The second largest outbreak of Legionnaires' disease in United States history began in July, 2015 in Bronx County, NY. It was initially described as a single outbreak affecting 138 patients with 16 deaths. Subsequently, additional cases were noted in the same area and time period, officially attributed to different exposures, making the final total 155 patients and 17 deaths before ending in September, 2015. The largest portion of cases was seen at Lincoln Medical and Mental Health Center with 48 patients treated.
We reviewed the hospital and public health timeline regarding the official response to the outbreak and performed a study of all patients who presented to Lincoln Medical and Mental Health Center from July 8 to August 03, 2015 with laboratory confirmed Legionella infection. The overall mortality was evaluated as well as risk factors for disease and clinical presentation.
The standard use of Legionella urine antigen testing for community acquired pneumonia allowed for early identification of the outbreak prior to public health notification. The type of public health service investigations varied by location due to non-uniform application of Centers for Disease Control guidelines. Of the 48 patients with laboratory confirmed disease, median age was 55 years. Patients presented most commonly with tachycardia (88%), fever (79%), and cough (79%). The most common clinical findings were hyponatremia (52%), rhabdomyolysis (42%) and respiratory failure (31%). Antibiotic therapy was initiated within 6 hours for 31 of 48 (65%) patients. Two patients (4%) died during this outbreak.
Divergence from Centers for Disease Control guidelines may have limited the investigators' abilities to more accurately determine the sources for the outbreak and may have prevented this from being seen as one rolling epidemic instead of three separate events. Standard use of Legionella urine antigen testing in community acquired pneumonia by Lincoln Medical and Mental Health Center allowed for identification of the outbreak prior to the public health authorities and neighboring hospitals. Rapid diagnosis and prompt treatment led to an overall mortality of 4%.
Legionella, Legionnaires', Epidemiology, Outbreak, Pneumonia
LMMHC: Lincoln Medical and Mental Health Center; CDC: Centers for Disease Control; LD: Legionnaires' Disease; CAP: Community Acquired Pneumonia; HCAP: Health Care Associated Pneumonia; ST: Serotype; DOH: Department of Health; NYC: New York City; IDSA: Infectious Disease Society of America; COPD: Chronic Obstructive Pulmonary Disease; IQR: Interquartile Range; SD: Standard Deviation; ARDS: Acute Respiratory Distress Syndrome; SHR: Supportive Housing Residence; PFGE: Pulsed Field Gel Electrophoresis; WGS: Whole Genome Sequencing; DNA: Deoxyribonucleic Acid; HIV: Human Immunodeficiency Virus; CPK: Creatinine Phosphokinase; ICU: Intensive Care Unit; APACHE: Acute Physiology and Chronic Health Evaluation; PSI: Pneumonia Severity Index;
Legionella pneumophila is a gram-negative bacterium that causes Legionnaires' disease (LD), an aggressive pneumonia associated with significant mortality first described in 1977 after an outbreak of disease at an American Legion convention in Philadelphia [1,2]. To date, this is the largest outbreak in United States history with 221 cases and 34 deaths. Most patients have notable risk factors such as tobacco and alcohol use, chronic lung disease, or some form of immunocompromise [1]. LD occurs worldwide with the highest incidence in the summer and fall seasons, and causes both Community Acquired Pneumonia (CAP) and Health Care Associated Pneumonia (HCAP) [1]. While LD occurs in both sporadic and epidemic (outbreak) forms, outbreaks are actually unusual in the US, accounting for only 4% of cases as opposed to nearly 35% in Europe [3].
Legionnaires' disease is contracted by inhaling or aspirating water containing the bacteria. Because it is chlorine tolerant, Legionella can survive the water treatment process and pass from its natural habitat of rivers, lakes and streams into the water distribution system, creating the potential for an outbreak directly from the potable water itself or from an aerosol of that water [1]. When the potable water is the direct cause of the outbreak, infection occurs via micro-aspiration, and there is a random distribution of cases within the same municipal water distribution system. This is the case in hospital outbreaks of LD, where potable water has been shown to be the primary source of infection [4,5]. This was also the case in the LD outbreak in Flint, Michigan from 2014-2015 that infected 87 people and killed at least 12 (Figure 1). This was due in part to low levels of chlorine used to treat the drinking water from the Flint River [6].
