We computed data from the records of the patients hospitalized in the Infectious diseases ward of University Hospital of Point G, from January First, 2005 to December 30, 2014.
Two thousand five hundred forty-six (2,546) patients were hospitalized in an increasingly growing manner. These patients were predominantly male (sex ratio = 1.12), young age (average = 37.03 ± 12.6 years) and leaving in Bamako and its surroundings. These admissions are most often (60.2%) on medical reference, but a significant proportion comes directly to hospital.
The human immunodeficiency virus (HIV) infection is the most prevalent disease with 74%, therefore influencing the profiles of other pathologies, such as: the importance of opportunistic infections (31.7%) and co-infections (Tuberculosis: 17.2%; Hepatitis B: 1.2%). Nevertheless, there are coexisting noninfectious diseases among patients hospitalized in the ward (1.5%). Among HIV patients: there is a relative feminization with a sex ratio equal to 0.96; a young age (average = 38.1 ± 10.6 years old); a longer hospital stay (average = 18.9 ± 23.8 days in HIV positive vs. 12.4 ± 14.1 days in HIV negative) and higher hospital mortality (46.6% in HIV positive vs 32.8% among HIV negative). In all patient admitted, Forty-one percent of deaths occurred during the first week of hospitalization.
This study gives an overview of infectious diseases seen in African teaching hospital and outlines the importance of HIV this ward over the past decade. That helps to have an idea of the trend of hospitalization and to plan resources for the coming years.
HIV, Pathology, Infectious diseases, Profile, Bamako, Mali
Infectious diseases remain major public health issues with their corollary of epidemic and endemic disease, principally in developing countries. In 2010, the number of infections diseases related deaths was estimated to 15 millions per year worldwide and the World Health Organization (WHO) fore-casts this number to 13 million in 2050 [1]. These various infectious diseases, from the most frequent like malaria to the less like neglected tropical diseases are a scourge for developing countries [2] and are major cause of hospitalization in Africa [3]. Among these diseases, HIV infection, appeared in the 80, is characterized by a decreased immunity favoring the occurrence of other so-called opportunistic infections and tumors. The emergence of HIV helps resurgence and re-emergence of numerous infectious agents. According to the 2013 UNAIDS report [4], the evolution of the HIV/AIDS in the world has firmly taken a new face in recent years. With the discovery of antiretroviral drugs, HIV infection has changed prognosis from a rapidly fatal disease to a chronic disease. Worldwide, the number of people living with HIV (PLHIV) in 2013 is estimated at 35 million, of which 24.7 million live in sub-Saharan Africa. An overall decrease of new infections is noted. Thus in 2013 in the world there were 2.1 million people newly infected against 3.4 million in 2001, a decrease of 38%. This decline is also noted in sub-Saharan Africa or the number of new HIV infections declined by 33% between 2005 and 2013. But sub-Saharan Africa still accounts for almost 70% of new HIV infections in the world.
In addition to the importance of new infections in sub-Saharan Africa, the number of deaths linked to HIV remains high, and 1.1 million people died of AIDS-related causes in 2013. However, there is a relative decline in these deaths AIDS of about 39% between 2005 and 2013. All these data affect the profile of patients hospitalized in various departments in these countries in pediatrics [5] as in adult medicine [6]. In Mali, HIV prevalence in people aged 15-49 in the general population was 1.1% in 2013 [7]. The proportion of PLWHA among patients hospitalized in Infectious Diseases Service has not been studied but a study conducted from 2007 to 2008 in an infectious disease in Senegal, a country bordering Mali with as an epidemiological profile of concentrated type for HIV in the general population showed that 27% of patients hospitalized in the service were HIV positive [8]. Another study conducted in 17 health centers located in Togo recruited 7361 hospitalized patients, 1764 were tested, of which 714 patients (40.5%) were seropositive for HIV [9].
These data shown change can occur in the configuration of hospitalized patients' trough years [10-12]. Although studies are conducted on various infectious diseases including HIV in hospital setting in many countries including Mali [8-13], no study shows the dynamics of the influence of HIV infection on the hospitalization of patients in Infectious Diseases ward. Thus, we wanted to study the pathologies encountered in hospitalization in an infectious diseases to HIV in Mali at the era of HIV in order to determine the frequency of different pathologies encountered, to describe the sociodemographic characteristics of patients to calculate main hospital indicators and to determine the specific mortality rate for all pathologies.
