Globally, the COVID-19 pandemic has resulted in immeasurable disruptions in countries activities. Since the first reported case in December 2019, an estimated 140,000 people have died, with a case fatality rate of about 3%. The increasing rate of new cases and the evolving epidemiology of the COVID-19 virus means that the global health community is grappling to understand the current situation. The aim of this paper is to determine if the Bacilli Calmette-Guerin (BCG) vaccine used to protect against childhood tuberculosis in TB endemic countries provides a protective effect against the SARS-COV-2 virus.
A cross-sectional study to establish the relationship between BCG vaccination policy and COVID-19 infection in 178 countries. Information on the BCG policies of 178 countries and COVID-19 were extracted from the BCG world atlas and the World Health Organization COVID-19 situation report of April 7, 2020. Chi square tests were used to determine statistical significance. Spearman's rank-order correlation was used to determine if a relationship exist between BCG policy and COVID-19 cases and deaths in 178 countries.
There is a strong correlation between BCG vaccination and incidence of COVID-19 cases. Two countries who had no BCG vaccination policy had over 100,000 confirmed cases and higher case fatalities. Chi square statistics showed a significant difference in COVD-19 related death between country with BCG vaccination policy and those without it; including those who had in the past but not anymore, (χ2 = 122.264, df 12, p < 0.0005). Spearman rank-order correlation shows statistically significant, strong negative correlation between countries BCG vaccination policy and confirmed COVID-19 cases and death (BCG policy and confirmed cases - correlation coefficient -0.427, p < 0.0005), BCG policy and COVID-19 related death - correlation coefficient -0.374, p < 0.0005).
We conclude that countries with robust BCG vaccination policy had lower case fatality of COVID-19 however further studies will be needed to determine the level of protection offered by the BCG vaccination against the SARS-COV-2 virus.
BCG, Vaccine, COVID-19, SARS-COV-2, Virus
The COVID-19 pandemic continues to cause serious havoc around the globe, spreading to 185 [1] countries since it was first reported in December 2019 in Wuhan, China. It was declared a pandemic by the World Health Organisation (WHO) on March 11, 2020 [2]. The disease is caused by SARS-COV-2 virus, a member of the corona group of viruses. Corona virus belongs to the group Coronaviridae and is said to be an established pathogen affecting both humans and animals. The corona viruses were initially classified into three groups based on their antigenic properties of the spike (S), membrane (M) and nucleocapsid (N) proteins. Group 1 family has the genetic phylogeny HCoVs and NL63, group 2 has OC43, HKU-1 and SARS coronaviruses, and group 3 codes are found in avian species [3]. The first known severe illness caused by a coronavirus was seen in 2003 during the Severe Acute Respiratory Syndrome (SARS) epidemic in China. Similarly, a second outbreak of severe illness occurred in 2012 in Saudi Arabia with the Middle East Respiratory Syndrome (MERS).
Due to genetic recombination between members of the same and different groups of corona virus, opportunity exists for increased genetic diversification. SARS-COV-2 virus is a novel strain which was recently transmitted to humans possibly from animals such as bats, with human to human transmission now widely documented. According to WHO, SARS COV-2, the virus that causes COVID 19 is primarily transmitted from a symptomatic person to another, however, transmission from an asymptomatic person is said to be possible [4].
Since COVID-19 was declared a pandemic by WHO, there have been speculations about the possibility of the SARS-COV-2 infection and fatality being lower in countries with routine BCG vaccination policy and practice despite the fact that evidence to support such hypothesis has been non-existent because COVID-19 remains a novel disease. The Bacilli Calmette-Guerin vaccine (BCG) was discovered over 80 years ago and is currently one of the most widely used vaccines globally. More than 80 percent of neonates and infants in countries where BCG is part of the national childhood immunization program have benefited from the vaccine which has been documented to have protective effect against meningitis and disseminated tuberculosis (TB) in children [5].
Since BCG protects against disseminated TB through triggering a robust T-cell type IV hypersensitivity reaction in the alveoli of adults and infants [6], it has been suggested that this type of reaction may be the bases for the protection against SARS-COV-2 virus, since this novel virus primarily affects the lung alveoli lining. SARS-COV-2 virus is found in abundance in certain progenitor cells which normally develop into respiratory tract cells lined with hair-like cilia projections, which sweeps bacteria and mucus out of the lungs [7]. Thus, those with severe COVID-19 infection present with respiratory distress and in critical cases lung collapse.