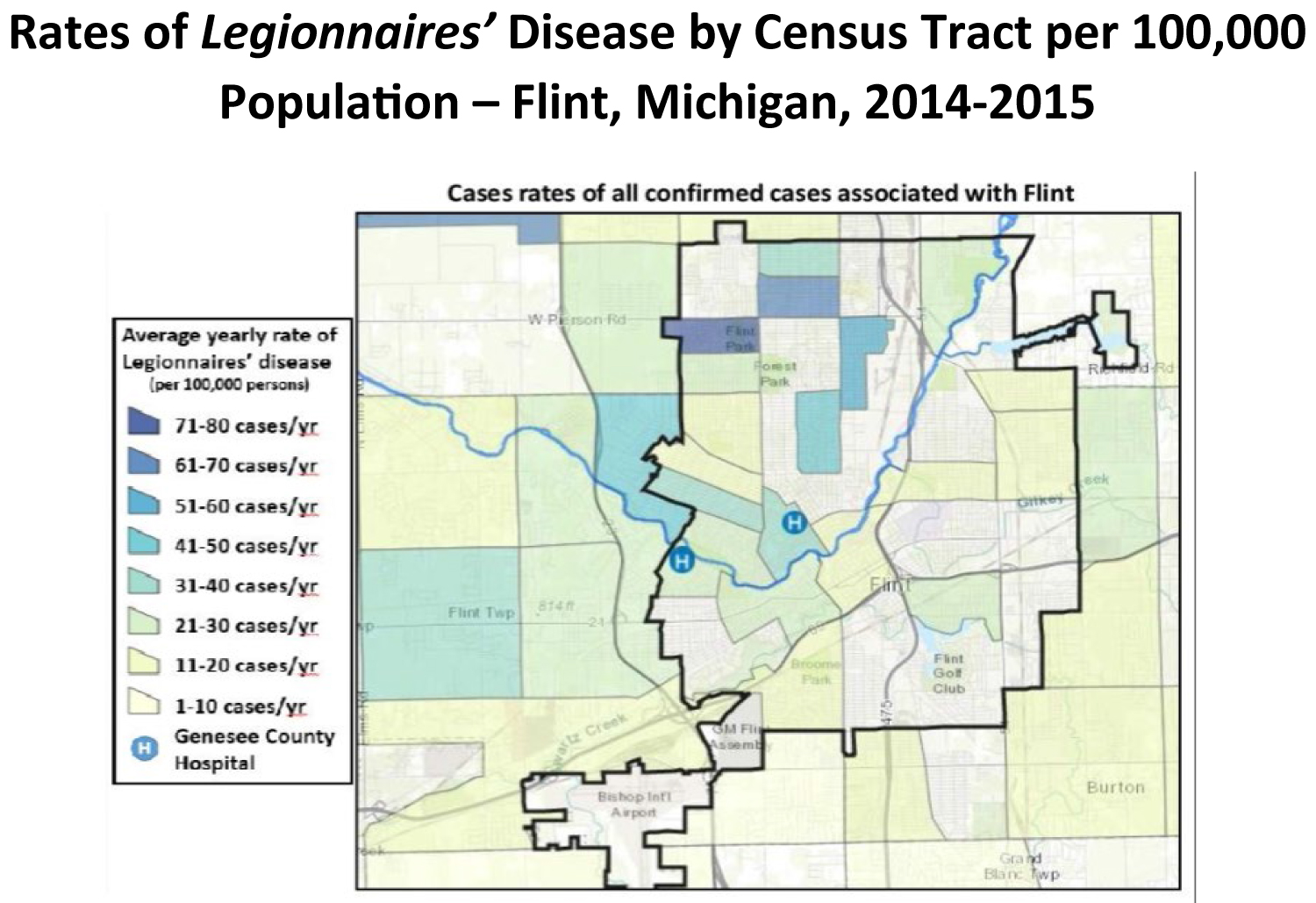 Figure 1: 2014-2015 Flint, Michigan Legionnaires' disease Outbreak Map [6].
View Figure 1
Figure 1: 2014-2015 Flint, Michigan Legionnaires' disease Outbreak Map [6].
View Figure 1
In an aerosol point-source outbreak, such as from cooling towers, fountains, spas or produce misters, there is a close relationship between proximity to the source and incidence of disease. Cases are heavily clustered around the source. This was true in the 2003 Pas-de-Calais cooling tower outbreak in France (Figure 2) [7] and also in the more recent 2019 Fletcher, NC outbreak from a hot tub display at a local fair [8]. In an outbreak investigation, epidemiologic approaches and molecular data need to be used in complement to determine the direct source of infection.
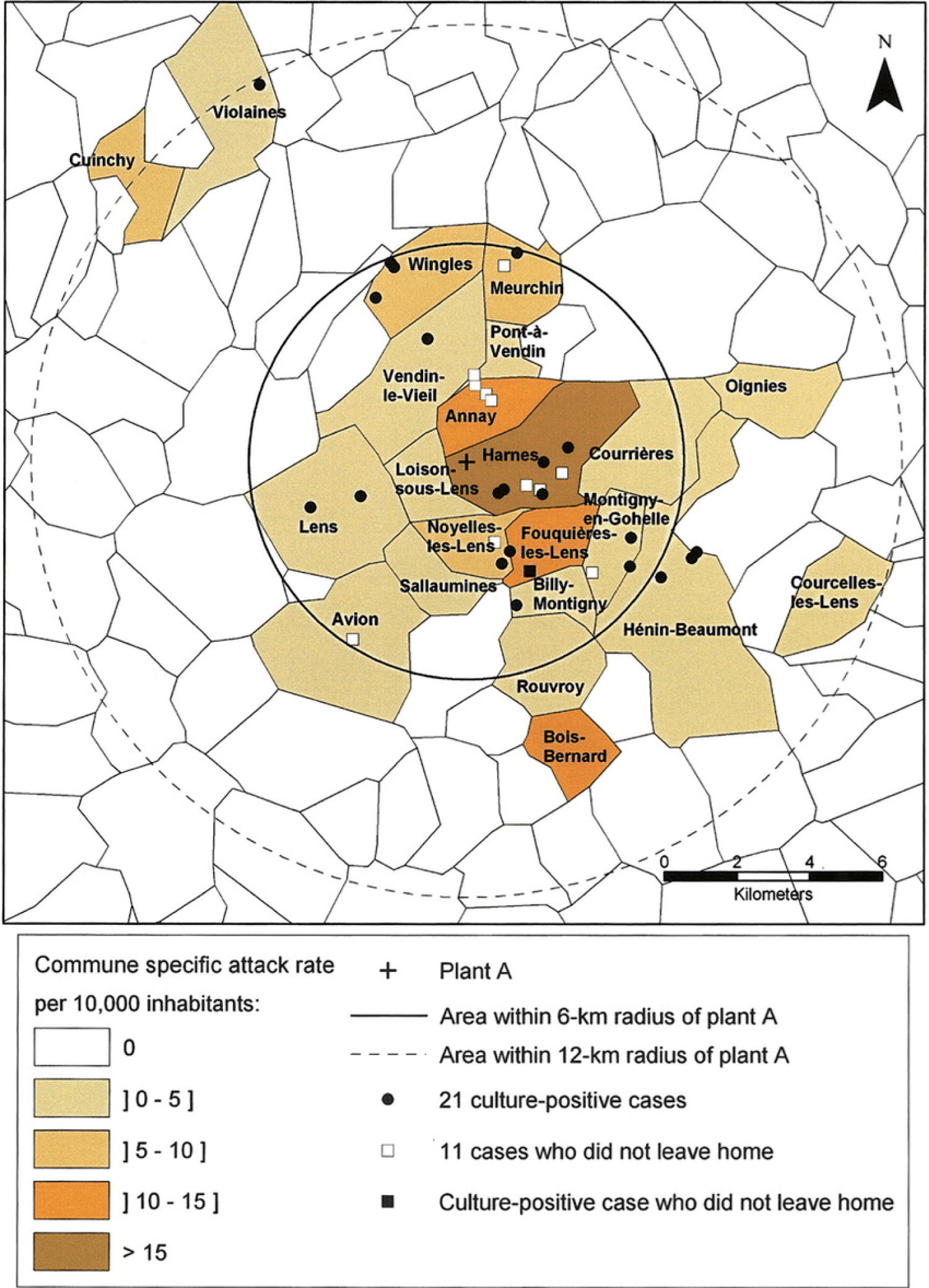 Figure 2: 2003 Pas-de-Calais, France Legionnaires' disease Outbreak Map [7].
