Background: Abdominal defects resulting from emergency open abdominal (OA) procedures require complex treatment algorithms and continue to burden both patients and healthcare providers due to increased risk of morbidity and complications. When primary closure of the abdominal subcutaneous and dermal tissues cannot be achieved, negative pressure wound therapy (NPWT) is among the most common treatment options. While biologic hernia meshes are often deployed to reinforce the abdominal wall or bridge fascia, the use of biologic grafts to specifically aid granular infill of abdominal defects is less reported.
Methods: This retrospective, observational case series (n = 3 abdominal defects) presents the authors' initial experience using a biological graft, ovine forestomach matrix (OFM), with and without NPWT to aid tissue infill of abdominal defects post OA surgery. De-identified data was collated via the electronic medical record and results reported herein.
Results: The mean time to 100% graft integration was 19.3 ± 0.9 days with a mean overall healing time of 9 ± 2 weeks, with no complications to a mean follow-up of 50 ± 14 weeks. Concomitant NPWT usage, with weekly NPWT dressing changes had a mean healing time of 3.7 ± 0.9 weeks.
Conclusion: These initial findings demonstrated that OFM graft especially when used concomitantly with NPWT is safe and may decrease the overall time to healing of complex abdominal defects resulting from emergency OA surgery.
Extracellular matrix, Ovine forestomach matrix, Soft tissue trauma, Open abdomen, Volumetric tissue loss, Laparotomy
OA: Open Abdomen; NPWT: Negative Pressure Wound Therapy; OFM: Ovine Forestomach Matrix; STSG: Split-Thickness Skin Graft; WTD: Wet-to-Dry; MLL: Morel Lavallee Lesion
Although open abdomen (OA) is a often used for “damage control” of catastrophic intra-abdominal injuries, it is typically associated with high complications rates and poor outcomes [1,2]. Closure of the OA typically proceeds with primary closure of the abdominal wall fascia that may be reinforced with a synthetic or biological surgical mesh. Ideally, the abdominal subcutaneous and dermal tissues are primarily closed but a large number of patients have either insufficient or contaminated tissue and are therefore left with significant soft tissue defects requiring delayed repair and/or regeneration. These abdominal defects are often defined by large and irregular wound beds. While there are a variety of pedicled and free flap reconstruction techniques available, these approaches are surgically complex with high donor site morbidity, so they are rarely indicated after damage control surgery [3]. Currently, NPWT is a mainstay to promote granulation tissue and expedite wound healing in abdominal defects [4]. NPWT can provide coverage to exposed viscera, protect the site from bacterial contamination, and manage wound exudate all while stimulating formation of granulation tissue [5]. Abdominal wounds managed with NPWT may ultimately be closed via a split thickness skin graft (STSG), or by secondary intention following standard wound care. Management of abdominal defects with NPWT has consistently led to improved wound closure rates compared to standard wound care methods such as wet-to-dry (WTD) or other standard daily dressing changes [6]. Despite these advantages, NPWT duration and management still places a significant burden on patients and health care teams. In order to achieve improved and increased abdominal wound healing, Seidel, et al. [7] reported an average NPWT treatment duration of 14.6 ± 9.1 days. In a retrospective review of 37 full thickness abdominal wounds, DeFranzo, et al. [8] reported an average NPWT treatment duration of 18 days (range; 11-25 days). These studies prove that it is valuable to both patients and the healthcare system to continue to explore strategies that reduce the duration of NPWT management of abdominal wounds. Reduced healing time not only leads to reduced costs of care but also improves patients’ quality of life [9-11]. Biologic meshes were originally used for hernia and OA surgery with contaminated fields, but have largely been replaced by a synthetic mesh or by choosing to forego the use of a mesh largely due to suboptimal clinical outcomes and cost of biologic meshes [12,13]. In these cases, it is necessary to consider how to facilitate expedited subcutaneous tissue healing with the plan of a delayed and definitive closure technique. Cutaneous tissue regeneration using mammalian tissue derived biologic grafts are now an established part of the reconstructive ladder [14,15]. The use of these biologic grafts extends to a variety of complex and often contaminated wounds, including abdominal wounds [16,17]. In complex wound reconstruction, biologic grafts are often used concomitantly with NPWT, and studies have shown that concomitant use can shorten the overall healing time [9-11,18]. Biologic meshes were originally used for hernia and OA surgery with contaminated fields, but have largely been replaced by a synthetic mesh or by choosing to forego the use of a mesh largely due to suboptimal clinical outcomes and cost of biologic meshes [12,13]. In these cases, it is necessary to consider how to facilitate expedited subcutaneous tissue healing with the plan of a delayed and definitive closure technique. Cutaneous tissue regeneration using mammalian tissue derived biologic grafts are now an established part of the reconstructive ladder [14,15]. The use of these biologic grafts extends to a variety of complex and often contaminated wounds, including abdominal wounds [16,17]. In complex wound reconstruction, biologic grafts are often used concomitantly with NPWT, and studies have shown that concomitant use can shorten the overall healing time [18].
