Intestinal parasitic infections (IPIs) remain a public health problem in rural areas of developing countries and are often associated with poor hygienic conditions, poor drinking water quality and unsanitary environmental handling of fecal materials in tropical and subtropical zones. This study was conducted with the objective to assess some epidemiological risk factors associated with prevalence and intensity of gastrointestinal parasitic infections within households in Tonga Sub-Division, West-Cameroon.
A community cross sectional study was carried out in eight quarters randomly selected. All participants from the selected quarters were invited to provide a stool sample, and interviewed about demographic and socioeconomic characteristics, sanitary situation, and hygiene behaviors. Stool samples collected were examined using simple sedimentation, Centrifugal Sugar Flotation techniques for qualitative analysis and Stoll counting technique for quantitative analysis in the Tonga Medical Health Center.
A total of 394 people participated in the study. An overall prevalence of intestinal parasitic infections (26.4%) was observed in the entire population. Five species of gastro-intestinal parasites were identified, principally soil transmitted helminths (STH) such as Ascaris lumbricoides (11.70% and 410.10 ± 193.48 EPG) which was the most common, followed by hookworm (Ancylostoma duodenale or Necator americanus) (11.20% and 784.09 ± 1148.96 EPG), Trichuris. trichiura (0.8% and 300.0 ± 0.000 EPG). The only parasitic protozoan was Entamoeba histolytica /dispar (2.3%). Multiple helminthic infections were recorded e.g. Ascaris lumbricoides + hook worm infection having the highest prevalence (3%). Prevalence was slightly higher in females than males being 27.4% and 25% respectively and the highest rate (35.4%) was among individuals aged 21-30 years and lowest (11.8%) was in individuals of age group 31-40 years. Civil servants and persons with a superior level of education harbored the highest prevalence of intestinal parasites (44.44% and 42.3%) respectively, meanwhile in individuals who practiced farming as their principal activity and those who had only a primary level of education showed prevalence of 21.1% and 24.3% respectively. Overall prevalence as related to sex, age, principal activity and level of education was not statistically significant (p > 0.05). Some risk factors such as hand washing practice before and after meal, after defecation, washing of fruits before consumption, types of latrines, careless swimming in rivers and types of domestic animals were significantly associated (p < 0.05) with (IPIs).
This study reveals that intestinal parasitic infections are prevalent within the studied area and are associated with personal hygiene and sanitation practices and thus call for immediate control and preventive measures at individual and communal levels.
Prevalence, Intensity, IPIs, Risk factors, Households, Quarter, Tonga
EPG: Egg Per Gram of Faeces; SPSS: Statistical Package for Social Science; STHs: Soil Transmitted Helminths; IPIs: Intestinal Parasitic Infections; NTDs: Neglected Tropical Diseases; GIP: Gastrointestinal Parasites; UNICEF: United Nations Children's Fund
Intestinal parasitic infections (IPIs) are known to affect the poorest and more deprived communities in low and middle income countries of tropical and subtropical regions. Even today, (IPIs) are still considered as the most prevalent infections of mankind [1]. Findings from WHO [2] revealed that more than three billion of the world's population are infected either by one or more intestinal parasites, particularly Ascaris lumbricoides, Trichuris trichiura and hookworm. About 39 million disability adjusted life years (DALYs) are attributed to these infections (IPIs) and thus, represents a substantial economic burden [3]. About a hundred species of helminths and protozoans have been reported from the human alimentary tract and of these; soil-transmitted helminthes (STH) (A. lumbricoides, hookworm and Trichuris trichiura) are among the most common. Current intestinal protozoa which infect human beings in tropical areas include amoeba, flagellates, ciliate, sporozoan and microsporidia. Through fecal-oral ingestion from unwashed food stuff, fruits or undercooked food, skin penetration, inhalation and auto-infection, intestinal parasites are swallowed and migrate to the intestine where they reproduce and cause disease. Intestinal parasites colonize the human digestive tract, their cysts, eggs or larvae are voided with human feces which in turn contaminate the soil in areas with poor sanitation practices. IPIs pose a serious threat, with common consequences shown to be associated mainly to iron deficiency anemia, intestinal obstructions, vitamin deficiency syndrome, survival, growth retardation in children, and eventually delayed intellectual development and cognition, as well as other physical and mental health problems and low educational performance [4], while also predisposing infected persons to other infectious agents [5].