View Figure 2
Figure 2: 2003 Pas-de-Calais, France Legionnaires' disease Outbreak Map [7].
View Figure 2
Legionnaires' disease is considered an atypical pneumonia because, historically, the organism itself was considered atypical in that it was not visualized on standard gram stain and would not grow on standard bacteriologic media [1]. Like pneumonia due to other atypical organisms, LD is associated with extra-pulmonary manifestations [9]. However, unlike disease due to Mycoplasma, or Chlamydia infections, LD has much higher mortality with rates up to 33% in early outbreaks [2,10,11]. More recent studies have documented rates consistently under 10%, [12-16] although when looking only at the most severely ill patients, these improvements are less apparent [17-19]. Multiple reviews have noted this trend and have suggested it may be related to better diagnostic and treatment algorithms [20-22]. Specifically, the Legionella urine antigen test, which has > 95% specificity for Legionella pneumophila serotype (ST) 1, allows for rapid diagnosis within 15 minutes of obtaining the urine specimen [20].
In July, 2015, the second largest outbreak of Legionnaires' disease in United States history would begin in the southern part of Bronx County, New York. By the time this rolling epidemic was complete in September, 2015, it would extend to the eastern part of the borough and total 155 cases with 17 deaths [23]. The largest portion of cases was seen at Lincoln Medical and Mental Health Center (LMMHC) with 48 patients treated. We describe the time-line and administrative response to this outbreak, discuss the possible source or sources of the epidemic and present the clinical course and outcomes for the treated patients.
We reviewed the LMMHC Infection Control records from the period of July, 2015 to August 2015 as well as the public reviewed public records relating to the formal New York City Department of Health (DOH) response during this same time period. Finally, we conducted a retrospective, observational study of all patients with confirmed Legionnaires' disease who presented to LMMHC from July 8 to August 03, 2015. Cases were defined as clinical pneumonia (fever, cough, respiratory symptoms and/or abnormal chest radiograph findings) with laboratory confirmed presence of Legionella bacteria by either the presence of urinary antigen or positive sputum culture.
Data collection forms were used to tabulate demographic data, symptoms with their date of onset, vital signs on presentation and background medical history. Laboratory test results, chest radiographs, treatment and outcomes were also recorded.
HCAP was defined according to Infectious Disease Society of America (IDSA) guidelines [24]. Lung diseases were defined as past medical history of Chronic Obstructive Pulmonary disease (COPD), asthma or fibrotic lung disease. Renal disease was defined as history of renal insufficiency or renal failure. Relative bradycardia, Acute Respiratory Distress Syndrome (ARDS), and Sepsis/Septic shock were all defined as noted [9,25,26].
After tabulation, median values with interquartile ranges (IQR) and standard deviations (SD) were calculated for all relevant data. Univariate and multivariate linear regression analyses were performed using the data analysis function in the Excel software.
South Bronx: July 16, 2015: The Infection Control nurse for LMMHC notified the DOH that the hospital admitted its fourth case of Legionnaires' disease over the prior four day period [27]. The DOH stated that they were unaware of any current outbreak and did not have enough cases to initiate an investigation.
July 17, 2015: LMMHC admitted its fifth and sixth cases of LD. The DOH was alerted after their automated monitoring system, SaTScan, detected a cluster of eight cases of LD centered in the South Bronx within a radius of 1.6 miles [28]. The DOH began performing "standard environmental and epidemiologic investigations". Environmental health and communicable disease response teams began conducting case interviews in order to identify a common exposure source. However, "the initial epidemiological findings did not suggest any common exposures. There were no common buildings visited by case patients, and case residences were spread across a 6.5 mi2 area" [29].
July 19, 2015: After LMMHC admitted its eighth case of LD, the chairperson for the Department of Infectious Diseases contacted its neighboring hospital and spoke with their Infectious Disease department about whether they had been seeing cases of LD [27]. This municipal hospital had not yet recognized the outbreak. They eventually diagnosed and treated 35 cases, the second largest cohort for any Bronx hospital [30].
July 26, 2015: The outbreak peak occurred on this date with onset of 14 cases (Figure 3). There was a rapid decline of new cases after this point in time.