Ovine forestomach matrix based biologic grafts are now routinely utilized in soft tissue regeneration across a range of contaminated defects including hidradenitis suppurativa [19], pilonidal sinus [20], chronic lower extremity defects [21,22] and necrotizing soft tissue infections [23]. In the search for new cost-effective options to improve healing of contaminated traumatic wounds the authors has begun to use OFM-based biologic grafts in combination with NPWT across a range of complex soft tissue defects. In this case report, we examine our initial experience using OFM-based grafts in conjunction with NPWT to treat complex abdominal defects resulting from emergency OA surgery.
The case report included three consecutive patients (n = 3) that had undergone reconstruction of abdominal defects resulting from OA surgery using OFM-based grafts during the period November 2021 to June 2022 at a single facility. OFM in either graft (Myriad Matrix Soft Tissue Bioscaffold™, Aroa Biosurgery Limited, Auckland, New Zealand) or morselized (‘particulate’ or ‘powder’) format (Myriad Morcells™, Aroa Biosurgery Limited, Auckland, New Zealand) were used in accordance with the manufacturer’s instructions for use. Patients were given general anesthesia, the surgical site prepared with povidone-iodine (Betadine ® , Cumulus Pharmaceutical LLC, and Cheyenne, WY, USA) and the patient surgically draped. The abdominal defects were thoroughly debrided to remove all necrotic tissue and lavaged with sterile saline. Defect dimensions and depth were recorded with a surgical ruler post-debridement. Utilization of either the OFM graft (3- or 5-layer), morselized OFM, or a combination of the two products was based on clinical judgement of the attending surgeon. The OFM devices were rehydrated (< 5 mins, sterile saline), trimmed to size as required and fixed to the defect edges or subcutaneous tissues in instances of undermined tissue with either suture or staples. The defects were subsequently dressed with a non-adherent petroleum-based contact layer (Xeroform ® , McKesson Medical-Surgical, Irving, TX, USA), then NPWT interface black foam, and NPWT system (V.A.C. ® , 3M/KCI, St. Paul, MN, USA). NPWT systems were set to 125 mmHg, and dressings changed every 5-7 days. At the discretion of the surgical team, definitive closure of each defect was achieved via STSG or secondary intention, according to institutional protocols.
