A 21-year-old female presented with non-specific symptoms of cough and sore throat. She rapidly became profoundly unwell, requiring intubation and ventilation. Clinical and radiological appearances were felt to be in keeping with Lemierre's Syndrome (LS). The diagnosis of LS was confirmed when pleural fluid samples were found to contain Prevotella veroralis and Fusobacterium necrophorum. Due to worsening respiratory function the patient was commenced on veno-venous extracorporeal membrane oxygenation (VV-ECMO). She subsequently underwent three thoracic surgical procedures, undertaken via video-assisted thoracoscopic surgery (VATS). She began to improve and was successfully discharged from hospital after twenty-nine days. Repeat imaging six weeks later demonstrated complete resolution of the pathology. As the incidence of LS continues to rise in the modern era, so must clinician awareness of this uncommon and frequently life-threatening condition. Timely and accurate establishment of diagnosis remains a major challenge in treating a condition where prompt management with antibiotic therapy is vital for survival. In patients with associated respiratory and/or haemodynamic compromise, the utilisation of ECMO can help to salvage an otherwise seemingly futile situation. However, whilst the benefits of extracorporeal support are clear, ECMO also poses its own unique set of challenges and hence its employment must be considered on an individual case-by-case basis. This case, which is the first English-language case report of utilisation of VV-ECMO for management of LS, highlights that when used appropriately, ECMO can be instrumental in ensuring patients with profound, life-threatening sepsis and associated multi-organ failure are successfully managed, leading to total resolution of infection and complete patient recovery.
Lemierre's syndrome, Thoracic surgery, Microbiology, Video assisted thoracoscopic surgery, Mechanical circulatory support, ECMO, VV-ECMO
LS: Lemierre's syndrome; VV-ECMO: Veno-Venous Extra-Corporeal Membrane Oxygenation; VATS: Video Assisted Thoracoscopic Surgery; VA-ECMO: Veno-Arterial Extra-Corporeal Membrane Oxygenation; ED: Emergency Department; CT: Computed Tomography; BiPAP: Bilevel Positive Airway Pressure; MRSA: Methicillin Resistant Staphylococcus Aureus; ARDS: Acute Respiratory Distress Syndrome
The case is presented of a 21-year-old female who initially presented with a sore throat and productive cough. She had previously been seen by a doctor in a primary care setting who diagnosed tonsillitis and commenced her on oral antibiotics. She had a background of recurrent chest and ear infections over the last few months, but no co-morbidities. She deteriorated significantly over the next twenty-four hours and was taken to her local Emergency Department (ED) by ambulance. Her presenting symptoms were vomiting, shortness of breath, and a cough productive of green sputum. On admission was found to be pyrexial, hypotensive, tachycardic and hypoxic. She was drowsy and had mottled extremities. A chest radiograph performed in the ED demonstrated left sided consolidation and right sided hydropneumothorax (Figure 1).
 Figure 1: Chest radiograph on initial presentation to the local emergency department.
View Figure 1
Figure 1: Chest radiograph on initial presentation to the local emergency department.
View Figure 1
She was intubated and ventilated in the ED and a right sided chest drain was inserted which drained approximately 600 ml of frank pus and also partially re-inflated the lung. She was transferred to the intensive care unit where she was commenced on inotropes and broad-spectrum antibiotics. She also underwent blood transfusion. A computed tomography (CT) scan was performed which demonstrated bilateral cavitating lung nodules and the presence of a large left sided effusion. A left sided chest drain was therefore also inserted, which drained an additional 500 ml of pus. A repeat chest radiograph demonstrated further improvement (Figure 2).
 Figure 2: Chest radiograph after insertion of a right-sided chest drain.
View Figure 2
Figure 2: Chest radiograph after insertion of a right-sided chest drain.
View Figure 2
After 72 hours she was extubated. A repeat CT scan revealed persistent bilateral pleural pathology despite the presence of three chest drains. Due to ongoing hypoxia and the recognition that surgical intervention would likely be required, she was subsequently transferred to our unit (a regional tertiary thoracic surgery centre) for further management.
Due to disease progression, the decision was taken to proceed to surgical treatment of the empyema. At induction of anaesthesia, the anaesthetist struggled to intubate and ventilate the patient. Due to her ongoing respiratory compromise, the decision was made by a team of consultant thoracic surgeons and consultant cardiothoracic anaesthetists to commence her on veno-venous extra-corporeal membrane oxygenation (VV-ECMO) and proceed with surgery as initially planned. During this first procedure a significant haemorrhagic collection (in excess of two litres) was drained from the left side.
