Apixaban is an oral anticoagulant that directly inhibits Factor Xa and is indicated for the prophylaxis and treatment of deep venous thrombosis and stroke prevention in non-valvular atrial fibrillation. Acute lower extremity Posterior Compartment Syndrome is a rare complication of Apixaban use. We present a 78-year-old male with significant medical morbidities taking Apixaban for Atrial Fibrillation presenting with post-traumatic extensive hemorrhagic bullae on the left proximal pretibial region secondary to anticoagulation. We recommend that clinicians develop awareness of the potential for serious bleeding complications of anticoagulants and devise strategies to identify the need for early recognition and prompt management.
Compartment Syndromes, Factor Xa Inhibitors, Fasciotomy, Apixaban
Acute Compartment Syndrome is a surgical emergency for which a delay in diagnosis can result in significant limb morbidity, including irreversible nerve and muscle damage and rhabdomyolysis [1]. Prompt diagnosis of ACS relies on a suggestive history and the presence of typical physical exam findings, as well as the measurement of compartment pressures [2-4]. A rare etiology of ACS is intra-compartmental hemorrhage [3]. Anticoagulants are the leading cause of adverse drug reactions leading to hospitalization secondary to hemorrhage. We present a 78-year-old male with atrial fibrillation on long-term anticoagulation with Apixaban presenting with post-traumatic extensive hemorrhagic bullae on the left proximal pretibial region which progressed to compartment syndrome.
A 78-year-old male presented to the ED for left lower extremity pain, swelling, and rapidly enlarging hemorrhagic blisters three days after he fell and scraped his left knee at an airport. His past medical history is significant for multiple comorbidities, notably Type II Diabetes Mellitus and Atrial Fibrillation managed with Apixaban. On day of incident, patient scraped his left knee with minimal reported pain.
Initial examination in the ED showed left lower extremity wound progression distally with extensive blistering, draining bloody fluid. The anterior lower leg distal to knee was extremely tender to light palpation with extensive bruising with in duration extending from point of impact proximally to the left thigh (Figure 1B). On presentation, patient was tachycardic, afebrile and without leukocytosis. Foot and distal left leg were neurovascularly intact. CT of the lower extremity demonstrated edema of the subcutaneous compartments initially suggestive of cellulitis (Figure 1A). Patient was started on empiric coverage for necrotizing fasciitis with suspicion of Vulnificus Vibrio with oral Doxycycline and Ceftriaxone, which were discontinued after wound cultures revealed no organism growth. During fasciotomy, a large posterior hematoma was found to dissect soft tissues across fascial planes resulting in compression syndrome of the posterior muscular compartments. Pale ischemic changes of the gastrocnemius and soleus musculature were visualized. Given that patient had atrial fibrillation CHA2DS2-VASc score of 6 and heart rate of 120 pre-operatively, debridement interventions placed patient at low risk for significant bleeding. Patient was treated with Metoprolol Succinate to maintain heart rate below 110 beats per minute. Apixaban was restarted on postoperative day one. Multiple debridement operations were performed and split-thickness skin graft was applied. Patient's wound healed well at one month reevaluation.