A 49-Year-old male with morbid obesity, bipolar disorder, and history of drug use presented after a high-velocity motor vehicle accident with acute hypotension, ruptured liver and bladder requiring two damage-control laparotomies. Fascia was closed three days following a second exploratory laparotomy with the subcutaneous tissue remaining open. Five days after fascial closure, the patient was undergoing dressing change and the fascial closure was found to have partially dehisced (Figure 1a), and the decision was made to apply OFM particulate at the bedside in the ICU due to the patient’s poor medical state. Prior to application of the OFM, the defect was irrigated with Betadine ® solution and saline. Post debridement the defect involving the subcutaneous and cutaneous tissues measured ~31 cm × 7 cm × 4 cm (Figure 1a). A single application of morselized OFM (1000 mg) was applied to the base of the defect and rehydrated in situ with sterile saline and blood (Figure 1b). The defect was dressed with a petroleum-based contact layer and standard NPWT (125 mmHg) was placed. NPWT was used for 2 weeks, with weekly dressing changes. Complete integration of the OFM was achieved in 21 days, with the regenerated tissue being flush to the level of adjacent skin (Figure 1c). Definitive closure was achieved by secondary intention at 6 weeks resulting in functional soft tissue with satisfactory contour restoration and no complications (Figure 1d). The patient subsequently underwent planned ventral hernia repair at 20 weeks. Abdominal cutaneous tissues previously regenerated with OFM were sufficiently robust to allow for primary closure following hernia repair and healing was uneventful and without complication. No recurrence was noted at last follow-up (70 weeks).
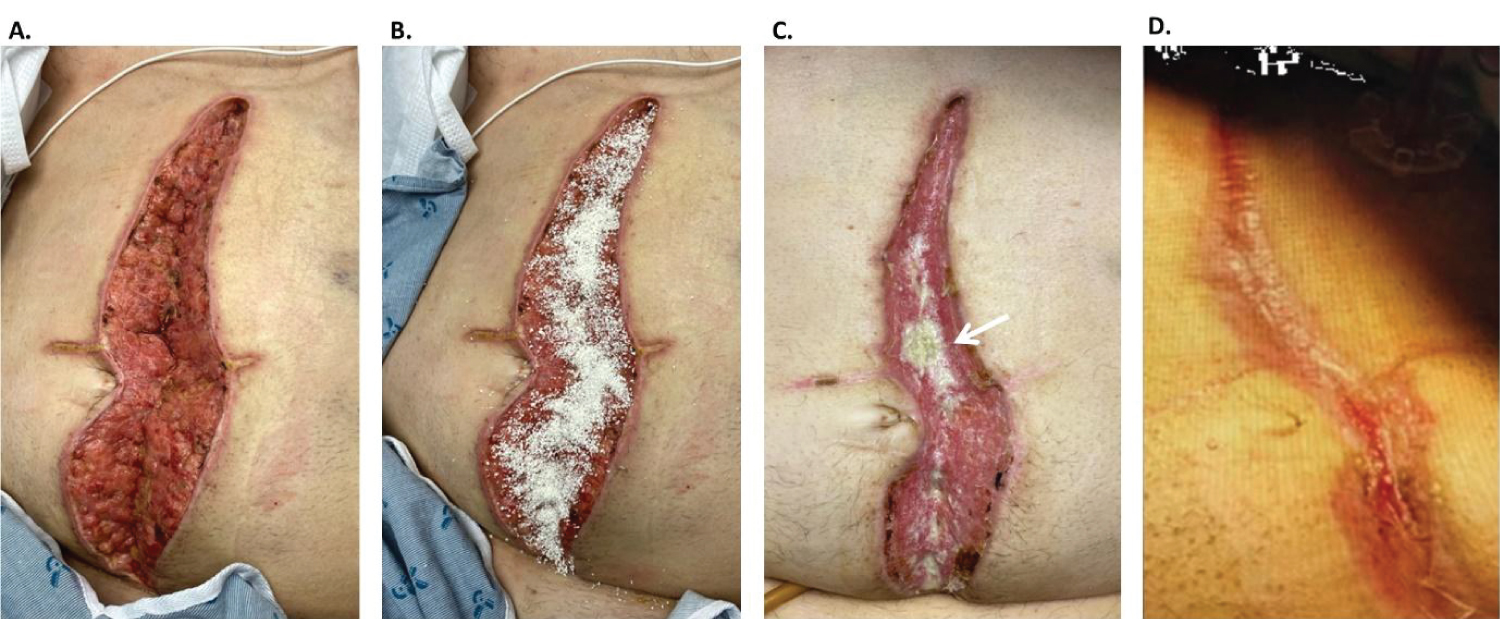 Figure 1: Case 1, open abdominal defect following MVA and multiple damage-control laparotomies: (a) Intra-operative, post debridement; (b) OFM particulate applied to the bed of the OA defect, prior to rehydration; (c) Week 3. Infill of the defect and graft integration. A small area of residual graft (white arrow) was present; (d) Week 6. Closure via secondary intention.