Soil transmitted helminths fall among the list of eleven neglected tropical diseases (NTDs) known to exist in Cameroon [6]. Although IPIs are considered to occur predominantly in rural areas, they may also develop in every setting where residents have poor sanitation access and poor hygienic conditions. Such environmental conditions are found in most African rural areas. Like other tropical and sub-tropical developing countries, intestinal parasites are widely distributed in Cameroon [7]. In 2012, the World Health Organization and UNICEF (United Nations Children's Fund) estimated that more than 700 million people worldwide still lacked ready access to improved sources of drinking water; nearly half living in sub-Saharan Africa and that more than one third of the global population did not use an improved sanitation facility, and of these 1 billion people still practice open defecation [8]. Such a situation is likely to maintain transmission of IPI's in sub-Saharan Africa. Nsagha, et al. [9], observed that the wide spread of IPI's in Cameroon and most developing countries in Sub-Saharan Africa is partly due to the low level of environmental and personal hygiene, fecal contamination of food, drinking water, poor housing, lack of potable safe water supply, contamination of the environment with human excreta and animal waste as well as geoclimatic nature of the area [10].
Most of the available data on the burden of IPI's worldwide are mostly focused on STHs in rural areas of tropical and subtropical regions while data on intestinal protozoan infections are scarce. Information on the prevalence of intestinal parasitic infections in Cameroon is focused on STHs infections in school-based surveys [11,12]. However, an understanding of the risk factors for each population is fundamental in order to provide recent and valuable information and to generate baseline data in relation to prevention and control of IPIs among the population in the area. Knowledge on the extent of intestinal parasitic infections through a community-based survey is rare, if any, in most rural milieus of Cameroon. Yet, to the best of our knowledge, there is none on investigating risk factors associated to IPI's within households located in Tonga Sub-Division, Nde Division, and West Region. Thus, the aim of the present study is to determine the risk factors more closely associated with the prevalence and intensity of IPI's in households in Tonga Sub-Division.
A cross-sectional survey was carried out within the period of April-August 2018 to assess risks factors associated to prevalence and intensity of intestinal parasite in households in Tonga, Nde Sub-Division, and West Region of Cameroon. Situated on the Bangangte-Yaounde national route number 4, this town opens entry to the West Region of Cameroon from Yaounde by River Nde [13]. It covers a surface area of 600 km2 for a population of about 30,000 inhabitants, comprised of four main groupings (Badounga, Baloi, Babitchoua, and Fagno). The Sub-Division is located on latitude 4°58, 11 North-South and 10°41, 45 longitude East-West, and has a divers relief with an altitude inferior or equal to 1200 meters. It has an average temperature of about 25 °C, characterized by a dry season of 4 months and a rainy season of 8 months favorable for agriculture (cocoa, coffee, food producing culture, palm tree, banana and plantain), breeding (pigs, goats, sheep and poultry), that constitutes the principal activity in the area together with petty trading. The Sub-Division is characterized by the existence of many rivers, and has a tropical, Soudano-guinean temperate climate type [13].
Persons aged 1 and above from different houses, needed consent of guardians and/or parents to participate in the study. Individuals who had been treated for any IPI's for the past two weeks at the time of stool collection were excluded. All persons in households served as target population for the study. Parents (fathers, mothers, elders and children) within households who voluntarily accepted to sign the consent form after reading through and being informed some days before and who fulfilled the selection criteria answered to a number of questions related to the study.
