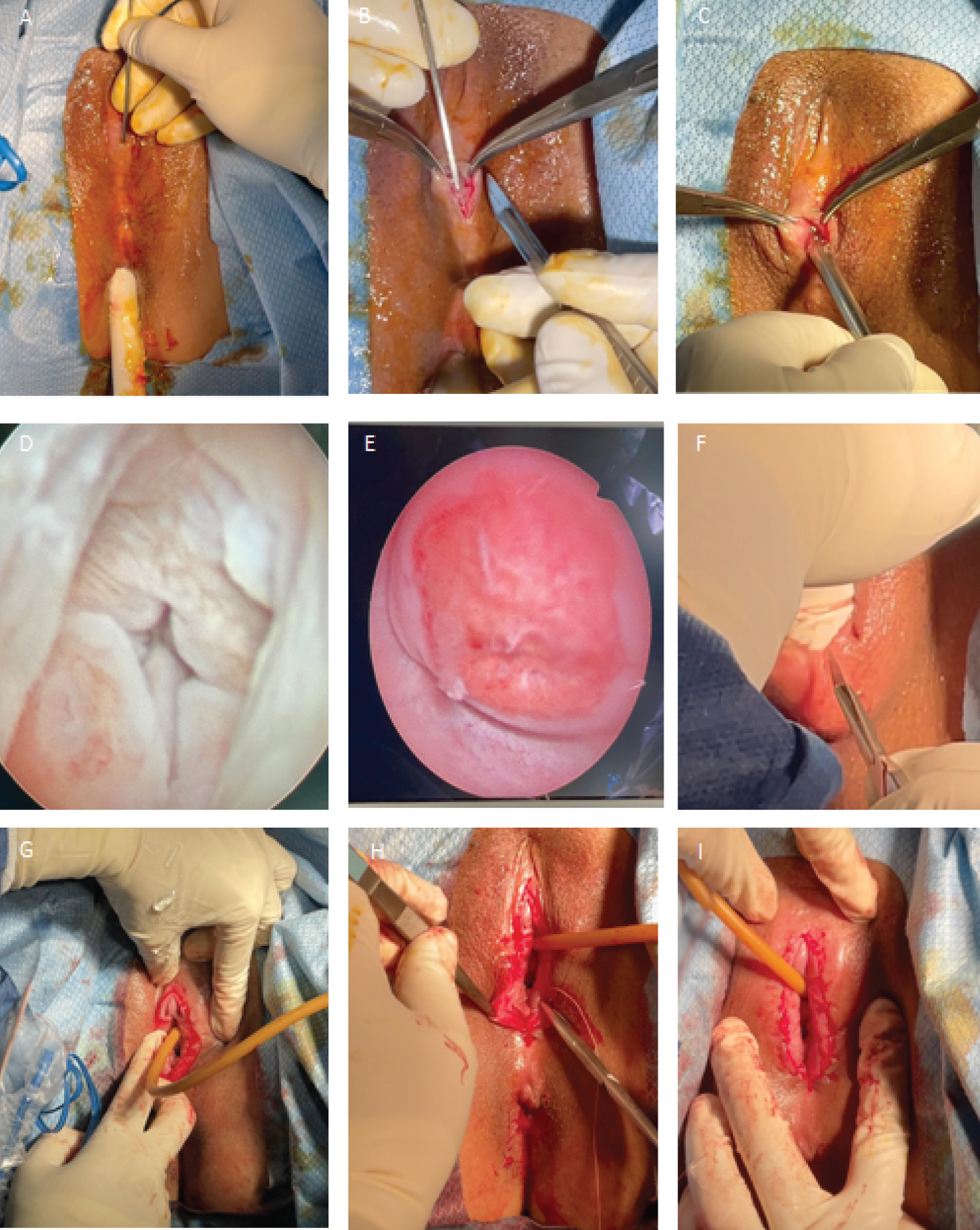 Figure 3: Vaginoscopy with incision of labial agglutination and repair. A) Upon identification of a pinpoint hole, 2 mm Hegar dilator was inserted vertically and downward until the superior portion of the posterior fourchette; B) Median raphe was sharply incised allowing enough room for the scope to pass through; C) Insertion of scope and vaginoscopy; D) Urethra; E) Cervix; F) Incision of labial agglutination, the labia majora and minora were noted to be fused. Labial tissue was held with curved Kelly forceps, with two fingers insinuating the tissue to be excised up to the superior portion of posterior fourchette; G) Sharp dissection was continued anteriorly towards upper border of labia. The clitoral hood, urethra and hymenal ring were eventually appreciated. Indwelling foley catheter insertion; H,I) The squamous epithelium of the labia minora and majora were sutured to the mucous membrane vestibule and repaired by interrupted stitches using Vicryl 4-0 suture.