View Figure 1
Figure 1: Case 1, open abdominal defect following MVA and multiple damage-control laparotomies: (a) Intra-operative, post debridement; (b) OFM particulate applied to the bed of the OA defect, prior to rehydration; (c) Week 3. Infill of the defect and graft integration. A small area of residual graft (white arrow) was present; (d) Week 6. Closure via secondary intention.
View Figure 1
A 67-Year-old female with morbid obesity, history of stroke, and dementia presented after a motor vehicle accident requiring an initial exploratory laparotomy with findings of multiple mesenteric lacerations and ischemic bowel. The abdomen was left open, and then closed to the level of the fascia two days later following a right hemicolectomy and small bowel resection. NPWT was placed to manage the defect involving the sub-cutaneous tissues. Three days later a subsequent open procedure was undertaken to further resect small bowel, perform a colo-enteric anastomosis, and loop ileostomy, with closure to the level of the fascia and NPWT (Figure 2a). To follow, the patient required four serial washouts and debridement of subcutaneous tissue due to lack of improvement and areas of tissue necrosis. The patient continued to be managed with NPWT. After 17 days without improvement, OFM particulate (500 mg) and graft (5-layer, 10 × 20 cm) were placed in the defect (~16 cm × 8 cm × 6 cm) involving the subcutaneous tissues (not shown). Prior to graft placement the defect was irrigated with Betadine ® solution and saline, then the graft rehydrated (saline), trimmed as needed and secured with absorbable suture. The graft was further bolstered to the underlying defect with NPWT (125 mmHg). Ten days later, a large Morel-Lavallee lesion (MLL) of the right abdomen was noted, likely from the seatbelt at the time of trauma. This large volumetric abdominal defect ultimately communicated with the previous midline defect. The MLL was opened via a transverse incision (Figure 2b), and OFM placed to address the MLL (~20 × 10 × 6 cm). OFM particulate (500 mg) was first placed in the base and tunneled areas of the MLL and rehydrated with exudate. OFM graft (5-layer, 10 × 20 cm) was then placed on top the particulate hydrated with saline, and semi-implanted with partial closure. The entire defect was dressed with NPWT (125 mmHg). Three days later, the MLL was further explored, debrided and extended transversely (Figure 2c). OFM particulate (1500 mg) and graft (5-layer, 10 × 20 cm) were placed as previously described, and a partial closure of the MLL was achieved. The entire defect was dressed with a petroleum contact layer dressing and standard NPWT (125 mmHg), maintained for 4 weeks, with weekly dressing changes. Nineteen days following the third OFM application the wound bed had granulated and at week 5 the transverse MLL defect of the right side had been eradicated (Figure 2d), and the original midline defect was filled with granulation tissue to the height of the surrounding skin. Definitive epithelialization was achieved by secondary intention at 13 weeks resulting in functional soft tissue coverage with satisfactory contour restoration and no major complications (Figure 2e and Figure 2f). Of note, a small area of dehiscence was noted, but subsequently healed with outpatient local wound care in 3 weeks. No recurrence was noted at last follow-up (23 weeks).