Based on 95% confidence limits and 5% sampling error, the sample size was calculated using the single population formula proportion [14]. Since the overall prevalence rate (p) of intestinal parasites was not known for the study area, p was taken to be 50% [14]. Using a simple lottery technique to select quarters within the entire population [15], three hundred and ninety four persons from different households randomly selected were enrolled to participate in the study.
For each quarter selected, local authorities, including the Community leader, Quarter heads, families, Meeting houses ("njangi houses") were visited some days before the recruitment and presented with the project. This includes information on the objectives of the study, presentation of the authorizations obtained for the study; from relevant administrative authority and its significance. Only households, whose members voluntarily accepted to sign and return the consent forms after having understood the content, were administered questionnaires. Data on socio-demographic, environmental sanitation and hygiene practices (hand washing before and after meal, consumption of unwashed fruits, system of garbage disposal, sources of water, latrine maintenance, open land defecation, shoe wearing, swimming in rivers and presence of domestic animals) were obtained through administration of a structured questionnaire with closed-ended questions. The questionnaire was prepared in English and French, and then translated into the local language for communication convenience. Questions were answered by respondents in each household in the presence and assistance of parents for children, the head of the family and/or the spouse.
During stool collection, clean sterile, wide mouthed capped plastic containers were distributed to each study subject along with brief instructions on how to collect stool such as to avoid contamination with water, soil and urine. A unique code, together with age and sex of the study subject were labeled on the container. They were advised to fill up the disposable plastic containers about the size of the thumb (approximately 9 g) of fresh stool using disposable spoon that were given with the containers. Each morning, filled containers were collected on the spot. Few drops of 10% formalin (5 ml) were added using a syringe to each of the stool samples and then carried in a confined carton box immediately to the Tonga Medical Center on the same day of collection for parasitological examination.
Using the simple sedimentation technique [16], and centrifugal sugar stools flotation technique [17], each stool sample was examined qualitatively and quantitatively using -Stoll's numeration method [18]. To ensure accurate identification of parasite species, bench aids for the diagnosis of intestinal parasites, was our guide together with experienced well-trained laboratory workers.
For the flotation technique, approximately 2 g of each fecal sample was put into a plastic cup containing 20 ml of flotation solution (454 g of pure saturated sugar, 355 ml of water and 3 drops of formalin) and stirred thoroughly. The resulting fecal suspension was strained through a well cleaned tea-strainer into another plastic cup and then transferred in to labeled plastic tubes and centrifuged for 10 mins at 800 rpm. Tubes were removed after centrifugation and placed in to a test tube rack and overfilled to the brim with more saturated sugar solution thereby producing a slight bulging meniscus. Cover slips were then deposited at the top of the tubes and allowed to touch the undisturbed fluid surface for two minutes. The cover slip was removed by lifting it straight up and placing on to the center of a clean grease free slide labelled with the sample number in a manner as to limit formation of air bubbles [17] and examined using the 10X and 40X objective lens.
For the Stoll quantification technique, after briefly mixing the stool sample, 3 grams were weighed out and introduced in a plastic cup. The amount of 42 ml of distilled water was added to each cup and stirred using a small spoon. The mixture was filtered through a tea-strainer into another plastic cup. While stirring the strained mixture, 0.15 ml (equal to 4 to 5 drops) of the suspension were obtained with a syringe and spread over left and right sides of the slide. Cover slips were put over the slide and placed on the compound microscope. The entire slide was examined and the total number of eggs counted multiplied by a factor of 300 representing the number of eggs per gram of feces (EPG) [18].
Data were registered in Microsoft excel 2007 and analyzed with (SPSS) version 20.0. Chi square (χ2) test was used to compare prevalence, Mann Whitney and Kruscal Wallis tests were also used to compare intensity. Differences were considered significant when p was less than 0.05.
Table 1 shows the overall prevalence of infection obtained in the study area. It appears from this table that the highest prevalence was in quarter 7 (64.3%) and the lowest was quarter 1 (14.7%).