After an expansive search of peer-reviewed articles linking COVID-19 with BCG, we found only two articles with evidence suggesting BCG may play a role in protecting against severe lung disease during COVID-19 infection. One study by Dayal and Gupta [8], found a significant difference in the case fatality rate (CFR) between countries after comparing the impact of COVID-19 in terms of CFR between countries with high disease burden and those with National revaccination BCG policy. The study concluded that vaccination practices provide added protection to the population against severe SARS-COV-2 infection [8].
In another study by Miller, et al. comparison was made between BCG vaccination policy of large number of countries and COVID-19 related morbidity and mortality. This study found that countries that do not have a universal policy for BCG vaccination are more severely affected by COVID-19 compared to countries with a universal and long-standing policy for BCG. This finding is consistent with the idea that BCG may protect the vaccinated elderly population. The study by Miller, et al. and Dayal and Gupta covers 60 and 24 countries respectively. This study looks at data from 178 countries across the globe. It will contribute new information to the body of knowledge emerging around this relationship. Additionally, this study provides a snapshot at a time when most countries have reached peak infections, however, it should be noted that some countries are still seeing rising number of cases [9].
1. Investigate the relationship between routine BCG vaccination and severity of SARS-COV-2 cases and fatality.
2. Establish if there is a correlation between BCG policy and SARS-COV-2 infection at multicounty level.
A cross-sectional study design was used to assess the relationship between BCG policy and COVID-19 outcomes in 178 countries. This study looked at total number of confirmed cases, and total deaths from the inception of the novel virus in December 2019 up until the April 07, 2020. Data on the BCG policies from 178 countries and COVID-19 cases and deaths were extracted from the BCG world atlas and the WHO COVID-19 situation report as at 10:00 Central European Time on 7th April 2020, respectively. The countries were categorized into three, with 0 representing countries with no BCG policy, 1 representing countries that used to have BCG policy but not anymore, and 2 representing countries with routine immunization policy. We assessed population data of 178 countries from worldometer as at May 14, 2020 [10].
The total number of confirmed cases and mortality from COVID-19 were recoded with the code range increasing as the number increases (code 1 being the lowest range and code 7 for countries with the highest confirmed cases and total death). For total confirmed cases, the following codes were used: 1 = < 100, 2 = 100-999, 3 = 1000-9999, 4 = 10,000-19,999, 5 = 20,000-49,000, 6 = 50,000-99,999, and 7 = > 100,00. For total confirmed death: 1 = < 10, 2 = 10-99, 3 = 100-499, 4 = 500-999, 5 = 1000-4999, 6 = 5000-9999, and 7 = > 10,000. The population of the countries from worldometer estimates was used to determine number of cases and death per 1 million persons. The countries were categorized into low, medium, and high depending on the percentile number of cases and death per 1million population. The classification is as follows:
Low = < 25 percentile
Medium = between 25-75 percentile
High = Above 75 percentile
Data was summarized using both descriptive and inferential statistics. Chi square was used to assess whether the difference in the outcome of COVID 19 in the listed countries based on BCG policy is statistically significant or not. Scatter plot was developed and visually inspected to assess if the data is monotonic. Fishers exact test was also conducted as some of the cells have values less than 5.
Spearman rank-order Correlation was conducted to identify if there is a relationship and determine the direction of the relationship between BCG policy and COVID 19 impact on the 178 listed countries. Significance level was set at 0.05. Data was analyzed using SPSS version 24.
Two countries without BCG policy had COVID 19 cases of over 100,000 and over 5,000 total deaths. While 161 countries with BCG policy had less than 1000 confirmed cases and less than 500 deaths as shown in Table 1.