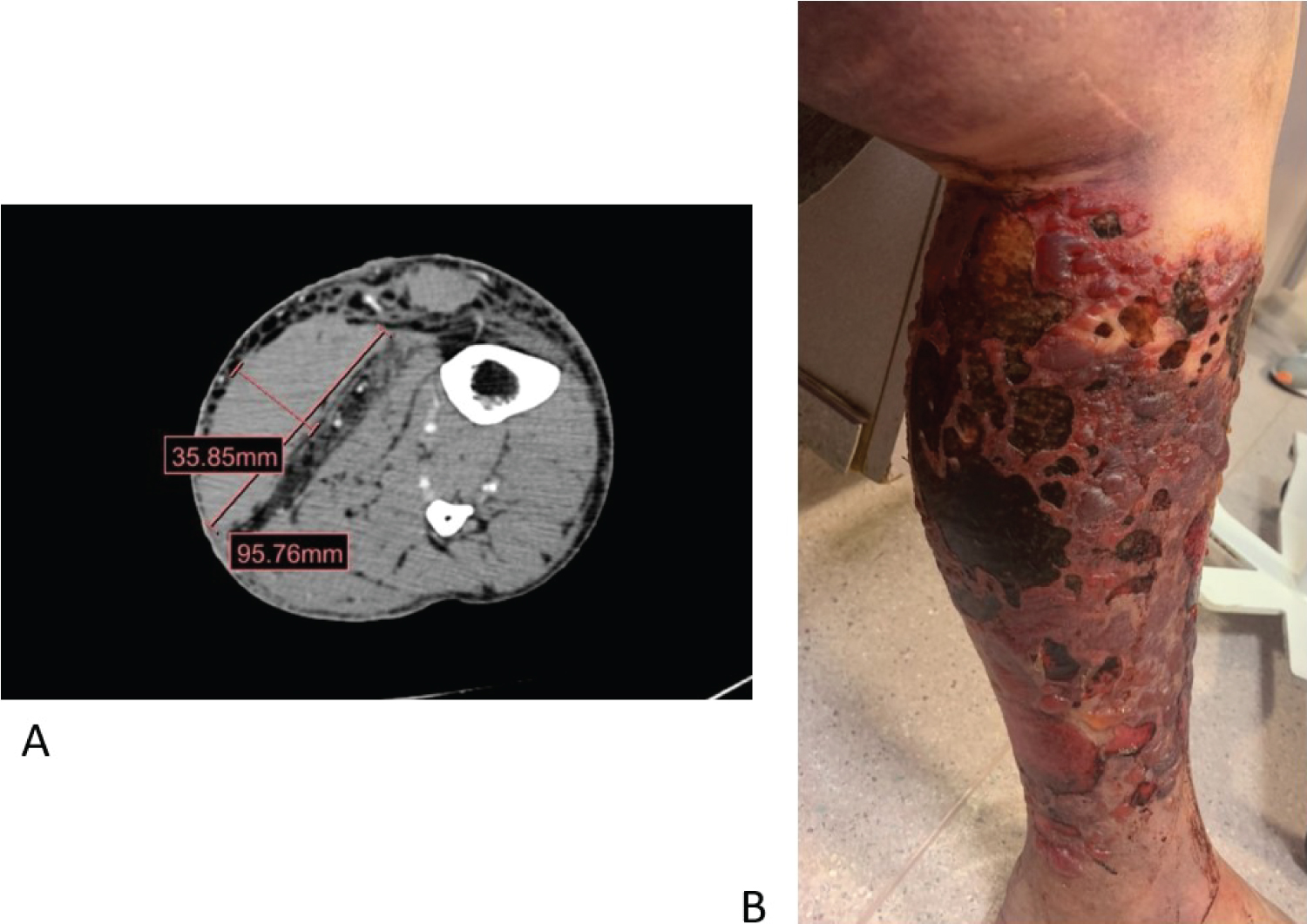 Figure 1: (A) CT of the lower extremity demonstrated edema of the subcutaneous compartments initially suggestive of cellulitis; (B) The anterior lower leg distal to knee was extremely tender to light palpation with extensive bruising with in duration extending from point of impact proximally to the left thigh.
View Figure 1
Figure 1: (A) CT of the lower extremity demonstrated edema of the subcutaneous compartments initially suggestive of cellulitis; (B) The anterior lower leg distal to knee was extremely tender to light palpation with extensive bruising with in duration extending from point of impact proximally to the left thigh.
View Figure 1
Acute Compartment Syndrome is often described as a clinical diagnosis. The classic teaching is the five "Ps," including pain, pallor, paresthesia, paralysis, pulselessness and poikilothermia [5]. The earliest symptom is severe pain out of proportion to the physical findings, which our patient exhibited. However, these classic findings have been shown to be unreliable and often indicate late disease with poor prognosis [5].
ACS commonly occurs secondary to soft tissue injury following a fracture [6] but has also been reported following moderate or minimal exercise [7-9]. This wide variety of injury patterns suggests that a high degree of suspicion for ACS is necessary even in patients without high energy mechanism of injury. Non-traumatic cases of ACS associated with anticoagulant use have been reported. Phillips, et al. described a case of atraumatic gastrocnemius rupture in a 56-year-old man on rivaroxaban [10] resulted in significant intra-compartmental bleeding, severe ACS which necessitated four compartment fasciotomy.
Anticoagulants are widely prescribed and used frequently in hospital and outpatient settings to prevent and treat thromboembolism, but double the risk of hemorrhagic complications [11]. Apixaban is popular direct-acting oral anticoagulant (DOAC) that works by selectively inhibiting both free and prothrombinase complex-associated factor Xa [12]. While apixaban shows lower rates of hemorrhage than warfarin, it still poses a risk to patients with hypertension, congestive heart failure and alcoholism [9,11,13]. We hypothesize that the etiology of ACS in our patient was a soft tissue lower extremity hematoma that expanded secondary to Apixaban use.
This case highlights the importance of a multidisciplinary team-based approach to patients on NOACs requiring surgery. Physician awareness that one complication of prolonged DOAC-use is bleeding into fascial compartments leading to ACS is critical. We feel that there is a need for further development of evidence-based guidelines for managing these patients in the acute setting.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent had been obtained from the patient for publication of the case report and accompanying images.