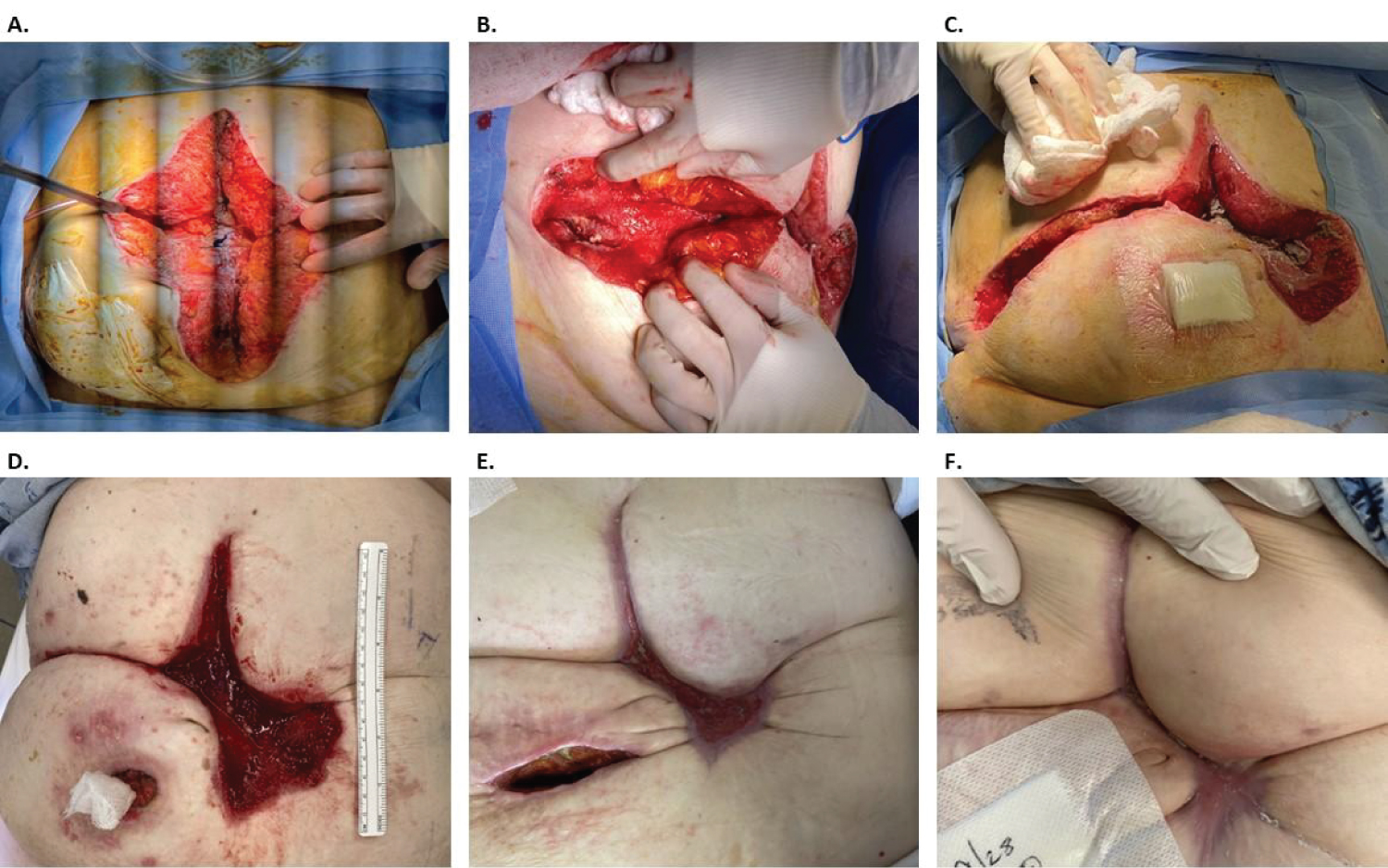 Figure 2: Case 2: (a) Open abdominal defect following multiple laparotomies and closure to the level of the fascia; (b) Exploration of the MLL transverse to the original mid-line defect, and prior to OFM graft placement; (c) Further exploration of the MLL defect and prior to the second OFM graft application; (d) Week 5 eradication of the transverse MLL defect; (e) Week 7; (f) Week 13.
View Figure 2
Figure 2: Case 2: (a) Open abdominal defect following multiple laparotomies and closure to the level of the fascia; (b) Exploration of the MLL transverse to the original mid-line defect, and prior to OFM graft placement; (c) Further exploration of the MLL defect and prior to the second OFM graft application; (d) Week 5 eradication of the transverse MLL defect; (e) Week 7; (f) Week 13.
