Pertussis is a drawn-out and troublesome respiratory disease. Infants have a greater burden of disease than older children and adults, and are more likely to suffer complications. New vaccination strategies need to be considered to reduce pertussis among infants. The aim of the study was to evaluate cost-effectiveness of three alternative vaccination strategies, in comparison with current vaccination schedule.
A decision-analytic model was developed to estimate the effect of different vaccination strategies on an average birth cohort in Sweden, with a time-horizon of one year. The following strategies were evaluated: 1) Cocooning, 2) Maternal vaccination, and 3) On-schedule vaccination. The main outcome was cost per gained quality-adjusted life year (QALY), i.e. the incremental cost-effectiveness ratio (ICER). Sensitivity analyses were performed on key assumptions in the model; including annual incidence of pertussis among infants and the cost of vaccination.
Cocooning and maternal vaccination result in an ICER of 240,000 euro and 66,000 euro respectively, whilst on-schedule vaccination is a dominant strategy in comparison with current vaccination schedule, i.e. have a better effect at a lower cost. The results from the three analyses are sensitive to assumptions on annual incidence. The results for cocooning and maternal vaccination are sensitive to the price of the vaccine and vaccination coverage among parents.
On-schedule vaccination would be a cost-effective and even cost-saving strategy compared to current vaccination schedule. The cocooning and maternal vaccination strategies would not be cost-effective assuming a willingness-to-pay of 50,000 euro. However, sensitivity analyses showed that a marginally increased incidence would make the maternal strategy cost-effective, and a three-folded increase would make the cocooning strategy cost-effective. Alternatively, a vaccine price reduction of 20% would make the maternal strategy cost-effective, while the required reduction for the cocooning strategy would be 80%.
Pertussis, Vaccination, Decision-analytical modelling, Cost-effectiveness, Health economic evaluation
Pertussis is caused by the bacteria Bordetella pertussis and is a drawn-out and highly contagious respiratory infection [1]. The infection is usually severe in incompletely vaccinated or unvaccinated infants (children less than 12 months old), who suffer the most severe complications such as apnea and are more likely to be hospitalized than older children and adults [2-9].
Pertussis is resurgent globally [10,11], with different pattern and time-points for the resurgence in different countries. Countries in North America and Europe with consolidated high vaccination coverage have observed re-emergence of pertussis [12-18]. The increase implies that there is a need for improved vaccination strategies to protect infants from pertussis [19,20]. Subsequently, the UK and the USA have implemented new vaccination strategies [21,22], such as vaccinating adults in close contact with infants too young to be fully immunized against pertussis ("cocooning strategy") and vaccinating pregnant women.
In Sweden, pertussis is a notifiable disease and all reported cases are contact traced [23]. After several years of stable low incidence of pertussis in Sweden, 688 cases were reported in the enhanced surveillance study in 2014. This is more than a threefold increase compared with 2013 (223 cases). This threefold increase applied to the majority of age groups. As in previous years, infants had the highest incidence in 2014 (105.3 cases per 100,000 individuals), and the majority of the infants (103 of 122 cases, 85%) had pertussis before the age of five months. In 2014, two children died due to pertussis, both unvaccinated and younger than 3 months [24].
In contrast to many European countries, there was no vaccination against pertussis included in the Swedish national immunization program (NIP) during 1979-1996. The withdrawal of the whole-cell pertussis vaccine in 1979 was due to concerns about its safety and efficacy. Based on good efficacy and safety data, acellular vaccines were approved in Europe in 1996 and since then vaccination against pertussis has been a part on the Swedish NIP [18]. Today, about 98% of all children receive vaccination against pertussis when they are 3, 5 and 12 months old, and a booster dose at the age of 5-6 years [25].
The objective of this study was to evaluate the potential cost-effectiveness of alternative pertussis vaccination strategies in comparison with current vaccination schedule, given the recent increase in pertussis. The alternative vaccination strategies that were investigated cocooning (i.e. vaccination of both parents), maternal vaccination, and on-schedule vaccination (i.e. no delay in the vaccination schedule) Figure 1.