The study was conducted in the ward of Infectious and Tropical Diseases at Point G teaching Hospital located in District III of Bamako. This ward is the only benchmark for management of all infectious diseases in Mali it is also a center of excellence for the treatment of patients infected with HIV. So, the staff brings expertise in clinical research for the prevention and management of all infectious diseases. The inpatient capacity is 36 beds; there are daily bedside visits but also general visit twice a week. Inpatient admissions are made from outpatient consultation or transfers from the emergency department.
The design of the study retrospectively captured and analyzed all records of the inpatients from 2005 to 2014.The sampling was exhaustive, taking into account all the patient records in the ward. All patients that have at least 48 hours of hospitalization were enrolled but those with no known diagnosis or not found record were withdrawn.
– Sociodemographic data: patient identification, age, gender, ethnicity, profession and residence;
– Dates of entry, diagnosis and release;
– Disease evolution: death; medical discharge; transfer or abandonment.
Data were entered into a database designed on the Microsoft Access 2007 software, then they were exported to SPSS 20.0 software for analysis. The relationship between variables was determined with Fisher test and the means were compared by the Mann-Whitney test with a significance threshold of p ≤ 0.05.
In total 2546 records of patients hospitalized in the ward was analyzed. The largest number of admissions was registered in 2012. The majority of patient was male (sex ratio = 1.12). Their mean age was 37.03 ± 12.6 years. Seventy two percent of them resided in Bamako and its neighborhood. The Bambara ethnic group accounted for 41.0% of cases.
The disease with the highest prevalence was HIV infection with 74.6%.
Infectious diseases were implicated in 98.5% of patients hospitalized in the service (Figure 1).
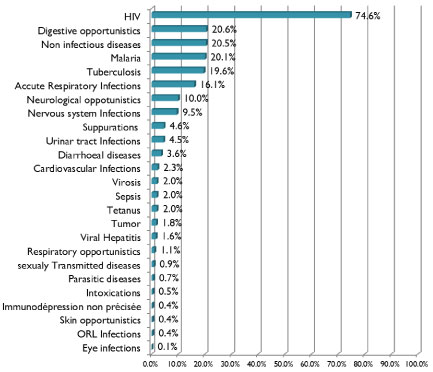 Figure 1: Prevalence of each pathology in the ward of infectious disease Point G teaching hospital from 2005 to 2014.
View Figure 1
Figure 1: Prevalence of each pathology in the ward of infectious disease Point G teaching hospital from 2005 to 2014.
View Figure 1
The most common noninfectious diseases were hematological and cardiovascular respectively with a prevalence of 5.2% and 3.8%. HIV1 was a majority 95.9% of HIV-positive patients for HIV.
The male was most represented (64.3%) in HIV-negative patients, while women were the majority in HIV-positive subjects (p < 10-3). The age group of the most affected by HIV infection was patients between 31-45 years (p < 10-3) (Table 1). Digestive coccidiosis was the majority opportunistic infection with 19.7%, followed by cerebral toxoplasmosis and digestive candidiasis, with 10.2% and 7.1% respectively. The most common co-infection with HIV was tuberculosis with 17.2%. The duration of hospitalization of patients with HIV infection was significantly higher than non-HIV infected patients. The HIV infection significantly increases the lethality of the nervous system infections, malaria, viral diseases, acute respiratory infections and cardiac infections (Table 2). Respiratory opportunistic infections had the highest lethality 57.1%.
Table 1: Relation between age, gender and HIV status of hospitalized patients. View Table 1
Table 2: Relation between lethality of infectious diseases and HIV status. View Table 2
The length of stay for patients hospitalized for infectious diseases was significantly higher than that of patients hospitalized for infectious diseases associated with another disease (Table 3). The most common output mode was medical discharge with 1332 patients (52.6%), the deaths occurred in 41% of cases during the first week of hospitalization. Mortality in patients infected with HIV was significantly higher than that of non-HIV-infected patients (p < 10-3). Mortality in patients hospitalized for a single infectious disease was significantly lower than in cases associated with another disease (p = 0.01) (Table 4).