View Figure 3
Figure 3: Vaginoscopy with incision of labial agglutination and repair. A) Upon identification of a pinpoint hole, 2 mm Hegar dilator was inserted vertically and downward until the superior portion of the posterior fourchette; B) Median raphe was sharply incised allowing enough room for the scope to pass through; C) Insertion of scope and vaginoscopy; D) Urethra; E) Cervix; F) Incision of labial agglutination, the labia majora and minora were noted to be fused. Labial tissue was held with curved Kelly forceps, with two fingers insinuating the tissue to be excised up to the superior portion of posterior fourchette; G) Sharp dissection was continued anteriorly towards upper border of labia. The clitoral hood, urethra and hymenal ring were eventually appreciated. Indwelling foley catheter insertion; H,I) The squamous epithelium of the labia minora and majora were sutured to the mucous membrane vestibule and repaired by interrupted stitches using Vicryl 4-0 suture.
View Figure 3
Post-operative application of petroleum jelly, antibiotic (Mupirocin ointment) and estrogen cream (Ovestin) were given for the following duration: one month, one week, and two weeks, respectively (Figure 4).
 Figure 4: Post-surgery documentation. A) First week; B) Second week; C) Third week; D) Fourth week; E) Eighth week; F) Twelfth week.
View Figure 4
Figure 4: Post-surgery documentation. A) First week; B) Second week; C) Third week; D) Fourth week; E) Eighth week; F) Twelfth week.
View Figure 4
Full labial healing was achieved after one month. The couple attempted sexual intercourse eight weeks post-surgery. Dyspareunia was experienced during the early attempts. Normal sexual intercourse was possible at ten weeks post-surgery. No dyspareunia, nor recurrence or persistence of labial agglutination were reported thereafter. Six months later, she conceived.
Labial agglutination is extremely rare in reproductive-age women [1]. In pre-pubertal girls, it occurs in 0.6 to 3.0%, and among them, the highest incidence is between 13-23 months of age at 21.3 to 38.9% [2]. In post-menopausal women, the incidence is unknown. The condition is multifactorial and mostly due to low or declining levels of estrogen. The etiology is related to local irritation and inflammation, especially in cases with decreased levels of estrogen [3].
Labial adhesion in reproductive age is unexpected and extremely rare due to adequate levels of estrogen. Therefore, in the reproductive-age group, the integrity of their HPO axis should be evaluated.
Oftentimes, it's found incidentally during a routine gynecologic examination. It can also present as gynecologic signs and symptoms prompting a consult with a gynecologist. Here, we describe a patient with adult-onset complete labial adhesion who was unbothered by the adhesions until she attempted intercourse. Etiological and contributing factors in older adult women are local inflammation, senile vaginitis, hypoestrogenism, lack of sexual activity, local trauma or sexual abuse, vaginal laceration following childbirth and recurrent UTI [4,5].
Various clinical presentations may occur, but it most commonly presents with a history of urinary tract infection, dysuria, incomplete voiding, urinary retention, hesitancy, dribbling [6] and absence of primary or secondary sexual penetration [7].
Choice of diagnostics is key in properly describing the pathology. Ultrasound appears to be a better alternative to MRI as the latter may be inferior at detecting subtle vaginal soft-tissue pathologies [8].
Several conditions can be considered in patients with labial agglutination. Antibiotics taken in the past for recurrent UTI could, in theory, predispose her to cutaneous adverse drug reactions. However, she did not report any related symptomatology such as flu-like symptoms and skin manifestations related to Stevens-Johnson syndrome [9]. Systemic Lupus Erythematosus was ruled out after confirmatory tests yielded negative results [10]. Clinical history ruled out local injury from trauma, sexual abuse, or scarring from birth injury.
Recurrent urinary tract infection is more commonly a result, rather than a cause of labial adhesions. However, the temporality of events and the patient's lack of any other predisposing factors point to an association with her urinary symptoms. It is possible that mucosal irritation secondary to an infectious process was the antecedent cause of scarring and agglutination. This clinical picture has yet to be reported in the literature and, because the exact etiology remains elusive, documentation and comparison with similar cases may lead to a better understanding of this condition.
There are different treatments for labial adhesions in pre-pubertal and postmenopausal women. It can be managed conservatively through topical estrogen treatment with or without manual separation of labia or surgery. However, in reproductive-age women with normal HPO function, surgery is the logical treatment choice.
Consent was obtained after thorough counseling regarding the surgical plan, risks, complications, and the recurrence rate post-surgery. According to Jurayyan [2], there is a 40% recurrence rate both for medical and surgical interventions.
A combination of topical antibiotics, estrogen, and emollients were helpful in reducing recurrence of adhesions. Improvement was noticeable on subsequent follow-ups. The result was similar to other studies [5]. Perineal hygiene and regular sexual intercourse were advised to prevent post-operative adhesions. Normal anatomy was achieved after 12 weeks. The patient's fertility, sexual function, and quality of life were markedly improved, and she conceived 6 months after the surgery.
Labial fusion during reproductive years should be carefully investigated as this is exceedingly rare and unexpected in reproductive-age women with normal hypothalamic pituitary ovarian (HPO) function. Issues of underlying predisposing factors need to be addressed and are necessary to prevent recurrence. History of recurrent UTI and absence of sexual penetration increases suspicion of a rare gynecologic condition.
I would like to express my deepest appreciation to my co-author Dr. Ma. Isidora Margarita Yap-Garcia for showing me the innate substance of the case and for providing a great amount of assistance.
None.
The authors declare no conflicts of interest and nothing to disclose.
All authors have contributed equally.