Table 1: Total numbers of cases and deaths in the different categories of countries based on BCG vaccination policy. View Table 1
Table 2 shows BCG vaccine policy and total confirmed cases. For total number of confirmed COVID-19 cases, 1 country with no BCG policy had between 10,000-19,999 cases while 2 countries also with no BCG policy had above 100,000 confirmed cases. For countries that used to have BCG policy but no more, 2 countries had between 100-999 cases, 7 = 1,000 to 9,999, 1 = 10,000-19,999 3 = 50,000-99,999. 1 country had > 100,000 confirmed cases from this group. Lastly for countries with routine BCG immunization policy, 64 = 0-99, 52 = 100-999, 36 = 1000-9,999, 4 = 10-19,999, 3 = 20,000-49,000 and 2 = 50-99,999 cases. There is no country with > 100,000 confirmed COVID-19 cases among the group which have routine BCG immunization policy in place.
Table 2: BCG vaccine policy and total confirmed cases. View Table 2
The Chi square and Fisher's exact test in Table 3 show a significant difference in COVD-19 confirmed cases between country with BCG vaccination policy and those without it (including those who had in the past but not anymore) (χ2 = 122.264, df 12, p < 0.0005). Out of 178 countries analyzed, 161 Countries have routine BCG immunization policy, 14 countries used to have vaccination policy but no more, and 3 countries had no BCG vaccination policy.
Table 3: Chi-square tests. View Table 3
Table 4 showed BCG vaccine policy and total confirmed deaths. Out of 178 listed countries, for those with no routine BCG policy in place, 1 had death between 100-499, 1 between 5,000-9,999 and 1 > 10,000. For countries that used to have routine BCG immunization but no more, 2 = 0-9, 4 = 10-99, 4 = 100-499, 1 = 1,000-4,999, 2 = 5,000-9,999. 1 country had > 10,000 confirmed death in this group. Lastly for countries with routine BCG immunization, 99 = 0-9, 46 = 10-99, 10 = 100-999, 2 = 500-999, and 4 = 1,000-4,999. There is no country in this group with death of up to 5,000 and above. Absolute number of COVID-19 related mortality is higher in countries without BCG policy.
Table 4: BCG vaccine policy and Total confirmed deaths. View Table 4
In Table 5, the Chi square statistics and Fisher's exact test show a significant difference in COVD 19 related death between country with BCG vaccination policy and those without it (including those who had in the past but not anymore) (χ2 = 86.581, df 12, p < 0.0005). Absolute number of COVID-19 related mortality is higher in countries without BCG policy.
Table 5: Chi-Square Tests for significance. View Table 5
Table 6 shows the BCG policy and COVID 19 cases and death adjusting for countries' population. Countries with BCG policy were observed to have lower COVID 19 cases and deaths attributable to COVID 19 per 1million persons.
Table 6: COVID-19 cases and deaths categorization per 1 million population. View Table 6
In Table 7, the Chi Square test and Fisher's exact test results of Countries' BCG policy and cases and death due to COVID19. It shows there is a significant difference between countries with BCG policy and number of cases of COVID 19 per million persons (χ2 = 28.941, df - 4, p < 0.005) death due to COVID 19 (χ2 = 16.178, df - 4, p = 0.003).
Table 7: The Chi Square test and Fisher’s exact test results of Countries’ BCG policy and cases and death due to COVID19. View Table 7
Spearman rank-order correlation was run to assess the relationship between countries' BCG vaccination policy and confirmed cases and death from COVID-19. Preliminary analysis showed the relationship to be monotonic as assessed by visual inspection of scatterplot (Figure 1 and Figure 2). In Figure 1 below, preliminary analysis shows the relationship between total number of COVID 19 cases and countries' BCG policy to be monotonic as assessed by visual inspection of scatterplot which also reveals that countries with BCG policy had less COVID-19 cases while countries with no BCG policy or previous policy had higher number of cases of COVID-19.