Table 1: Overall prevalence of gastrointestinal parasites by quarters. View Table 1
Three hundred and ninety-four people (230 females and 164 males) from eight quarters in the study area were randomly selected and examined for IPIs (Table 2). This Table indicates that more females (27.4%) were infected than males (25%); however this difference was not statistically significant (P > 0.05). All age groups were infected. Furthermore, the study showed that with respect to age, the highest prevalence (35.4%) was observed in individuals aged between 21 to 30 years while the lowest prevalence (11.8%) was in the age group 31 to 40 years (Table 2).
Table 2: Prevalence of intestinal parasites in relation to sex and age. View Table 2
Table 3 shows the prevalence of intestinal parasites in relation to level of education and principal activity. In relation to level of education, findings showed that individuals who had acquired a superior level of education had a higher prevalence (42.9%) than those with a primary level of education 33 (24.3%). Regarding principal activity, highest number of infections was encountered among civil servants and informal sector individuals 4 (44.44%) and 8 (36.4%), respectively but lowest in individuals who practiced agriculture as their main activity 20 (21.10%) (Table 3). No significant difference was recorded in relation to prevalence of intestinal parasites by level of education and principal activity (P > 0.05).
As shown in (Figure 1), results revealed five common types of intestinal parasites present in the study area. From this Figure, it appears that the highest numbers of infections were encountered with Ascaris lumbricoides 46 (11.70%).
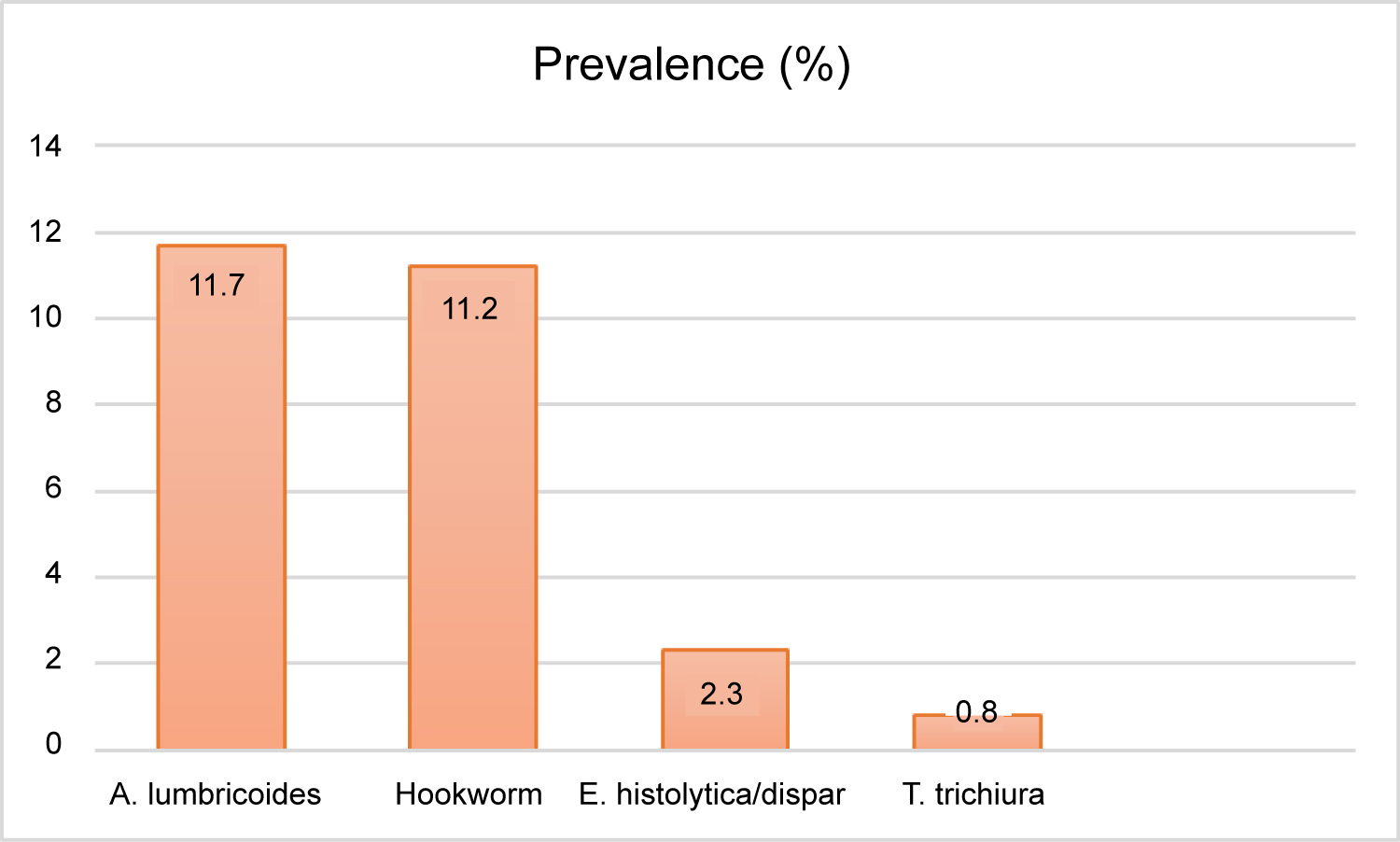 Figure 1: Common intestinal parasites affecting individuals within households.
View Figure 1
Figure 1: Common intestinal parasites affecting individuals within households.
View Figure 1
Table 3: Prevalence of infection in relation to level of education and principal activity. View Table 3