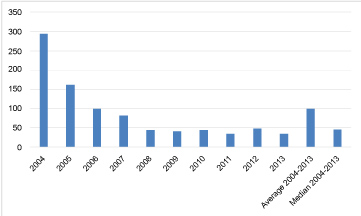 Figure 1: Incidence per 100,000 infants (< 12 months) based on the number of reported cases of pertussis among infants 2004-2013.
View Figure 1
Figure 1: Incidence per 100,000 infants (< 12 months) based on the number of reported cases of pertussis among infants 2004-2013.
View Figure 1
Since 1997 all cases of pertussis, either clinically suspected and/or laboratory confirmed by culture, polymerase chain reaction (PCR) or serology, should be reported to the Public Health Agency of Swedena through a computer-linked reporting system, SmiNet [26].
aBefore 1st of January 2014 the Swedish Institute for Communicable Disease Control.The enhanced pertussis surveillance started in October 1, 1997. Cases reported according to the Communicable Disease Act of culture- and PCR- positive cases of pertussis in children born since January 1, 1996, enter the SmiNet data base automatically. In the enhanced surveillance study, additional information about these cases was then collected through structured telephone interviews with the parents of children diagnosed with pertussis using a standardized questionnaire. The clinical questions included type and duration of cough, presence of apnea and other complications, number and length of hospital admissions, and timing of antibiotic treatment if given, and vaccination dates. If medical record was needed for complementary medical information, parents were requested for consents.
Detailed vaccination history for children born since 1996 was obtained from the medical records of the CHC or School Health Centers by telephone call to the nurse attending the individual child. With access to clinical information, data from the enhanced surveillance study were based on age at onset of symptoms, which is important when analyzing age-specific severity of disease in infants [18].
Three strategies were investigated the current vaccination schedule: 1) Cocooning, 2) Maternal vaccination, and 3) On-schedule vaccination. In the vaccination strategy "cocooning", both the parents of a newborn were assumed to be vaccinated just after childbirth, whilst "maternal" implies that just the mother was vaccinated during her third trimester. Both cocooning and maternal aim at protecting the newborn from infection transmitted from parents, and maternal also provides the newborn with maternal antibodies. Due to the withdrawal of the whole-cell pertussis vaccine, many of today's' parents are not vaccinated against pertussis. They may, however, have some protection due to natural infection. On-schedule vaccination could provide a sooner protection against infection for infants. A previous study found that the timeliness of pertussis vaccination decreased by dose number, were 8% of the children were more than 30 days late for their first dose. The corresponding numbers for the second and third dose is 31% and 24% [27].
Vaccination strategies 1 and 2 complement the current vaccination schedule, since the most common source of infection for infants is via parents or other members of the immediate family [28-32], whereas strategy 3 is an alternative to the current schedule. In the cost-effectiveness analyses, the three vaccinating strategies were compared with today's schedule, and the relative cost-effectiveness between the strategies was also commented on.
We constructed a decision-tree model to simulate the incidence and severity of pertussis among otherwise healthy infants (Figure 2) for the four scenarios; i.e. with today's schedule, cocooning, maternal, and on-schedule vaccination. Modeling was performed in Microsoft Excel 2013. Since the most severe cases of pertussis occur during a newborns first year, we applied a time-horizon of one year.
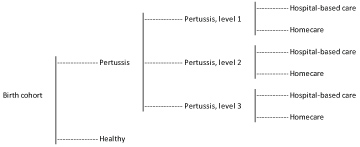 Figure 2: Flowchart of the decision-analytic model.
View Figure 2
Figure 2: Flowchart of the decision-analytic model.
View Figure 2
In the model, infants could either get ill with pertussis or stay healthy, i.e. an infant was considered healthy if it did not have pertussis, regardless of other diseases or complications. The severity of disease was divided into three levels; level one, two, and three, and the distribution was based on surveillance data. Level three, the most severe state, refers to infants with pertussis with respiratory complications, with or without apnea, dehydration with more than 5% weight loss, or other serious complications. Level two refers to infants with pertussis with coughing attacks that ends with vomiting several times a week or more, that cannot be classified as level three, and level one refers to infants with pertussis that cannot be classified as level two or three. An infant sick with pertussis could either receive hospital-based care or be cared for at home, dependent on the risk for hospitalization for each severity level.