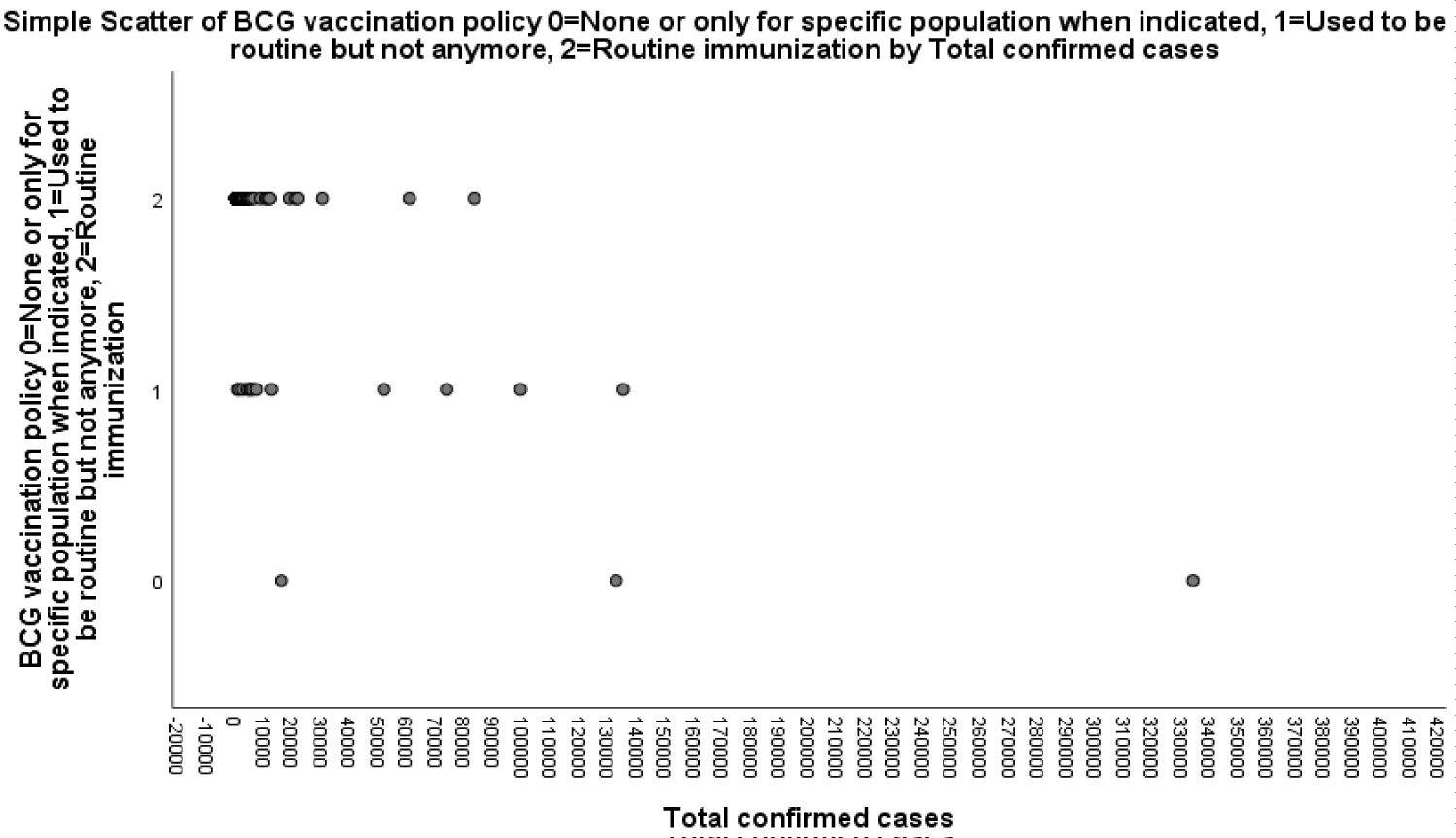 Figure 1: Scatter plot showing monotonic relationship between COVID-19 confirmed cases and countries’ BCG policies.
View Figure 1
Figure 1: Scatter plot showing monotonic relationship between COVID-19 confirmed cases and countries’ BCG policies.