A further CT scan was performed which demonstrated a right submandibular & hypopharyngeal fluid collection with peritonsillar inflammation in the presence of right subclavian and jugular vein thrombosis. It was felt that these features were indicative of Lemierre's Syndrome (LS). The bilateral pleural collections had progressed significantly, to the extent that virtually no aerated lung was present on either side. The diagnosis of LS was confirmed when pleural fluid samples were found to contain Prevotella veroralis and Fusobacterium necrophorum (Figure 3).
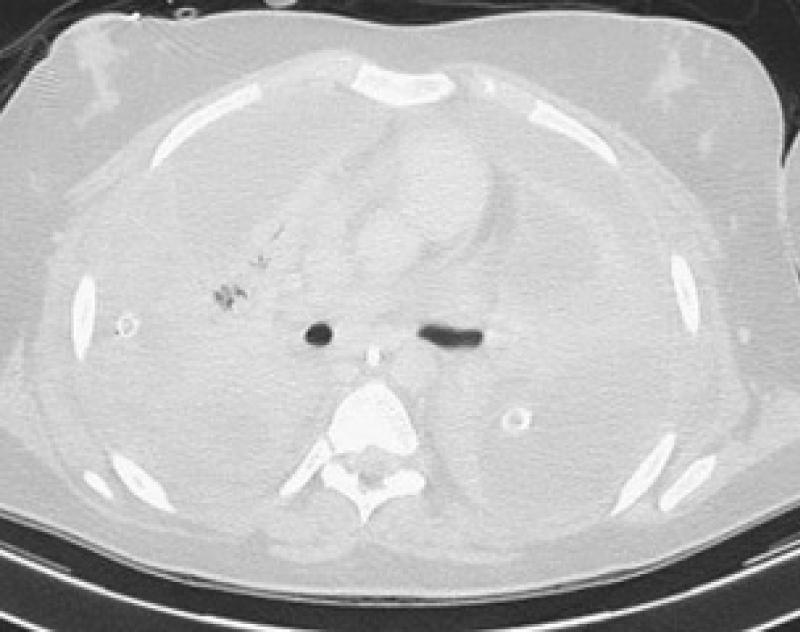 Figure 3: Computed tomography demonstrating the absence of aerated lung.
View Figure 3
Figure 3: Computed tomography demonstrating the absence of aerated lung.
View Figure 3
She remained on ECMO for the next nine days and during this time she underwent two separate thoracic procedures: A left video-assisted thoracoscopic surgery (VATS) exploration and washout, and a subsequent right VATS exploration and washout. During both of these procedures complex pleural collections were broken down and evacuated. Repeat chest radiograph demonstrated a substantial improvement in the appearance of the lung fields (Figure 4).
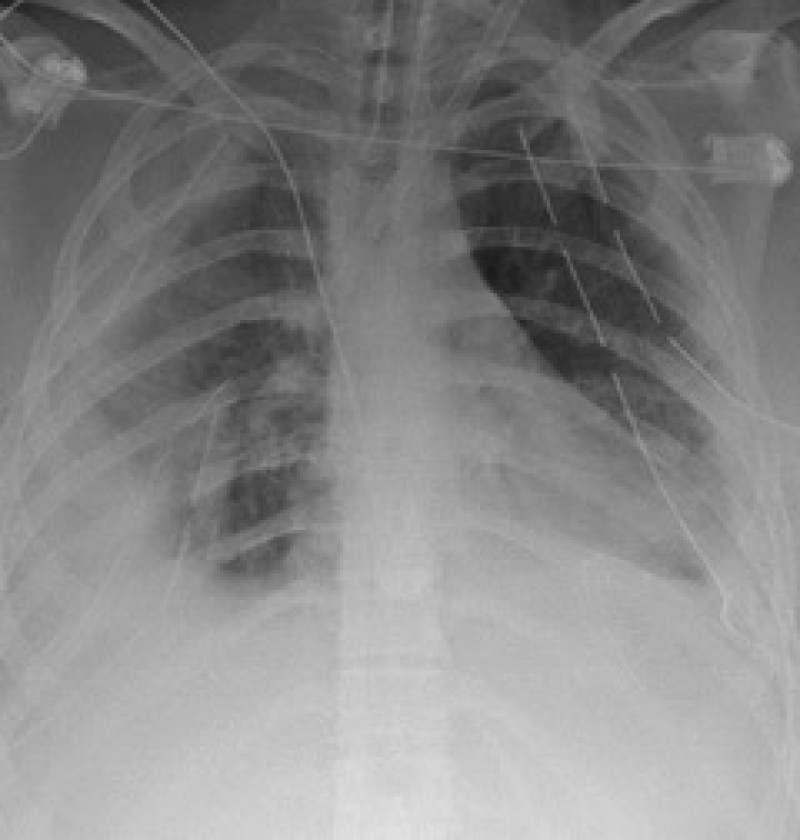 Figure 4: Chest radiograph showing a marked improvement.