We applied health related quality of life (HRQoL) and costs to each health state in the model. The outcome was measured as quality-adjusted life years (QALY), and the results presented as cost per gained QALY (ICER: incremental cost-effectiveness ratio). The model was run for four different scenarios, where the health effects and costs of scenario 1, 2 and 3 were compared to scenario 4 independently, the scenarios are thus considered mutually exclusive. Scenario 1 ("cocooning") describes the situation with cocooning, i.e. a situation where two caregivers are vaccinated in order to protect the newborn from infection. Situation 2 ("maternal") refers to maternal vaccination during pregnancy, and situation 3 ("on-schedule") a situation where there is no delay in the vaccination schedule - the first dose of the vaccine is given on exactly day 90 (Figure 2).
The model population corresponds to an average birth cohort in Sweden during the years 2004-2013 (109,089 infants) [33]. Swedish data on the incidence of pertussis was population-based. Pertussis is a notifiable disease in Sweden, and since 2004 it is also mandatory to perform contact tracing. All children and adults with clinical and laboratory-confirmed pertussis should be reported to the Public Health Agency. Since 1997 the Public Health Agency of Sweden conducts enhanced surveillance of pertussis, where a study nurse contacts all reported cases of pertussis and inquiries about onset of coughing and length of the disease [34]. Data on the current incidence, categorized by health state, and information on health care consumption was obtained from this enhanced surveillance [34]. We used the average annual number of cases during the years 2004-2013 in our analysis [35].
Table 1 presents the parameter values used in the model. Out of the total number of cases, 52% were assumed to have pertussis of level 1, 21% pertussis of level 2 and 27% pertussis of level 3, summing to 100%. The hospitalization risk was 35% for level 1, 44% for level 2 and 95% for level 3. All risks were derived from the enhanced surveillance data.
Table 1: Data input and assumptions in the model. View Table 1
The assumption on risk reductions from the alternative vaccinations strategies were collected from recent studies [3,27]; cocooning decreased the risk of pertussis with 48%, maternal vaccination with 67% and on-schedule vaccination with 28%. Among those infected, the distribution between level 1, 2, and 3 was the same as with current schedule. Also the hospitalization rate was the same for cocooning and maternal, whilst on-schedule vaccination was assumed to reduce the fraction of hospitalizations with 38% [27]. The reason for this inconsistency was lack of data, we only found studies that presented reduced hospitalization risks for on-schedule vaccination.
We assumed a vaccine coverage of 98% among infants and 60% among adults, strategy 1 and 2 [21,36-38]. We did not include mortality in the model, since pertussis related deaths are very rare and consequently the risk is hard to quantify. Nor did we include waning vaccine immunity, due to the short time-horizon (Table 1).
Health-related quality of life weights (HRQoL) for pertussis infection in combination with the duration of disease were used in order to estimate the QALY. The health related quality of life was dependent on the health state of a patient (i.e. level 1, 2 or 3 pertussis or healthy), and not on whether the patient received hospital-based care or not.
In the analysis, healthy infants had a HRQoL of 1, and when recovered they had no lasting disabilities, i.e. have a HRQoL of 1 as soon as they were well again. The decrease in HRQoL during pertussis was obtained from the literature [39,40]. The average length of illness was taken from the enhanced surveillance of pertussis [34] (Table 2).
Table 2: HRQoL and QALY weights in the model. View Table 2
The analysis applied a societal perspective in the base case analysis, i.e. it includes all direct medical costs as well as indirect costs in form of production losses among parents with children ill with pertussis.
Direct health care costs include the costs of vaccination and the cost for treatment of pertussis, both in-and outpatient costs. We excluded the cost for vaccinating infants, as this cost was the same in all vaccination strategies. Therefore, it did not affect the results since it cancels out in the incremental comparison between the strategies - a possible future change in the price of the vaccine for infants would thus not affect the cost-effectiveness.
Clinical experts at the Public Health Agency of Sweden assumed an average resource use for infants depending on their health state as well as if they were hospitalized or not. The average durations of disease and hospitalization were obtained from the enhanced surveillance of pertussis, years 2004-2013 [34].
The cost for one dose of the vaccine for adults with cocooning and maternal vaccination was 16 EURO (list price for DiTekiBooster) [41] (exchange rate 100 SEK = approximately 10 (10.36) euro [2018-10-02, Swedish Central Bank]). The direct vaccination costs of cocooning and maternal vaccination were calculated by multiplying the number of children in the birth cohort with the vaccine coverage among parents.