View Figure 1
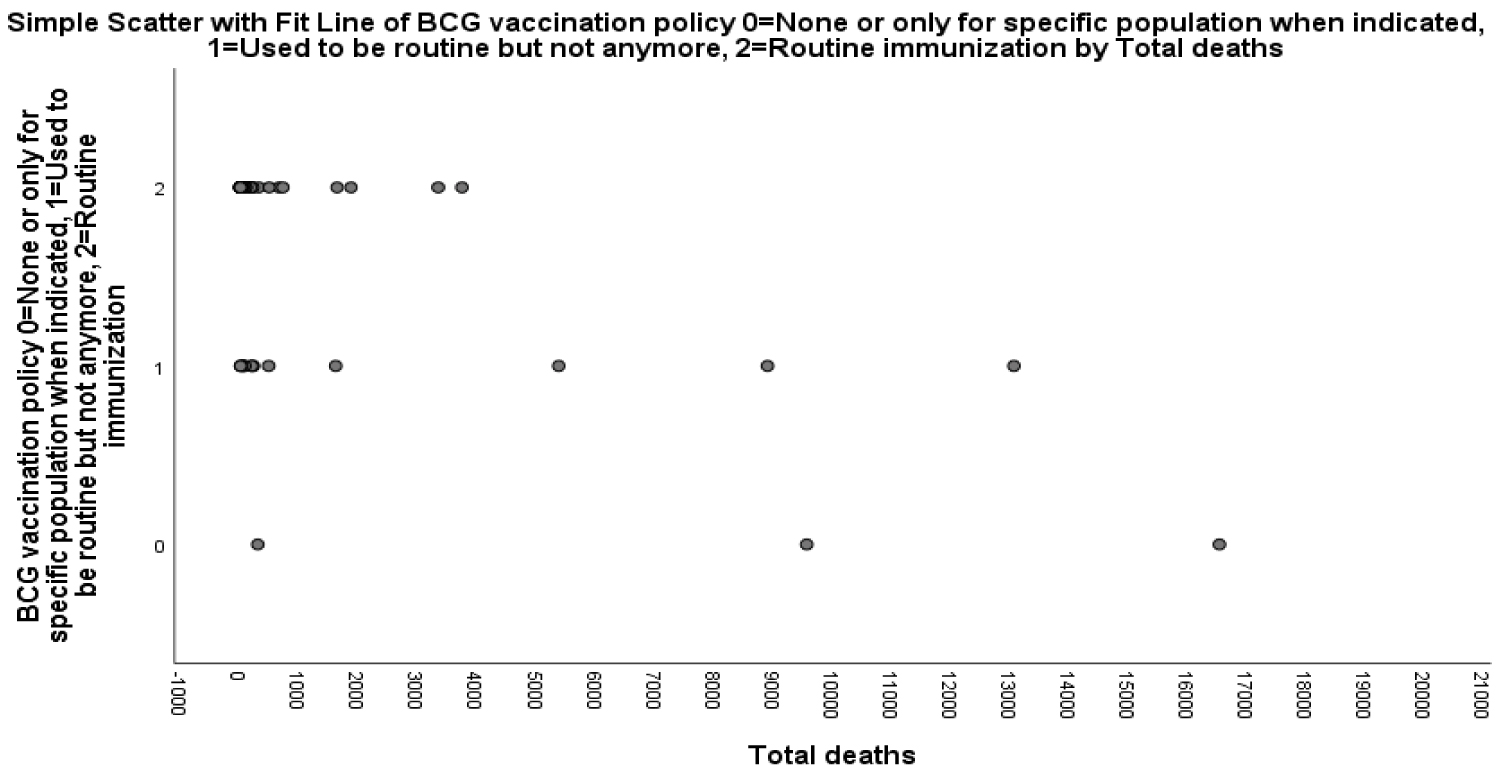 Figure 2: Scatter plot showing monotonic relationship between COVID-19 confirmed deaths and countries’ BCG policies.
View Figure 2
Figure 2: Scatter plot showing monotonic relationship between COVID-19 confirmed deaths and countries’ BCG policies.
View Figure 2
Figure 2 below, preliminary analysis shows the relationship between total number of deaths attributable to COVID-19 and countries' BCG policy to be monotonic as assessed by visual inspection of scatterplot which also reveals that countries with BCG policy had less COVID-19 attributable death while countries with no BCG policy or previous policy had higher number of death attributed to COVID-19.
Table 8 further showed the correlation between BCG vaccination policy and COVID-19 confirmed cases and COVID 19 related deaths. There was statistically significant, strong negative correlation between countries BCG vaccination policy and confirmed COVID-19 cases and death. (BCG policy and confirmed cases - correlation coefficient -0.427, p < 0.0005), BCG policy and COVID-19 related death - correlation coefficient -0.374, p < 0.0005).