Table 3: Relation between hospital stay duration and diseases. View Table 3
Table 4: Relation between diseases and hospital lethality. View Table 4
The most common condition in hospitalized patient in the ward of infectious disease during the study period was the HIV infection with a hospital prevalence of 74.6%. This prevalence is high compared to the general population in Mali, 1.1% according to DHS V [6]. This is due to the selective nature of our recruitment which involves persons already presenting diseases. Moreover, the ward of infectious disease is considered as the one giving the highest standard of care to people living with HIV in Mali. Lower HIV prevalence were found in hospitals setting in some other African countries such as Togo or on 1764 patients hospitalized in several centers, 714 were HIV positive, 40.5% [8]. In Senegal 27% of all admissions in the infectious diseases ward of Fann Teaching between 2007 and 2008 (527/1947 patients) were infected by HIV [8]. In Benin, Zannou, et al. found that HIV infection had a frequency of 20.2% in internal medicine [14]. These frequencies lower than our finding can be explained by the fact that studies in Benin and Togo (where HIV prevalence in the general population is higher than in Mali) [14] took place in internal medicine where many other pathologies are hospitalized including non-infectious diseases; but in study carried out in an infectious disease ward like the one in Senegal, the reason is probably the lowest HIV prevalence in the population as compared to Mali [4]. The HIV prevalence in hospital across years has no significant variation in our study (from 69.0 to 84.9%). Similarly, in another recent West African study, Ouedraogo in Burkina Faso found no significant variation from 8.7 to 22% between 1998 and 2000 [15]. But differently in Central Africa and older studies, the variation according to year was significant: Okome in Gabon found a variation from 28.8 to 49.5% between 1994 and1998 [16]; and Loemba from 9.8 to 35.9% between 1988 and 1992, in Congo [17].
HIV-1 was the most frequent with 95.9%; HIV2 and coinfection HIV1 + HIV2 were 2.5% and 1.6% respectively, this result is consistent with the finding of Oumar, et al. (95.7% of HIV-1) in the same ward [18], that corresponds to the epidemiological profile HIV in West Africa.
After HIV, digestive opportunistic infections occupied the second place with a prevalence of 20.6%. This is in fact the first clinical manifestations of infection with HIV. Digestive coccidiosis has a prevalence of 19.7% followed by the digestive candidiasis with 7.1%. Alongside these digestive opportunists, those of the nervous system were also frequent with toxoplasmosis as heading disease 10.2%. However, for most authors, it is the candidiasis who came first among digestive opportunistic [8,9,14]. It is noteworthy that in our study, the biological evidence was not available for all cases of coccidiosis. It is the same for toxoplasmosis. This can be explained by the fact that the majority of patients, firstly, received treatment before being hospitalized or came in the late stage of HIV infection. This is also the result of the limitation of the technical platform in our hospital or the lack of resources for patients hospitalized in the ward. Among the Co-infection, tuberculosis was the most frequent seen in 17.2% of HIV infected patients. This frequency is lower as compared to the one found by Oumar, et al. earlier in the same ward (26.1%). We must remember that our study covered a longer period from 2005 to 2014 and that in recent years the treatment of HIV with ARVs is earlier (CD4 inclusion rate is higher) the occurrence of disadvantage opportunistic infections late stages of HIV. An Ivorian study [12] and another Senegalese [8], found higher frequencies of TB-HIV co-infection, respectively, 34.2% and 40.9%. However, in two series, one from Togo [9] and another from Benin [14] found lower frequency of co-infection of TB and HIV, respectively 11.3% and 14.8%. These studies only took in account cases of pulmonary tuberculosis.
The young age of subjects in our study can be explained by the great proportion of PLHIV among the hospitalized patients. Indeed, this distribution of age among all patients (37.1 ± 12.6 y/o) can be aligned to that of patients with HIV (38.1 ± 10.7 y/o). This average age is higher than that found by Apetse in Togo in 2008 (37 y/o, ranging from (15-78)) [9] and Ouedraogo in Burkina between 1998 and 2000 (36.7 y/o ranging from (17-73)) [15]; butit is inferior to the average age found by Kra in Ivory Coast from 2006 to 2007 (39 y/o with extremes of [18-86 y/o]) [12] and Fortes in Senegal between 2007-2008 (41 ± 10 y/o) [8]. The last two studies were as inclusion criteria age over 15 years and membership in an active file of PLWHA already followed in a support structure with ARVs while our study was exhaustive including subjects under 15 y/o (representing 2.5% of our population) and also already followed PLWHA as well as recently discovered patient.