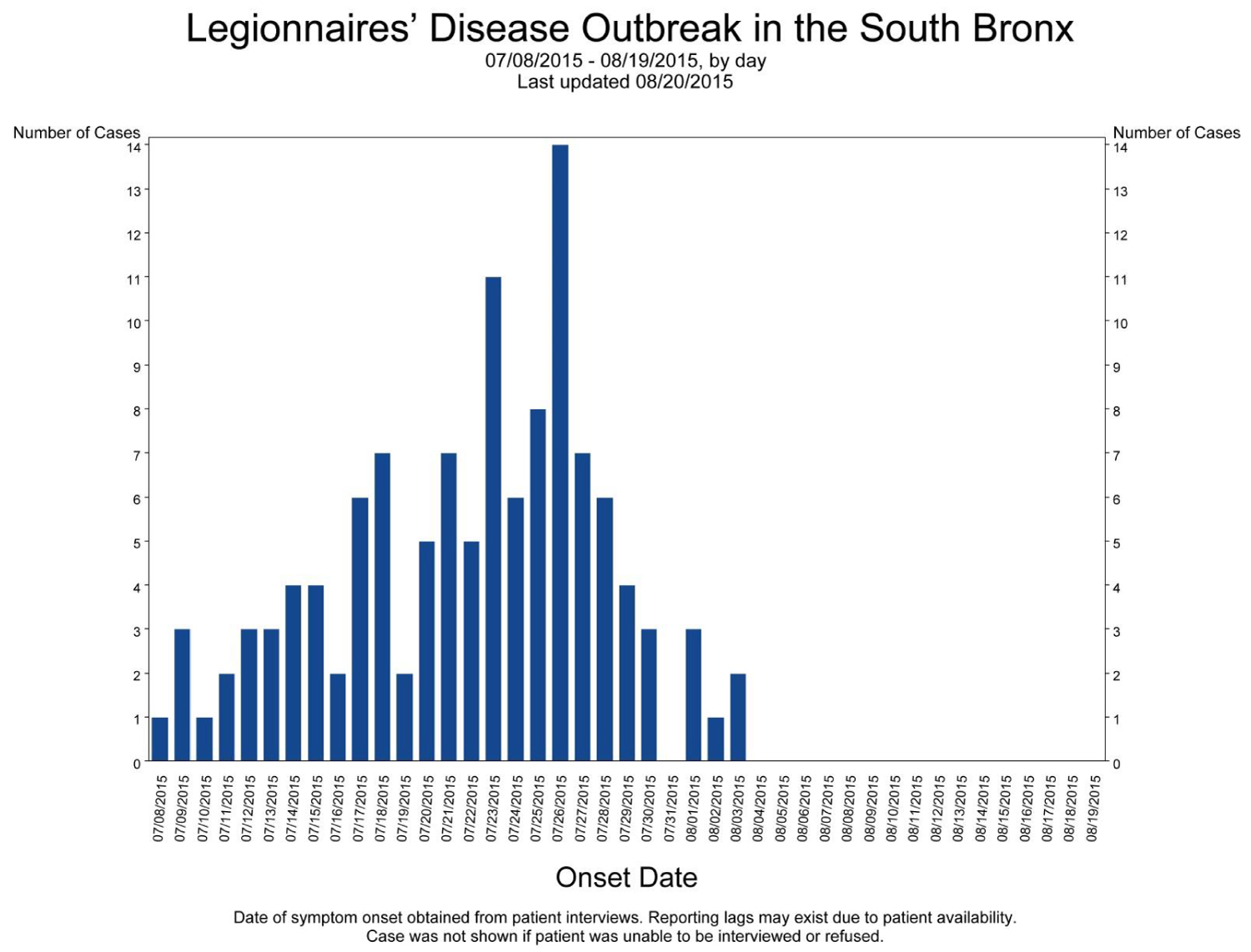 Figure 3: 2015 South Bronx Legionnaires' disease Epidemic Curve [33].
View Figure 3
Figure 3: 2015 South Bronx Legionnaires' disease Epidemic Curve [33].
View Figure 3
July 27, 2015: The DOH historical limits method, which compares case volumes from the prior four week period against historical data over the previous five years, signaled an elevated number of cases in two South Bronx neighborhoods [28].
July 28, 2015: After more than 30 cases had been reported, New York City began sampling cooling towers for Legionella [29]. The DOH stated that "we prioritized cooling tower sampling in the outbreak zone per the location of patients with Legionnaires' disease and the multi-focused cluster test" [28]. The DOH received a report from a physician who noted a cluster of respiratory illnesses among patients living in a supportive housing residence for people with medical needs (SHR) in the outbreak zone [28]. Three cases of LD were identified in this single building.
July 29, 2015: The DOH was contacted by the Centers for Disease Control (CDC) regarding a traveler diagnosed with LD shortly after a stay in a Bronx hotel (The Opera House Hotel) located one block from the SHR [28]. A second case in the hotel was also identified. The cooling tower on top of the hotel was sampled on this date. The DOH issued a citywide health alert to assist in case finding and encourage patients to seek care [30].
July 30, 2015: Of the 55 cooling towers tested in the outbreak zone, 21 were positive for Legionella ST 1. Isolates from two of these buildings, the Opera House hotel and a homeless shelter, matched the particular strain type (Pulse Field Gel Electrophoresis pattern O-1) from those patients who were both considered as part of the outbreak and had sputum culture results available for analysis [28]. The Opera House Hotel was a more likely source based on the Cluster analysis performed by the DOH. Further molecular analysis of the isolates with whole genome sequencing showed the patient isolates matched those from the hotel but not the shelter [31]. The hotel began disinfection of the cooling tower [29].
July 31, 2015: After the 46th total case was reported, the DOH issued a Fact sheet: "the New York City water supply does not pose a risk, and this investigation does not suggest that the source is a building's plumbing system. Legionella is spread through inhaling mist" [32].