Table 8: Correlations. View Table 8
Since the first case of COVID-19 was reported on 31st December 2019 in Wuhan, China, the disease has spread globally making WHO to declare it a pandemic on March 11, 2020 [2]. It remains a disease of mounting public health concern. However, the impact of COVID-19 has not been the same across countries [11]. Whilst the search for curative medicines and preventative vaccines frantically continues, the BCG vaccine, which was developed primarily against tuberculosis was speculated to provide some level of protection against COVID-19. This speculation is linked to data which suggests that low and middle income countries (LMIC) appear to have lower number of cases and deaths due to COVID-19 [12].
BCG is no modern miracle. It was developed by French physicians and biologists Léon Charles Albert Calmette and Jean-Marie Camille Guérin in the 1900s and was first successfully tested in 1921 [11]. It is the only vaccine available today against tuberculosis and has been in use with astonishing safety records [13] for about a century.
A total of 1,276,010 cases and 72,540 deaths have been recorded across the 178 countries of interest during the study period from the inception of the virus in December 2019 up until April 7, 2020. The 178 countries were divided into 3 groups based on their BCG vaccination policies. Three of the countries never had routine BCG vaccination policy, and they made up the first group. The second group had routine BCG vaccination policy in the past, but not anymore, they were 14 in number. The remaining 161 countries which made up the third group currently have routine BCG vaccination policy in place to routinely administer BCG as a preventive measure against tuberculosis.
Among the three countries (Italy, USA, and Canada) without universal BCG vaccination policy and practice, two of them (USA and Italy) were found to have over 100,000 confirmed cases of the novel coronavirus infection. Among the countries that had routine BCG vaccination in the past, one of the 14 countries, Spain had over 100,000 cases, while none of the 161 countries with routine BCG immunization policy had over 100,000 cases (though two countries have between 50,000-99,99 cases). When the numbers of cases per 1 million population was compared among