Table 4 illustrates the overall prevalence of specific intestinal nematodes according to intensity of infection. Analysis of the Table illustrates a light intensity of infection in individuals infected with hookworm 784.09 ± 1148.96, followed by infection with ascariasis 410.10 ± 193.48 Trichuris trichiura. No statistical significance was observed between the four nematodes parasites (P > 0.05).
Table 4: Prevalence of infection according to intensity of infection. View Table 4
Intensity by age groups as shown in Figure 2 revealed that individuals aged 41-50 years recorded the highest mean intensity with hookworm infection with a significant difference (P < 0.05).
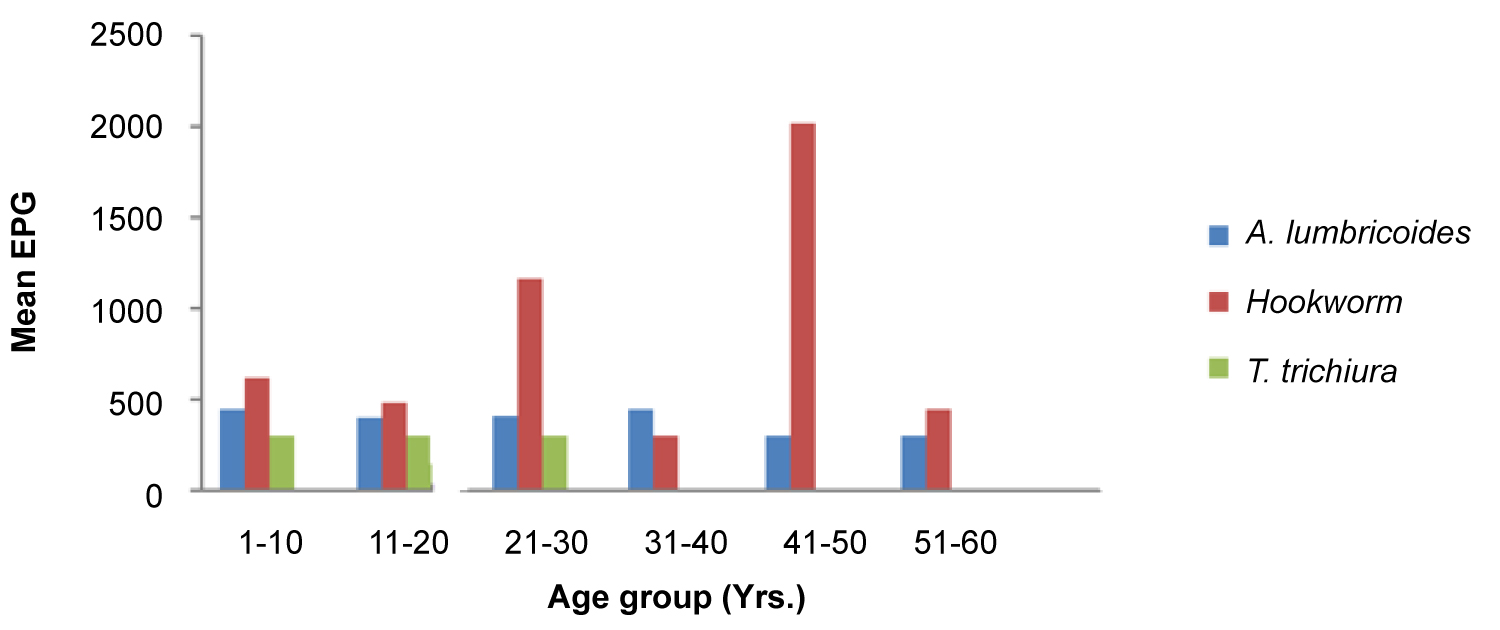 Figure 2: Mean intensity (EPG) by age groups.
View Figure 2
Figure 2: Mean intensity (EPG) by age groups.
View Figure 2
With respect to parasitic associations, 16 (4.1%) cases of polyparasitism were observed, with association between Ascaris-hookworm the most prevalent 12 (3.0%), while the least association observed between was that Ascaris-Trichuris-hookworm 1 (0.3%) (Table 5).
Table 5: Prevalence of single and polyparasitism. View Table 5
As illustrated in (Table 6), results obtained from questionnaire survey revealed that risk factors such as hand washing after defecation, hand washing before and after meal, washing of fruits before consumption, nature of latrine, indiscriminate defecation, indiscriminate swimming in rivers and types of domestic animals in homes were observed to be significantly different (p < 0.05) associated with gastrointestinal parasite infections.
Table 6: Association between risk factors and the prevalence of intestinal parasites among studied persons within households. View Table 6
All the studied quarters showed infection with intestinal parasites with varying degrees of prevalence and intensity. The prevailing intestinal parasites in all the studied quarters might be explained by the wide variation in factors like quality of drinking water supply, hygiene/sanitation practices and other environmental conditions in different quarters that predisposed the population