August 01, 2015: Disinfection of the Opera House Hotel cooling tower was completed [33].
August 03, 2015: LMMHC admitted its final LD patient in this outbreak. As per the DOH, this was the last date of symptom onset for any outbreak patient [28].
August 06, 2015: A city-wide order was issued that mandated all cooling towers be disinfected within 14 days [29].
August 20, 2015: The NYCDOH declared the South Bronx Legionnaire's disease outbreak officially ended. There were a total of 138 cases and 16 deaths, making it the 2nd largest outbreak in United States history [34].
Melrose houses: September 02, 2015: The NYCDOH issued a press release identifying a new outbreak of four cases of Legionnaires' disease in the Melrose Houses [35]. This group of buildings is 0.4 km from the Opera House hotel. The first case occurred in March, 2015 and was not investigated. The next two cases occurred in July, 2015 and were originally included in the South Bronx outbreak. The final case occurred at the end of August, 2015. The DOH investigated and identified the potable water as the source for these cases. Legionella was found in the water distribution system in 4 of 9 buildings in this complex. A copper-silver ionization system was installed in the buildings potable water piping [33]. When asked why the potable water was considered a possible source, the DOH formally stated "we are looking at the water system because we have two cases in one building" [36]. No further information was provided regarding the clinical or environmental isolates.
Morris park: September 28, 2015: The NYCDOH issued a press release that identified an outbreak of Legionnaires' disease in the East Bronx neighborhood of Morris Park, four miles from the Opera House hotel [37]. 13 cases were identified from 9/14/15 to 9/31/15 with one death. The cooling towers in the vicinity were sampled as possible sources. 15 of 35 cooling towers tested positive despite the mandatory disinfection that was completed 1 month earlier. The DOH matched a strain from the Bronx Veterans Administration Psychiatric Center cooling tower by "DNA fingerprinting" with samples taken from 4 patients. WGS done on the patient and environmental isolates "suggest that the East Bronx and South Bronx strains only recently diverged after horizontal gene transfer events" [31]. According to the DOH press statement, the "NYC drinking water supply was unaffected".
48 patients confirmed to have Legionnaires' disease were treated at LMMHC during this outbreak (Table 1). All cases were noted as CAP. The median age of the confirmed cases was 55 years (range 35-76) and 27 (56%) were male. The population was primarily Hispanic (50%) and African American (48%). Overall, there were two deaths (4%) during this outbreak.
Table 1: Characteristics, Symptoms, Vital Signs, and Time Course of Clinical Disease of 48 patients with confirmed Legionnaire's disease. View Table 1
Urine for Legionella antigen was tested in 47 patients with 45 (95%) positive results. The two patients with negative tests had sputum cultures that grew Legionella. The remaining patient, who could not produce urine due to pre-existing renal failure, also had a positive sputum culture. In total, 24 patients had sputum samples sent with 13 (54%) positive results.
The most common underlying medical problem for these patients was lung disease. 36 of the 48 patients (75%) had COPD. Human Immunodeficiency Virus (HIV) was found in 25% of the patients. Of those with HIV, all were noted to be receiving antiretroviral therapy prior to admission. There were few patients with other classically associated medical problems such as renal disease (8%), malignancy (2%) or organ transplant (2%). The majority of patients (58%) were active tobacco users and 33% were actively using alcohol.
The most common symptoms at presentation were fever and cough. Both were present in 38 out of the 48 patients (79%). Respiratory failure requiring invasive mechanical ventilation occurred in 18 patients (38%). Altered mental status, defined as lethargy, stupor or coma, was present in 15 patients (31%) on admission. Relative bradycardia was found in 8 of the 27 patients with admission temperatures higher than 38.8 ℃. The median time from symptom onset to presentation was four days (interquartile range 3 to 7).
The most common radiologic or laboratory finding was lobar infiltrate present in 47 of 48 (98%) patients. The single patient with a normal chest radiograph presented with fever (39.0 ℃), productive cough and chest pain with a positive urinary antigen for Legionella. In those patients selected for follow-up imaging, progressive worsening was noted in the majority of cases, even after five days of treatment.
Hyponatremia (Na < 130 mEq/L) was found in 14 of 48 (29%) patients (Table 2). In addition to four patients with renal failure at baseline, 11 patients presented with evidence of acute renal insufficiency (Cr > 2.0 mg/dl). Renal impairment resolved in 10 of these 11 patients. The single patient with persisting new onset renal failure expired. Rhabdomyolysis (Creatinine Phosphokinase (CPK) > 1000 U/L) was present in 12 of 39 subjects who were tested on admission (31%). We found evidence of chemical pancreatitis (Lipase > 480 U/L) in 11 0f 29 patients who were tested, with abnormal levels ranging from 517 U/L to 37,250 U/L.
Table 2: Laboratory, Radiologic, and Severity Data on Admission for 48 Patients with Legionnaire's Disease. View Table 2
Pneumonia severity index (PSI) [38] was determined for all patients. 17 of the 48 patients (36%) were in category 4 or 5. APACHE (Acute Physiology and Chronic Health Evaluation) II [39] scores were calculated for those patients admitted to the ICU. Of the 19 patients, 11 (58%) had scores > 15.
The majority of patients received treatment within six hours of arrival to the hospital (Table 3). Antibiotics were given in the emergency room in 31 of 48 (65%) patients. The longest time to first dose of antibiotics was 26 hours in a patient that was initially suspected to have alcohol withdrawal. 40 of 48 (83%) patients received combination therapy with Levofloxacin and Azithromycin.