the 178 countries, those without universal BCG vaccination policy all had a high number of cases compared to only 1 in 5 countries that currently have BCG vaccination policy in place. In the same vein, when the numbers of deaths per 1 million population for the countries were compared, one-third of the countries without BCG vaccination policy had high mortality whilst only 3 out of 100 countries with BCG vaccination policy had high mortality. The findings here are consistent with that of Miller, et al. who also found that BCG vaccination correlates with significantly less COVID-19 reported infections. Miller, et al. further suggested that BCG might confer some protection specifically against COVID-19 [9] (Figure 3 and Figure 4).
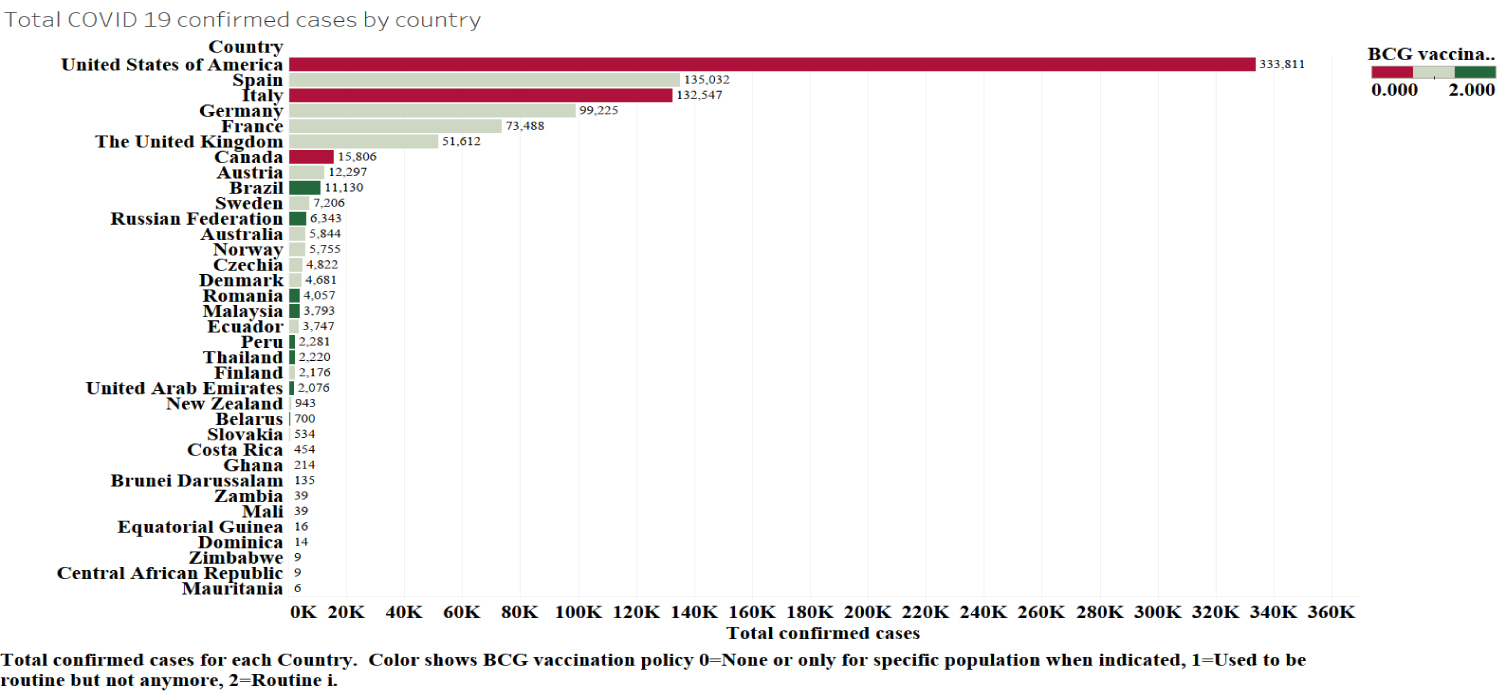 Figure 3: Color coded horizontal bar chart showing confirmed cases of COVID-19 in all countries without current BCG policy and randomly selected countries with current BCG policy.
Figure 3: Color coded horizontal bar chart showing confirmed cases of COVID-19 in all countries without current BCG policy and randomly selected countries with current BCG policy.
Red = No BCG policy; Brown = Had BCG policy but no more; Green = Current BCG policy.
View Figure 3
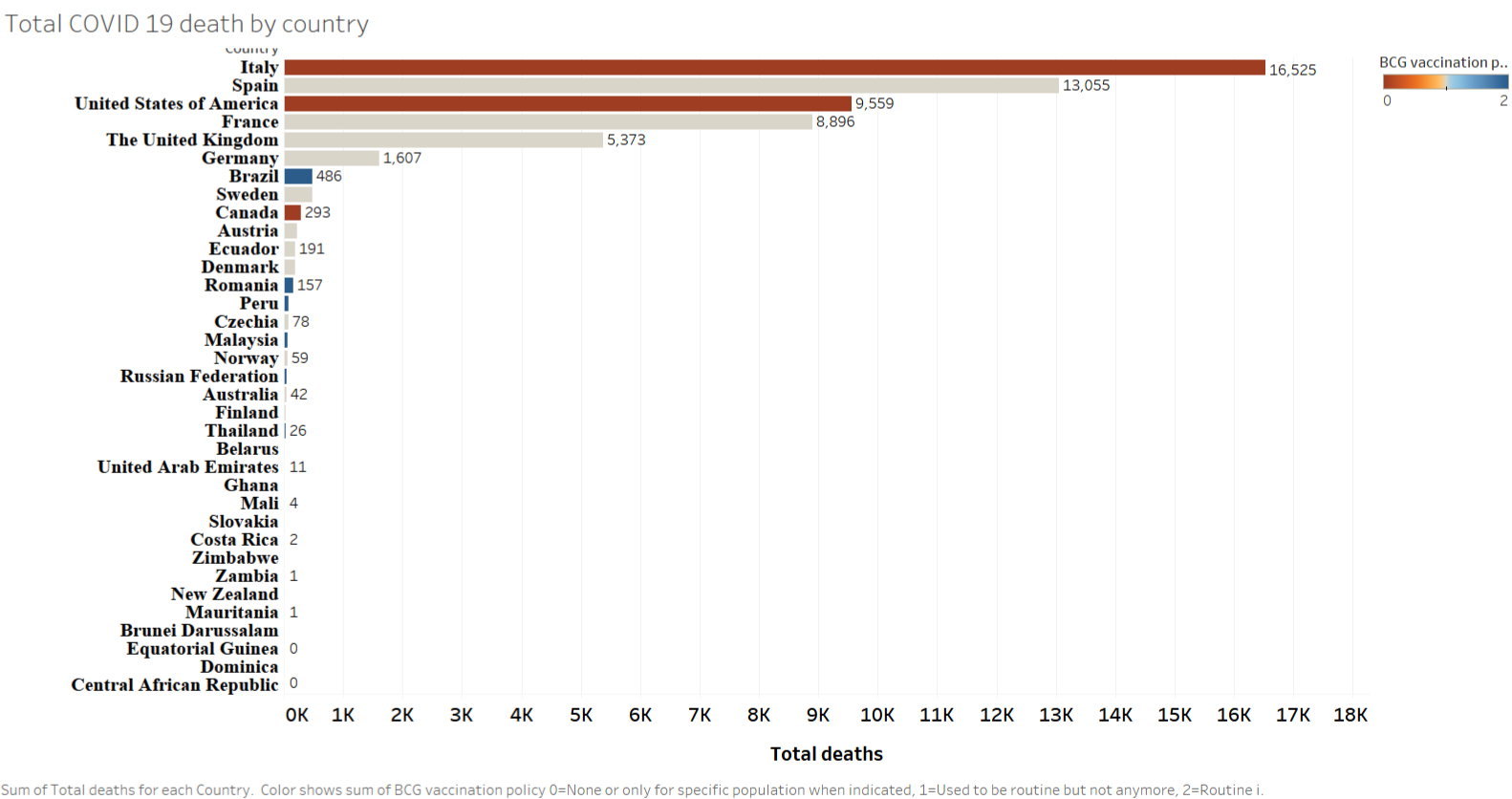 Figure 4: Color coded horizontal bar chart showing Number of deaths due to COVID-19 in all countries without current BCG policy and randomly selected countries with current BCG policy.
Figure 4: Color coded horizontal bar chart showing Number of deaths due to COVID-19 in all countries without current BCG policy and randomly selected countries with current BCG policy.
Red = No BCG policy; Brown = Had BCG policy but no more; Blue = Current BCG.
View Figure 4
Out of the over 100,000 cases that were reported in the 2 countries without routine BCG administration, one recorded over 10,000 deaths. In the second group of countries, Spain that had over 100,000 cases was the only country in the group that had also recorded over 10,000 deaths [14]. Countries with BCG vaccination (161) had fewer deaths compared to the other two categories. There is no country in this group with up to 10,000 deaths. In the study carried out by Dayal and Gupta, the case fatality rates (CFR) between the countries with high COVID-19 burden and