to infection. The overall prevalence of 26.4% is similar to earlier studies from Babile town (27.2%) in Ethiopia by Girum [19], 28% in Nigeria by Gimba and Dawam. [20]. However, prevalence is higher when compared with studies from Uttarakhand in India where Kotian [21] recorded 11.6%, Kuete, et al. [22] 15.2% in Douala Urban setting. Results of the present study are lower when compared with studies of Kang, et al. [23] in Vellore, Tadesse [24] in Ethiopia, who recorded a prevalence of 97.4% and 46.2%, respectively. The difference in findings observed in this study might be due to different socio-economic conditions in the study population, individual behavioral habits of the selected study group, quality of drinking water supply, sanitation and other environmental climatic conditions in the area.
Overall prevalence of intestinal parasites by sex showed, that female individuals were slightly more infected than males at 27.4% and 25.0%, respectively. This can be better explained by the fact that in addition to household work, women in this area are also engaged in handling of livestock and farming too and thus are comparatively more exposed to contaminated soil and water, a major predisposing factor for infection. This finding is in agreement with those of Kotian, et al. [21] in India. The high prevalence rate in the age group 21-30 was an indication that individuals within this age group are more exposed since they are usually more active and frequently involved themselves fully in activities that bring them in contact with sources of infection and negligence towards basic hygiene and sanitation practices. Lower rate in the other age groups 31-40 and 71-80, can be explained by assuming perhaps their good mastery and awareness of hygiene and sanitation practices, combined with sedentary state of life style. This result was compared to studies of Kotians [21] with high prevalence among individual's aged 51-60 (22.2%) and low in age group 21-30 (6.98%). The findings were in disagreement with those of Abdalla, et al. [25] in Khartoum state.