Table 3: Outcomes and Therapies Received by 48 Patients Hospitalized for Legionnaire's Disease. View Table 3
Both patients who died were in respiratory failure and suffered cardiac arrest on hospital day four. The first patient had HIV, COPD, diabetes, and chronic kidney disease, while the second patient was diabetic with newly diagnosed lung cancer on this admission. Both patients were treated with combination antibiotic therapy within six hours of arrival to the emergency room. The mean duration of symptom onset to death was eight days.
Given the low mortality noted, we evaluated risk factors for increased length of stay in this patient group (Table 4). In univariate analysis, active alcohol use, respiratory failure, altered mental status and hyponatremia were significantly associated with increasing length of stay. However, on multivariate analysis, only the need for mechanical ventilation and altered mental status were significantly associated with the outcome measure.
Table 4: Multivariate Analysis of Factors Associated with Increased Length of Stay. View Table 4
The 2015 Legionnaires' disease outbreak in Bronx County, NY was considered to be a group of three distinct outbreaks in space and time, attributed to different sources, termed a rolling epidemic [23]. The source for the largest portion of the epidemic, the South Bronx outbreak, was officially identified as a hotel cooling tower.
This was unusual, because in the US, cooling tower sources accounted for only 7% of all outbreaks from 2000-2012, while in NYC, 16% of outbreaks were related to cooling towers from 2003 to 2012 [23,40,41].
The South Bronx Epidemic curve (Figure 3) shows the typical rise and fall of cases consistent with a common source outbreak [42]. The cases occur beyond the incubation period of LD (usually less than 10 days), indicating an ongoing source of contamination. From this, the source could be either a contaminated aerosol or a colonized water distribution system. The curve also shows that the cases declined rapidly starting 6 days before the Opera House Hotel cooling tower was disinfected, strongly suggesting that this was not the source of the outbreak.
The NYC DOH South Bronx outbreak map (Figure 4) shows 85 case locations including the Opera House hotel. The red circles represent cases with patient samples matching samples from the hotel. The outbreak map for LMMHC (Figure 5) shows case locations for the 48 patients treated and adds the Melrose Houses (four patients), the Opera House hotel (two patients) and the SHR (one patient added) for a total of 55 cases. Neither map shows clustering around the official source. The cases are widely and seemingly randomly scattered. The DOH selected cooling towers for environmental testing and publicly stated that the "NYC water supply was unaffected".
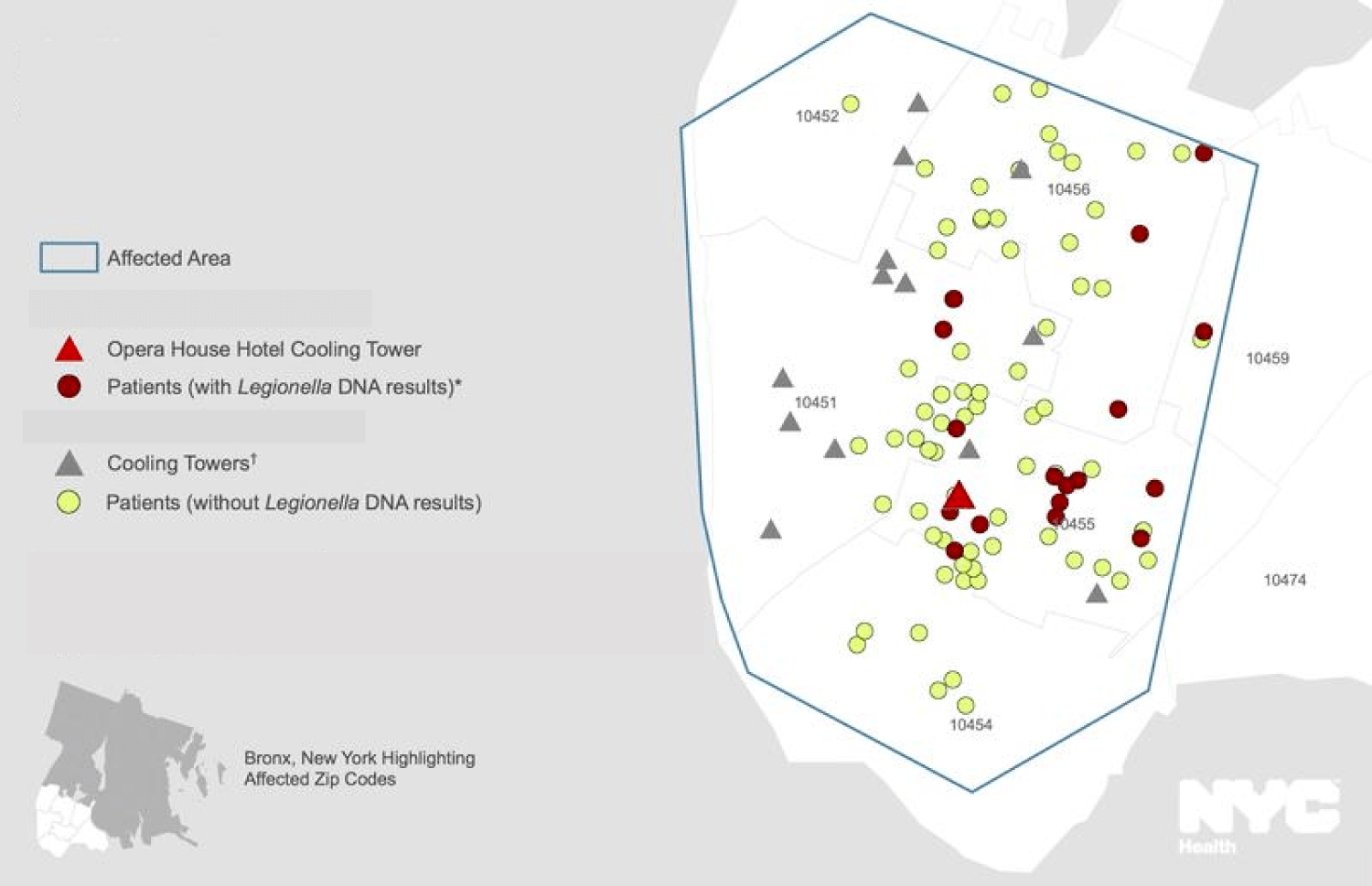 Figure 4: 2015 NYCDOH South Bronx Legionnaires' disease Outbreak Map [33].