View Figure 2
A 51-Year-old male presented after high-velocity motor vehicle accident requiring multiple damage-control laparotomies to repair the diaphragm and bladder, as well as for a small bowel resection. The OA was initially closed at the level of the fascia and managed with NPWT. The patient had a small area of fascial dehiscence seven days after closure (Figure 3a). The decision was made to proceed with repair of the sub-cutaneous and dermal tissues, until the abdominal wall could be closed via a delayed planned ventral hernia repair. The defect was irrigated with Betadine ® solution and saline, prior to sharp debridement resulting in a defect measuring 24 cm × 4 cm × 2 cm (Figure 3a). OFM particulate (1000 mg) was applied directly to the defect (Figure 3b). OFM graft (10 × 20 cm, 3-layer) was placed to cover the entire defect (Figure 3c) and into the undermined areas and was secured with synthetic absorbable sutures. The defect was dressed with a petroleum-based contact layer dressing and standard NPWT (125 mmHg). NPWT was used for 5 weeks, with weekly dressing changes (Figure 3d). Complete integration of the OFM device was achieved by day 18. Definitive epithelialization was achieved by STSG applied at week 7, with 100% stake of the STSG at one week. Long term follow-up at 16 weeks showed the defect was restored with functional tissue coverage, until planned ventral hernia repair could be completed (Figure 3e). There were no complications or recurrence at last follow-up (57 weeks). The patient ultimately underwent a planned ventral hernia repair at 41 weeks following re-epithelialization and was uneventful and without complications.
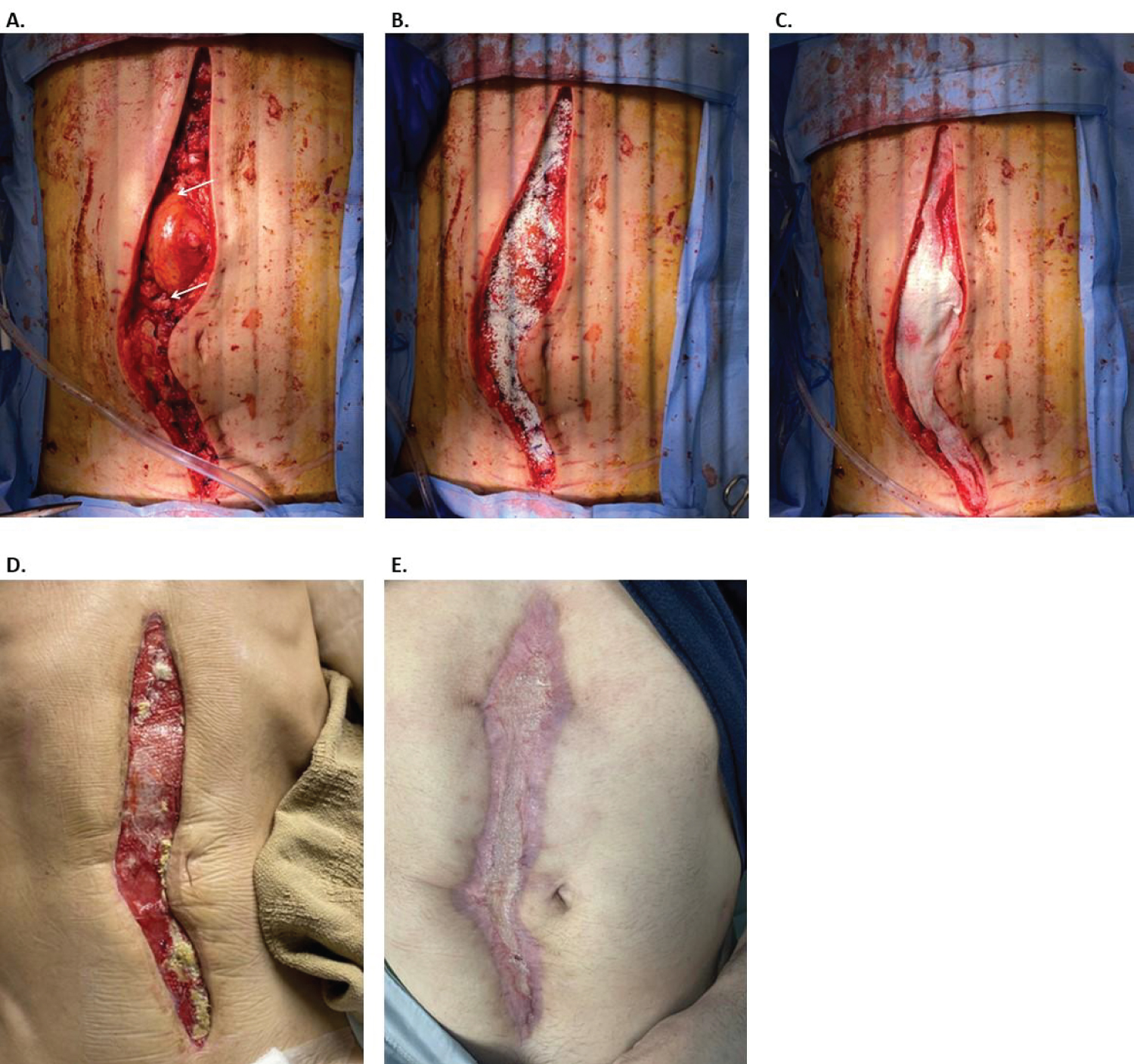 Figure 3: Case 3, Open abdomen due to multiple damage-control laparotomies: (a) Intra-operative post debridement. Prior primary closure to the level of the fascia had dehisced leaving a small area of exposed viscera (indicated between the two white arrows); (b) Application of OFM particulate (1000 mg); (c) Application of OFM graft (10 × 20 cm, 3-layer); (d) Week 5; (e) Long term follow-up at 16 weeks, 9 weeks post application of a STSG.
View Figure 3
Figure 3: Case 3, Open abdomen due to multiple damage-control laparotomies: (a) Intra-operative post debridement. Prior primary closure to the level of the fascia had dehisced leaving a small area of exposed viscera (indicated between the two white arrows); (b) Application of OFM particulate (1000 mg); (c) Application of OFM graft (10 × 20 cm, 3-layer); (d) Week 5; (e) Long term follow-up at 16 weeks, 9 weeks post application of a STSG.
View Figure 3