Prevalence in relation to level of education although not significantly different, in this study showed that infection was highest (42.9%) among individuals having a superior level of education, while lowest prevalence among individuals with a primary level of education (24.3%). This is an indication that parasitic infections in general and intestinal parasites in particular are predominantly associated with poor hygiene and sanitation together with climatic factors that favor their survival and propagation. As such, everybody can be infected with intestinal parasites in the sense that everything we come in contact with, handle and or consume could be contaminated. Moreover, negligence could also be attributed to such findings, as also with those of Kidane [26] in Ethiopia.
In the present study, prevalence with respect to principal activity revealed that the rate of infection with intestinal parasites among civil servants (44%) and the informal sector (36%), were higher compared to those who practiced agriculture (21%) as principal activity, although not statistically significant. Based on environmental, socio-cultural and behavioral habits, prevalence of infection can vary within households. However, the reason for this unexpected finding is not clear but it may be the result of a relatively uniform exposure to intestinal parasitic infections across all members of the population. This result is similar to the results observed by Forrester, et al. [27] but in disagreement with those of Kuete, et al. [22]. Principal activity indeed, in urban areas, as well as economic status may be an important factor compared to the situation in rural areas where other factors such as rainfall and personal hygiene may play a major role in transmission [28]. The most plausible explanation is that it might be due to socio-cultural beliefs (most adult recruited in the study responded by saying that "dirt does not kill black man and that they are used to their poor water sources".
Multiple infections co-existed in some study subjects in the present study, concretely 4.1%, similar to that reported by Tadesse [24] (3.0%) in Ethiopia. The highest co-infection occurred between Ascaris lumbricoides and hookworm (3.0%). In this study, higher intestinal worm burdens whereas recorded among individuals aged 41-50 years with hook-worm infections. Results recorded were in agreement with reports from Bethony, et al. [29]. This was an indication that adult persons are more exposed to infection in contaminated fields and re-infection by hookworm during agricultural practices.
The unprotected nature of latrines in the study area was significantly associated to prevalence of intestinal parasites. The principal explanations to this can be that transmission may also be through mechanical vectors such as flies [30] whereby flies may carry the infective cysts/larvae from contaminated sites or dirty latrines and cause contamination of food and/or water. However, toilets which were not frequently cleaned invited the breeding of latrine flies (Fannia scalaris) which transmit intestinal infections [31].
During swimming, water contaminated with infective stages of intestinal parasites is ingested or even inhaled leading to their establishment in human body. The most common domestic animals were fowls, dogs, cats. Domestic animals often serve as companion, protection and socio-cultural wellbeing of the holders. However, their close contact with human beings might be a threat to human health. This is because animals are often implicated as natural reservoirs and intermediate hosts of many parasites involved in transmission of parasitic diseases to humans [32]. It was observed that most of the animals were not controlled and as such consumes contaminated human feces from unprotected latrines increasing chances of spreading it further in surroundings.
The present study revealed that intestinal parasitic infections are prevalent within the studied area and associated with various biological, social, behavioral and environmental factors like poverty, substandard living conditions and lack of personal hygiene and sanitation practices and thus call for immediate control and preventive measures at individual and communal levels.
Data and material are available to other researchers upon request.
The authors declared that they have no competing interest.
No funding.
The author sincerely grateful to the research unit of Biology and Applied Ecology.
KGGI, KPV, NACN and YC contributed to the design of the study, data collection, led the analysis and drafting of the manuscript. All authors read and approved the final manuscript.
The research proposal for this study was submitted to the Cameroon Bio-ethics Initiative (CAMBIN) for an ethical clearance.
Not applicable.