View Figure 4
Figure 4: 2015 NYCDOH South Bronx Legionnaires' disease Outbreak Map [33].
View Figure 4
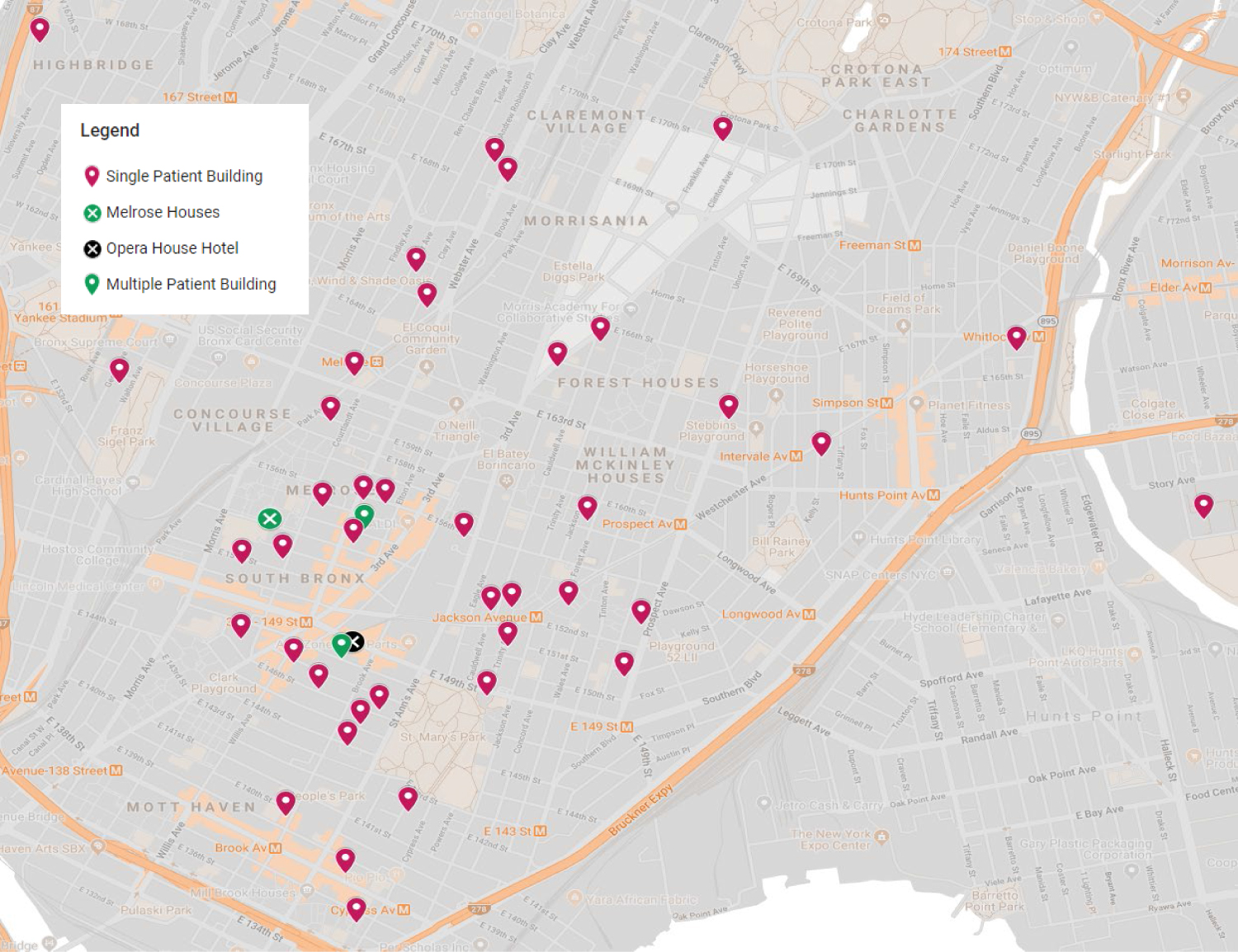 Figure 5: 2015 LMMHC Legionnaires' disease Outbreak Map.
View Figure 5
Figure 5: 2015 LMMHC Legionnaires' disease Outbreak Map.
View Figure 5
In the beginning of September, 2015, it was announced that Legionella had been found in the water distribution system of multiple buildings in the Melrose Houses and the potable water was formally identified as the source of the LD cases in that location. Two of these cases actually occurred in July, at the height of the South Bronx outbreak. The outbreak map shows that the buildings are centrally located in the initial outbreak zone. This group of cases was officially classified as a different outbreak. WGS on the clinical or environmental isolates was not published. The DOH statement at that time regarding the protocol of testing the potable water due to the presence of "two patients in one building" is consistent with CDC outbreak guidance [43]. By July 29, 2015, the Opera House hotel and the SHR had multiple documented cases in each building. The LMMHC outbreak map shows an additional building, one block from the Melrose Houses, which also housed multiple patients during that month. Given that this map only shows 35% of all cases, it would be important to know how many more residences for the rest of the population had multiple cases per building and did not have potable water testing performed.