View Figure 4
Figure 4: Chest radiograph showing a marked improvement.
View Figure 4
After nine days she was decannulated from ECMO and remained on bilevel positive airway pressure (BiPAP) ventilation. A further right sided VATS exploration followed a week later after a repeat CT demonstrated a non-resolving right sided loculated effusion with associated lobar collapse.
Following successful surgical intervention, a percutaneous tracheostomy was sited and a month-long respiratory wean began. Her recovery was complicated by bilateral internal jugular vein thrombosis and bilateral iliofemoral vein thrombosis. She was found to be antiphospholipid, lupus anticoagulant and anticardiolipin positive and commenced on warfarin. She was stepped down from intensive care after twenty-five days and from there was discharged home four days later. An outpatient CT six weeks later demonstrated complete resolution of the pathology (Figure 5).
 Figure 5: Computed tomography showing complete resolution of pathology six weeks after discharge.
View Figure 5
Figure 5: Computed tomography showing complete resolution of pathology six weeks after discharge.
View Figure 5
Lemierre's syndrome (LS) is an uncommon clinical condition characterised by oropharyngeal infection, infectious internal jugular vein thrombosis and systemic anaerobic septicaemia. Whilst sepsis following throat infection was initially described in a case report in 1918 by Schottmuller, it was André Lemierre in 1936 who published the first case series of patients presenting with this condition. He classified the disease “anaerobic post-anginal sepsis,” and eighteen of the twenty patients described in the case series died [1]. However, it was not until the 1980s that this condition became widely known as Lemierre's Syndrome (LS) [2].
As usage of antibiotics for treatment of oropharyngeal infections became increasingly more commonplace, the incidence of LS dropped dramatically, and increasingly became known as the ‘forgotten disease,' [3-5] as reported cases continued to dwindle. However, this dormancy period appears to be at an end, as the incidence of LS has continued to rise since the late 1990s [6-8]. Theories to explain this resurgence include a reduced contemporary usage of antibiotics for oropharyngeal infection and increasing antibiotic resistance [2,7,9].
Despite the increasing number of cases being reported, diagnosis is often delayed or missed, as LS is not a condition commonly known to clinicians. Moreover, the severity of the disease means that patients frequently present in extremis or deteriorate rapidly. The decreased level of consciousness or need for intubation associated with this dramatic presentation means that prolonged and thorough history-taking is not always practical, further reducing the possibility of an accurate diagnosis being established from the outset. Alvarez, et al. recognised this limitation and reported an average delay of five days before establishing the correct diagnosis [10]. This is similar to the scenario that we have described in our case, where the patient deteriorated rapidly following presentation. Initial treatment was for chest sepsis, with a definitive diagnosis only being established once the presence of Fusobacterium necrophorum in pleural fluid samples was highlighted.
Epidemiologically, LS has an incidence of 3.6 cases per million people per year and is recognised as being a disease that typically affects healthy young adults [8,11]. Indeed, in a case series published by Karkos, et al. over half of the patients affected were in their twenties [12]. This trend towards LS affecting young and otherwise healthy individuals perhaps explains why, despite the severity of the infection, and the difficulties encountered in establishing diagnosis, the mortality rate, which was previously much higher, has most recently been reported as being as low as 2% [8,13].