We assumed an additional cost of about 300,000 euro for educating vaccination nurses for the on-schedule vaccination strategy, based on the cost of educating 2,200 nurses (expert opinion).
The costs for resource use was mainly obtained from the Southern Healthcare Regions price list, and is presented as average cost per patient depending on health state, in Table 3 [42].
Table 3: Average cost per patient (infant with pertussis). View Table 3
Indirect costs were included in form of production losses incurred when parents had to stay home from work to care for their infant. We assumed that at least one of the parents were on parental leave and thus the production was not affected if a child was cared for at home. If the infant was hospitalized, however, we assumed that both caretakers needed to be available. Production loss was based on the average salary in Sweden in 2013 (adjusted with CPI 2014 and with the inclusion of social security costs of 31.42%) [43].
Deterministic sensitivity analyses were performed to investigate how varying the input parameters affected the results. We varied the incidence with current vaccination schedule, the price of the vaccine and the vaccination coverage as well as the effect of vaccinating parents, in one-way sensitivity analyses. Results from the sensitivity analyses are presented in the result section.
The three alternative strategies all resulted in both lower costs of treatment and lower indirect costs than the current vaccination schedule (Table 4). In addition, the three alternative strategies resulted in more gained QALY than with current vaccination schedule.
Table 4: Costs of health care and indirect costs of production losses and gained QALY with the alternative vaccination strategies and current schedule, and ICER for each strategy in comparison with today's schedule. View Table 4
On-schedule vaccination was a dominating strategy in comparison to the current schedule, i.e. had a better health effect at a lower cost. Maternal vaccination had an ICER of about 66,000 euro, and cocooning an ICER of about 240,000 euro (Table 4), compared to the current schedule. However, cocooning was dominated, since it gained fewer QALY at a higher cost than maternal. The ICER of maternal in comparison to on-schedule was about 30,000 euro.
The annual incidence of pertussis among infants was the variable that had greatest impact on the results. Therefore, we investigated the effects of using the median incidence instead of the average, lowering the incidence from 93 to 52.5. Finally, we investigated the effect of basing the incidence on the most recent data, from 2014, an incidence of 122. When the median incidence (52.5) was used instead of the average (93), the ICER increased to 450,000 euro for cocooning, 160,000 euro for maternal and 21,000 for on-schedule vaccination. When the most recent number of reported cases was used the ICER decreased to about 170,000 euro for cocooning and 40,000 euro for maternal. On-schedule vaccination was still dominant. This implies that the potential cost-effectiveness of a vaccination strategy are highly dependent on the number of cases that can be avoided - and are thus more favorable the higher the incidence among infants.
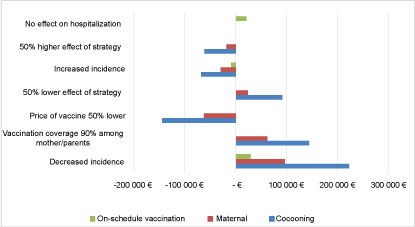 Figure 3: Diagram presenting the impact of different assumptions on the incremental cost-effectiveness ratio (ICER) of the different vaccination strategies in comparison with today's schedule as presented through deviation from base-case.
View Figure 3
Figure 3: Diagram presenting the impact of different assumptions on the incremental cost-effectiveness ratio (ICER) of the different vaccination strategies in comparison with today's schedule as presented through deviation from base-case.
View Figure 3
Varying the price of the vaccine to the caregivers had an impact on the results for the cocooning and maternal vaccination strategy. The price of the vaccine had to be lowered with more than 80% for cocooning to become a dominant strategy, and with about 50% for maternal vaccination to become dominant.
When the vaccine coverage among parents was increased to 90% (instead of 60%), the cost per gained QALY increased to 390,000 euro and 130,000 euro for cocooning and maternal respectively, due to a higher cost for intervention. The effect of cocooning and maternal vaccination had an impact on the results. As expected, the ICER increased for both cocooning and maternal when the effect decreased, and the ICER decreased when the effect increased.