OA commonly occurs after damage-control of catastrophic intra-abdominal injuries, but the long-term management and outcome potential of these defects continues to be a challenge in trauma and emergency general surgery. Many strategies have evolved to close the fascia including vacuum-assisted closure, mesh-mediated fascial traction, dynamic wound closure system and fascial bridging [24]. Fascial defects after OA surgery occur either as the result of dehiscence after primary closure or from a lack of tissue to achieve primary closure. The resultant abdominal defect presents a challenge to the surgical team as do all large volumetric wounds involving potentially contaminated and inflamed soft tissues. Granulating the abdominal defect is the primary focus to enable either coverage by secondary intention or by placement of a split thickness skin graft. NPWT has been used extensively to encourage the formation of well vascularized tissue over these abdominal defects. Often NPWT is used in conjunction with various surgical meshes which can be placed to reinforce or bridge the fascial defect. Many studies have been presented in the literature describing this approach [25,26], however complete healing of the abdominal defects have been reported to take 6 months or more [27]. The use of biologic grafts to aid regeneration of abdominal cutaneous tissues doesn’t replace the need for surgical meshes to reinforce the abdominal wall post OA surgery. Rather the intent of biologic grafts, overlaid on the fascia and/or subcutaneous tissues is to aid formation of robust granulation tissue to cover the abdominal defect. Many of these defects will require complex abdominal wall reconstruction techniques in the future for definitive fascial closure. There are very few reports in the literature describing the application of biologic grafts to accelerate vascularized tissue formation within abdominal defects, prior to definitive closure. Puckett, et al. [16] described healing of abdominal defects with the biologic graft, urinary bladder matrix. In their retrospective case series, the authors described initial fascial closure with a dynamic wound closure system, and then once fascial closure was achieved, powdered biologic graft and sheet were applied to the primary myofascial closure and subcutaneous tissue. Abdominal defects were then covered with NPWT, with a reported healing rate of approximately 8 weeks across 50 patients. Single case reports have been published using porcine dermal graft after abdominal wall dehiscence [17] and fish-skin graft in a partial thickness abdominal dehiscence [28].