the countries which had followed BCG revaccination policies in the past was compared, and there was an observed marked difference in the mean CFR between the two groups of countries [8]. Data from Miller, et al.'s study tentatively suggests that BCG vaccination could significantly reduce mortality associated with COVID-19 [9]. Findings from this study on BCG and COVID-19 mortality show similar results to both Dayal and Gupta, and Miller, et al. studies. This study however looked at greater number of countries with higher cases and mortality data. Comparison was also made based on population size.
This study further identifies that there is a correlation between BCG vaccination policy and COVID-19 confirmed cases and deaths. The result suggests that BCG vaccine might be protective against coronavirus infection and death [9].
This study is limited by the lack of adjustment for possible confounding factors such as the quality of the health care system by country, COVID-19 surveillance systems, territorial extension and testing capacity of the 178 countries which may impact on number of confirmed cases and deaths. Countries with high quality responsive healthcare systems which are accessible, available, and affordable to all may perform better in saving lives, however public health systems and good governance related to lockdown behaviour and test and trace capacity are also critical factors in any comparison.
This study has clearly shown that countries with routine BCG vaccination policy have significantly lower COVID-19 cases and deaths compared to countries who had BCG vaccination policy in the past or those that never had one. However, there is no current evidence that BCG is a protective factor again COVID-19. Studies that controls for the limitations outlined above are required to determine how much of protection the BCG vaccine can offer against COVID-19 infection. A number of RCT trials have commenced to investigate this correlation further. The world will watch with interest as the results unfold.
The authors certify that they have no potential conflict of interest in the subject matter or materials discussed in this manuscript.
All authors equally contributed to the design, implementation of the research, analysis of the results and writing of the manuscript.