When changing the assumption of a reduction in hospitalization with on-schedule vaccination, from a 38% reduction to no reduction at all, the strategy was no longer dominant and the ICER became 18,000 euro.
On-schedule vaccination was a dominant strategy in comparison to today's vaccination schedule. However, the possibilities to implement the strategy, i.e. to give infants in Sweden the first dose of the vaccine exactly 90 days after birth etc., may not be realistic, since such a strategy could be interrupted during summer holidays or weekends. This indicates that the decrease in incidence may not be as large as assumed in our analysis, which would affect the cost-effectiveness. Therefore, we focus on the results from the cocooning and maternal vaccination strategies in the discussion.
If we assume a willingness-to-pay for one gained QALY of 50,000 euro, the results show that neither cocooning nor maternal is cost-effective in comparison with today's schedule unless the price of the vaccine given to parents is significantly reduced. For the cocooning strategy to become cost-effective in comparison with today's schedule, the price of the vaccine given to caretakers must be reduced with more than 70%. The corresponding figure for the maternal strategy is 10%. If the county councils are able to negotiate the price at procurement, the maternal strategy is likely to be cost-effective. A reduction of 70% is not as likely, indicating that the cocooning strategy is not expected to be cost-effective. In addition, cocooning was dominated by maternal since it gained fewer QALY at a higher cost. In comparison with on-schedule vaccination, maternal had an ICER of about 30,000 euro, which would be considered cost-effective in a Swedish setting.
The effect that maternal vaccination may have on the antibodies of the infants was yet to be evaluated when the analyses in our study were performed [21,44,45]. However, recent studies have shown that there appear to be no negative impact maternal antibodies on the vaccine effectiveness of infants' vaccination [46,47], why this should not be an obstacle for the maternal vaccination strategy to be implemented in a NIP.
If the high incidence of 2014 (108 per 100,000 infants) was not an exception, but instead the beginning of a situation with more cases, the strategies may become cost-effective. With a willingness-to-pay of 50,000 euro, the annual incidence would need to be 275 or higher for the cocooning strategy to be cost-effective, and 110 for the maternal strategy to be cost-effective, in comparison with today's schedule.
Since pertussis in infants lead to a disease severe enough to be detected and reported, we believe that the number of unreported cases is negligible [48]. Therefore, our analysis is based on the most reliable data available. Data showed that on-schedule vaccination lead to a milder disease, with a lower hospitalization rate of 38%. Corresponding data were not available for the cocooning and maternal strategy, why hospitalization reduction was not included in these analyses. It is however reasonable to assume a similar effect.
We also performed an analysis of vaccinating infants earlier; at 2, 4 and 11 months of age instead of 3, 5 and 12 months of age, since most of the infants with pertussis are infected before 3 months. Reliable data was not available for this analysis and therefore only a very simple analysis was conducted. The results indicated that such a strategy may be cost-effective since it lowers the number of infected infants with 25% and is potentially easy to implement.
The study did not include costs and QALY losses due to adverse events of vaccination. The adverse events associated with pertussis vaccination are generally mild and therefore no significant costs and QALY could be expected. However, the inclusion of such might have slightly increased the ICER of the different vaccination strategies.
A limitation of the study was that it only included the benefits of reduced incidence in pertussis among infants, i.e. children younger than 1 year. Additional benefits is expected if we would have included the effect on older children and adults. However, since the vaccination programme for pertussis aims at reducing the incidence among infants, it is reasonable to only investigate this effect. In addition, since the infection is not as severe among older children and adults as among infants, there are reasons to suspect underreporting which in turn would increase the uncertainty of the results.
The study applies a short time-horizon of one year. The most important reason for this, was that the most severe cases of pertussis occur during a newborns first year, and since the modelled population was one birth cohort the time-horizon covered this. It is hard to estimate the effect of a longer time-horizon, since the model did not account for herd-immunity of the effect of pertussis vaccination on older children and adults. Further research should be directed to the effect of herd-immunity within a dynamic modelling context, to facilitate more precise estimates of cost-effectiveness.
This study estimates that on-schedule vaccination would be cost-effective whereas cocooning and maternal vaccination would not be cost-effective in a Swedish setting. The results were mainly affected by the price of the vaccine, and the incidence of pertussis among infants. The primary objective with the pertussis vaccination programme is to protect the infants from infection.