In this retrospective case series, we present the successful treatment of three consecutive abdominal defects resulting from OA defects where OFM grafts were used to regenerate well vascularized granulation tissue. In these instances, the fascial tissue had already been primarily closed. In all three cases, the defects were at or beyond the level of the fascia, clean-contaminated (Grade 2) and in one case, there was exposed viscera due to partial dehiscence (Case 3). The mean time to complete integration of the graft was 19.3 ± 0.9 days. One patient received a split thickness skin graft at week 7 and the mean time to compete healing across all three cases was 9 ± 2 weeks, with no complications to a mean follow-up of 50 ± 14 weeks. Case 1 and 3 required only a single application of the OFM graft. Case 2 received three separate applications of the OFM grafts, not due to graft failure or lack of incorporation but due to extension of the initial defect after revealing the interconnected MLL.
There is some controversy in the literature as to the true effectiveness of NPWT in the management of OA defects and the ability to facilitate faster time to closure, but regardless, there are noteworthy increases in cost when utilizing NPWT [29]. It is postulated that by using a biological graft to expediate tissue regeneration providers can potentially reduce the number of dressing changes and overall duration of NPWT, thereby reducing financial burden for patients and facilities alike [30]. The use of biologic grafts adjunctively with NPWT to synergistically improve wound healing trajectory has been widely described in the scientific literature [31-33], and shorten the duration of NPWT use [34]. Across our current cases the concurrent NPWT usage ranged from 2-5 weeks with a mean of 3.7 ± 0.9 weeks. We note that our current approach to concomitant NPWT utilization with OFM grafts adhered to NPWT dressing change frequency of 5-7 days, whereas other published protocols report a dressing change frequency of up to 2 days using a porcine urinary bladder matrix graft [16].
Abdominal defects resulting from OA surgery are often contaminated [35]. The success of OFM in reconstructions involving contaminated fields, such as abdominal defects, may be attributable to its ability to form well-vascularized tissue [36] while concurrently modulating wound proteases that are known to prolong inflammation [37]. This, in theory, should allow the patient’s native immune system to primarily fend off microbial contamination thereby minimizing clinical infection and ultimately facilitating progression of the defect to definitive closure [38].
This study is comprised of observations from a single center with all the other limitations of a retrospective case series such as small sample size and no comparative cohort group. While the results of this case series are promising, there is a need for future research to expand the number of patients to validate these initial results. Future studies may involve a controlled prospective study design with an aim to compare the overall healing rates, complications, including herniation and fascial dehiscence, and NPWT utilization when used in combination with OFM grafts.
This case series builds on a growing body of evidence that OFM can be utilized to facilitate the formation of robust, well-vascularized soft tissue in large contaminated volumetric soft tissue defects and reduce complications. The OFM grafts were shown to complement existing NPWT protocols and may reduce the frequency of dressing changes associated with NPWT usage in abdominal soft tissue defects.
The authors wish to acknowledge Aroa Biosurgery Limited for editorial assistance in preparing this manuscript. We thank the efforts of the nurses and surgical team of WellStar Kennestone Hospital.
No funding was provided for this study. RT is a consultant for Aroa Biosurgery Limited.
All authors contributed significantly and equally to the direct patient care, collation of retrospective data, data analysis, and development of the manuscript.