The Morris Park outbreak was of interest due to the decision to test cooling towers as the source of infection, given the disinfection of all city cooling towers that was completed one month earlier. The fact that 15 towers tested positive for Legionella suggests that either disinfection is of limited value in preventing cooling tower related LD, or that the municipal water supply was heavily colonized, perhaps causing both reintroduction of Legionella to the cooling towers and the outbreak itself. That the strain found in this East Bronx outbreak was so closely related to the South Bronx infecting strain again suggests that the municipal water supply was compromised.
While industrial cooling towers have been confirmed sources of LD, residential cooling towers are unusual causes of LD, especially in New York, as noted [7,23]. The cooling tower in Pas-de-Calais was 15 meters high and produced nearly 200 liters per hour of aerosolized water. The residential cooling towers in New York City, such as the one for the Opera House Hotel, are small by comparison with modern drift eliminators in place that remove most of the water from the exiting air. They aerosolize less than 2 liters of water per hour. After passage across these drift eliminators there are typical concentrations of 0.00002 ml of water per liter of exhaust air. This means that if contaminated water levels reached 1000 CFU/ml of Legionella, there would only be 1 bacterium in 50 liters of exhaust air. Breathing in exhaust air directly from the blower for one hour (15 breaths per minute with 500 ml tidal volume) would potentially expose the nasopharynx and lungs to no more than 10 bacteria. By contrast, even if the potable water was far less contaminated at 10 CFU/ml of Legionella present, the oropharynx would be exposed to more than 2,000 bacteria in a matter of seconds by drinking 1 glass of colonized water.
Whole genome sequencing is increasingly used in LD outbreak investigations due to its higher resolution than standard sequence-based typing. The lack of a DNA match between clinical and environmental specimens can definitively rule out a possible source, however, an exact match only proves that there is a potential source, given that multiple water features in any area can be contaminated with the same organism. In the 2013 Warstein, Germany LD outbreak, the largest in that country's history, core genome multi-locus sequence typing was used to identify two strains from an industrial cooling tower that matched the patient isolates [44]. However, they also found the same exact DNA match in the local river and in 2 water treatment plants. In this New York outbreak, WGS was used to officially name the Opera House hotel and the VAMC cooling tower as the definitive sources for the South Bronx and Morris Park outbreaks, respectively, based on DNA matches with a small number of patient cultures (4 isolates for Morris Park and 26 isolates for the South Bronx) [28,31]. No other sources were considered despite patient interviews showing that only 37 total patients had ever been within a 3 block area surrounding the Opera House hotel prior to their illness onset during the South Bronx outbreak [28]. When the municipal water supply was examined due to "two patients in one building", the environmental and patient isolates did match and this was officially declared a separate outbreak despite the timing and location noted. The primary point is that colonization of the potable water supply is always the original source of the bacteria and should be evaluated.
The standard use of Legionella urine antigen testing in acute respiratory infections allowed LMMHC to rapidly diagnose and appropriately treat patients encountered during this outbreak. At that time, The IDSA guidelines for CAP considered Legionella urine antigen testing as optional and only formally recommended the test for the most severe cases [24]. Beta-lactam antibiotics were avoided at LMMHC because of early diagnoses. This is the most likely reason for the low mortality seen in this cohort, given that delays in therapy lead to higher mortality for pneumonia [45]. LD mortality rates from 28-33% have been found in studies of both sporadic and outbreak cases treated in ICU settings with Apache scores similar to our cohort [17-19].
We could find no clinical differences to account for the low mortality. The radiographic presentations were similar to what has been described previously with lobar consolidation found in nearly all patients [46-48]. Our rate of hyponatremia was similar to the 26-30% rates documented in other outbreaks [49,50]. Altered mental status occurred at rates similar to the encephalopathy rates documented in studies of both outbreak and sporadic LD that have ranged from 17-40% [12,46,51,52]. The 38% rate of gastrointestinal symptoms in this cohort was only slightly higher than the range of 18-32% seen in the same outbreak and sporadic groups noted. Rhabdomyolysis rates of 20-26% have been documented in sporadic case series, while our neighboring Bronx hospital found Rhabdomyolysis in 43% of their LD cases during this outbreak [52-54]. This is similar to the 31% rate in our cohort.
Our standard use of Legionella urine antigen testing also allowed LMMHC to notify the NYC DOH before their automated systems noted any signs of the outbreak. LMMHC notified the DOH one day before their SaTScan system alerted them to a cluster of cases and 11 days before their historical limits method alerted them to the narrow location in two Bronx neighborhoods around our hospital. Additionally, we were the first to notify our neighboring hospital and alert them to the outbreak. They diagnosed 35 cases of LD. Their rate of ICU admission was the same as LMMHC (40%) and their overall mortality was 9%.
The formal investigation of the 2015 New York City Legionnaires' disease outbreak by the NYC DOH, the CDC and the New York State DOH led to an official statement: "This analysis warns us that because of the particular biologic and ecologic nature of L. pneumophila, reliance solely on 1 source of evidence (epidemiologic approaches or molecular data) might be insufficient to identify exact sources of Legionellosis outbreaks" [31]. We strongly agree with this statement and would recommend that existing CDC guidelines be closely followed in the future. The routine use of Legionella urine antigen testing allowed LMMHC to identify this outbreak and improve treatment for patients in multiple hospitals during this epidemic.
This study was approved by the Lincoln Medical and Mental Health Center Medical Center Institutional Review Board.
Not Applicable.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
No funding was required for this study.
All authors read and approved the final manuscript.
YS collected the initial data to define the patient population.
MAH, JM, IEH, EG, and MR collected and reviewed all of the original patient data for accuracy.
TT, MG, and IB reviewed the radiology data.
NC reviewed the emergency room treatment of the patients.
RB reviewed the ICU treatment and evaluation (Apache scores etc.) for the patients.
KH made extensive revisions to the final manuscript.
MS wrote the final manuscript.
Not applicable.
Not applicable.