In overall patients' majority was male (sex ratio = 1.12). Drabo in Burkina Faso between 1990 and 1993 [19] had also found a male but with a sex ratio superior to ours (1.61); his study took place in an internal medicine department. This higher sex ratio can be explained by the recruitment in internal medicine department that is more general as compared to infectious diseases ward that has more specific recruitment, in particular HIV positive patients. Men also hold financial power in Africa, and therefore, they have greater financial access to care and more frequent health services. But for HIV positive patients in our series, the majority was female (sex ratio = 0.96), similarly in Senegal, Fortes, et al. found a sex ratio of 0.90 [8], and Apetse in Togo 0.59 [9]. But Ouedraogo in Burkina Faso from 1988 to 2000 had found a male predominance (sex ratio = 1.2) in PHAs hospitalized in the pulmonology department [15]. This can be explained by the influence in the latter study lung opportunists who were the reason for hospitalization of these PHAs in the pulmonology department.
In our study the average length of hospitalization of PLWHA in the ward was 18.9 days, this is greater than the one of patients tested negative for HIV (12.4 days). HIV patients generally have a number of co-morbidity and come at the advanced stage of diseases; they need more time to recover. Our result is consistent with the study of Fortes, et al. [8] who found a mean hospital stay of 16 ± 14 days for patients infected with HIV in Dakar between 2007 and 2008. The length of stay for patients hospitalized for infectious diseases was higher than that of patients hospitalized for infectious diseases associated with a non-infectious pathology with respectively 17.3 and 12.5 days. Patients that have other non-infectious pathology are often quickly referred to other ward as needed by their pathology.
In our series, the overall hospital mortality was 43.1%. Stratified analysis of mortality showed significant differences. Hospital mortality in patients with HIV infection was significantly higher than in non-HIV infected 46.6% and 32.8% respectively patients. The mortality in patients with infectious diseases only was significantly lower than that of patients hospitalized for infectious diseases associated with other pathologies, with 43.1% and 46.2% respectively. In their study internal medicine Drabo, et al. in Ouagadougou [19] and Zannou, et al. in Cotonou [14], have found lower mortality than us, respectively 25.2% and 21%. These studies were recruiting a wide range of diseases with a specific mortality lower than we found in our study. Moreover, in the two studies the mortality in PLWHA was lower than ours; 23.4% and 11.6% in Zannou in Drabo. But in Strong, et al. study selectively conducted in PLHIV populations have higher mortality rates than ours (44% hospital mortality) [8]. Regarding the delay from the disease onset to death, 41% of our patients died during the first week of hospitalization. A higher proportion of patients (60%) died during the same period in the study of Zannou conducted in Benin from 2002 to 2003 in the ward of internal medicine [14]. In Burkina Faso, between 1990 and 1993, Drabo in internal medicine ward found a mortality rate close to ours (46.2%) but for a longer period (10 days in hospital) [19]. The variation of these delays could be explained by the nature of the condition, the condition of patients on admission, timeliness and appropriateness of care.
The analysis of lethality by pathology shows that infections like sepsis (66.7%), viral hepatitis (58.5%) and tuberculosis (50.3%) were the most lethal in our series. Sepsis also was found with a high mortality in the series of Lewden [20]. For tuberculosis, lethalities we have found in the literature are lower than ours, it is 24.8% in the study of Zannou [14], 22.2% in the study of Apetse [9], 21% in the study of Ouedraogo [15] and 16.3% in the study of Kra [12]. This difference could be due to the varied nature of recruitment: Our study included both HIV positive patients and HIV-negative patients and found that HIV infection increases the lethality of certain infectious diseases such as those of nervous system, sepsis, hepatitis, viral diseases, malaria, urinary infection, abscesses. In contrary, it does not affect the lethality of diseases such as diarrheal diseases, and tuberculosis. Several authors have made similar findings [20-22]. Opportunistic infections of HIV, that represents the second group of the most prevalent disease in our serie, they have various fatality rates: thus respiratory opportunistic infections had the highest fatality rate with 57.1% followed neurological opportunistic infections 48.8%. In his study, Fortes had found us as the strongest lethality to respiratory opportunistic infections with 36% for tuberculosis and 18% for pneumonia; neurological opportunistic infections came in second with 12% for encephalitis and 8% for the neuromeningeal cryptococcosis. In contrary, Kra had found neurological opportunistic infections to be more frequent (51.9%), followed by respiratory opportunistic infections 22.9% [12].
HIV infection is the most prevalent disease affecting the profile of other conditions, in the ward of infectious diseases. Thus, opportunistic infections and co-infections are important in the ward. The coexistence of non-infectious diseases is also seen as well as a relative feminization of admissions, the young age of the patients, an extension of the length of stay and high hospital mortality.