A number of different causative organisms have been associated with LS. The vast majority of cases occur secondary to infection with Fusobacterium, of which Fusobacterium necrophorum is the most common. This is an obligate anaerobic Gram-negative rod, once thought to be part of normal gut flora [13,14]. However, current consensus is that Fusobacterium colonisation is always pathogenic and warrants antimicrobial treatment [12]. Whilst the pathogenic mechanism of F. necrophorum is complex, its ability to produce several toxins including leucotoxin, endotoxin, haemolysin, haemagglutinin and adhesin are implicated as factors responsible for its virulence [15]. Other organisms frequently associated with LS include Streptococcus, Staphylococcus aureus, Methicillin resistant staphylococcus aureus (MRSA), Klebsiella and Pseudomonas [13]. Polymicrobial infection often exists in LS: Synergism between F. necrophorum and other pathogens may occur and propagate infection [15]. Our patient was colonised by F. necrophorum and Prevotella. Whilst we do not have any direct evidence of pathogen synergism, this is one plausible theory as to the cause of such profound and rapidly occurring sepsis. Prevotella (anaerobic Gram-negative rods which are important agents of periodontal bacteraemia [15]) as a single causative organism for LS has previously been described in the literature, however this is the first published incidence of concurrent Prevotella and Fusobacterium infections causing LS.
In addition to internal jugular vein thrombosis, patients can occasionally also have thrombosis of the facial vein, transverse sinus, cavernous sinus or ophthalmic vein [13,16]. Bilateral involvement of the iliofemoral veins in addition to the internal jugular vein, as described here, has not previously been described in the literature.
The severity of respiratory compromise in our patient required commencement of VV-ECMO. Utilisation of extracorporeal life support in LS, albeit rare, has previously been described in the literature [16]. Indications for ECMO in LS include haemodynamic instability secondary to septic shock and/or refractory respiratory failure (often secondary to acute respiratory distress syndrome [ARDS]). Veno-arterial (VA) ECMO is used to achieve cardiovascular stability in the event of sepsis-related haemodynamic compromise. Moreover, the use of VA-ECMO also ensures patient stability during surgery for source control, an event which can otherwise cause significant haemodynamic compromise, due to the vasoplegic effects of disturbing a large focus of infected tissue [17]. In contrast, VV-ECMO is appropriate when ongoing respiratory support is required, yet haemodynamic parameters remain relatively stable. This is the situation described in our case and is the first English-language publication of a case describing isolated VV-ECMO to treat the severe respiratory insult encountered in LS.
One of the recognised complications of ECMO is thrombosis and often difficulties arise in maintaining a fine balance between avoiding both haemorrhage and thrombosis [18,19]. The combination of ECMO and the pro-thrombotic blood profile (antiphospholipid, lupus anticoagulant and anticardiolipin positive) described in our patient could explain why such extensive thrombosis (outside of the classical thrombosis spectrum seen in LS) was seen in this patient. In view of such atypical and extensive thrombosis our patient was subsequently anticoagulated with warfarin. The role of anticoagulation in the treatment of LS is controversial, as evidence is scarce, with no high-quality trials available. Whilst some authors have advocated anticoagulation for all patients diagnosed with LS, others have advised limiting its role to those patients with more extensive thrombosis, as in our case [20].
Whilst the benefits of ECMO in management of severe LS are clear, one particular challenge requiring special attention is limiting haematogenous spread of pathogens via extracorporeal circuits. Mattke, et al. described this phenomenon especially with Staphylococcal infections as this organism is able to adhere to and persist within the circuits [21]. Nevertheless, the spread of septic emboli resulting in multi-site abscesses is already well described in many cases of LS where ECMO has not been used. However, the extent to which ECMO circuits propagate or exacerbate this phenomenon, particularly in cases where the causative organisms are non- Staphylococcal, remains unknown.
As the incidence of LS continues to rise in the modern era, so must clinician awareness of this uncommon and frequently life-threatening condition. Timely and accurate establishment of diagnosis remains a major challenge in treating a condition where prompt management with antibiotic therapy is vital for survival. Early commencement of treatment coupled with judicious surgical excision of all affected tissue offers the best chance of achieving successful outcomes.
In patients with associated respiratory and/or haemodynamic compromise, the utilisation of ECMO (both VA and VV) can help to salvage an otherwise seemingly futile situation. However, whilst the benefits of extracorporeal support are clear, ECMO also poses its own unique set of challenges and hence its employment must be considered on an individual case-by-case basis. Yet, as described in this case, when used appropriately, ECMO can be instrumental in ensuring patients with profound, life-threatening sepsis and associated multi-organ failure are successfully managed, leading to total resolution of infection and complete patient recovery.
The authors have no conflicts of interest to declare and have not received any funding for this project. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.