Some tuberculosis locations are rare or even exceptional and mammary tuberculosis (MT) is the least frequent one among visceral locations. MT still presents difficulties both in its diagnosis and treatment. We're reporting the case of a 24-years-old female patient, with no medical history, for instance, no tuberculosis contact. She was admitted for exploration of a fever associated to a general state deterioration, and arthralgia, the physical examination found a lump in her right breast, an erythema nodosum and bilateral ankle arthritis.
The diagnosis of mammary tuberculosis was made based on bacteriological evidence and a favorable evolution under anti bacillary treatment. Through available literature data, we will review the epidemiologic, clinical, diagnostic and therapeutic properties of this affection. Through this case, we will also bring up the problem of MT differential diagnosis with other mammary granulomatosis especially idiopathic granulomatous mastitis; we will then discuss the benefit and the place of corticotherapy as an adjuvant treatment of MT.
Tuberculosis, Mastitis, Idiopathic granulomatosis, Anti bacillary, Corticotherapy
Mammary tuberculosis (MT) is a granulomatous mastitis, due to an infection by bacteria belonging to Mycobacteriaceae family, also called Koch's bacillus (KB). It's the least frequent visceral locations of tuberculosis. It's a rare affection even in countries where the incidence of pulmonary and extra-pulmonary tuberculosis is still very high.
MT can be confused with breast cancer, an abscess, or another inflammatory granulomatosis that can be infectious or not.
The diagnosis can't be confirmed unless the anatomopathological examination shows the classic epithelioid cell granuloma with caseating necrosis or the bacteriological examination finds the KB (Mycobacterium tuberculosis).
The objective of this case was to describe our experience and to highlight the diagnosis and treatment difficulties we faced in front of this rare form of MT.
A 24-years-old female patient, married, primigravida, primipara, under combined hormonal contraceptives, with no medical or surgical history or tuberculosis contact, was admitted for exploration of a fever associated to a general state deterioration and bilateral ankle arthralgia.
Her medical history was within normal limits, except for the appearance of a breast lump two months and of multiple red painful nodules in her extremities one week prior to her hospitalization.
Her vital parameters consisted of a heart rate at 90 beats/minute, a blood pressure at 120/70 mmHg, a respiratory rate at 21 cycles/minute and a temperature at 38 °C. Physical examination found a quite red and hot right breast compared to the left one. The right breast also had an indurated lump with a major axis measuring 6 cm (Figure 1a and Figure 1b), that was painful to the touch and with an ipsilateral axillary adenomegaly. The examination also pointed out multiple red, hot and hyperalgic nodules on the extensor surface of her two lower limbs, which undoubtedly evoked an erythema nodosum associated to (Figure 1c) bilateral ankle arthritis. The pleuropulmonary examination was normal, no rales were heared. The cardiovascular examination found no abnormalities and there was no splenomegaly or hepatomegaly in the abdominal examination.
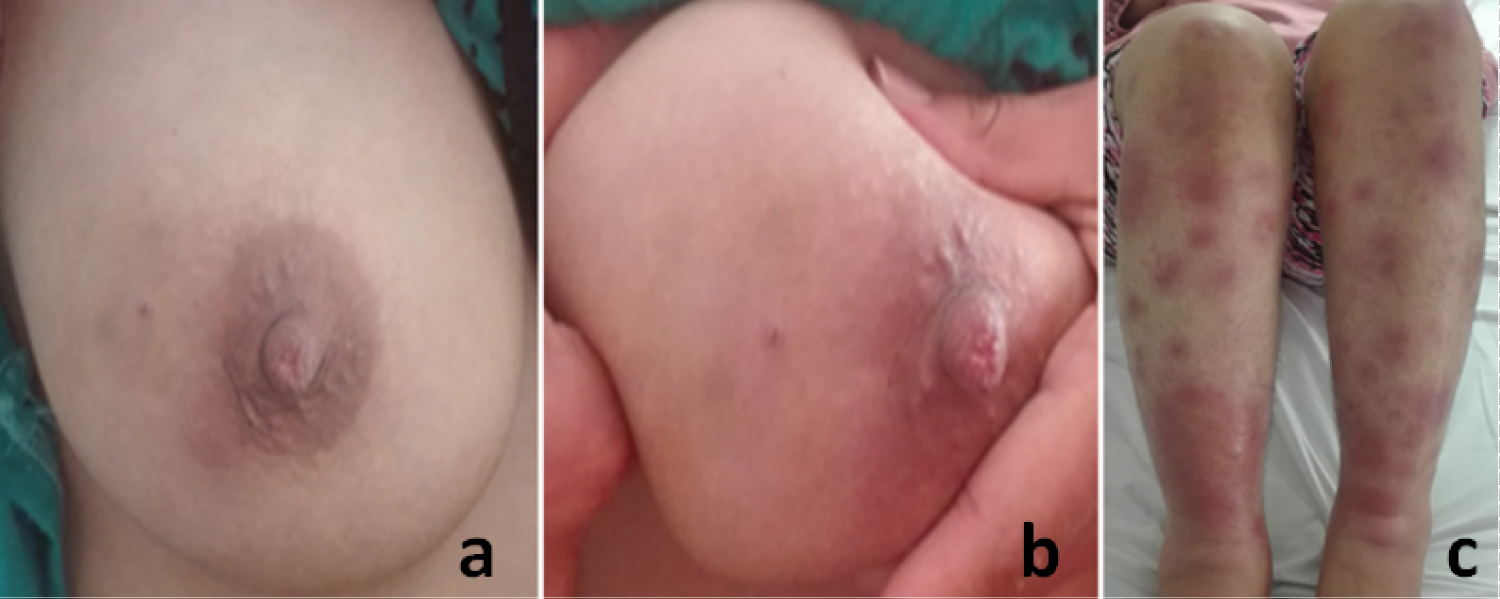 Figure 1: (a,b) An inflammatory mass in the upper outer quadrant of the right breast; (c) Diffuse erythematous nodular lesions on the lower limbs.
View Figure 1
Figure 1: (a,b) An inflammatory mass in the upper outer quadrant of the right breast; (c) Diffuse erythematous nodular lesions on the lower limbs.
View Figure 1
The biological check-up showed a major inflammatory syndrome consisting of a high sedimentary rate with 96 mm in the first hour (Normal rate : < 30), an elevated C-reactive protein of 320 mg/l (Normal rate: < 6) and a normal procalcitonin level. Blood count revealed a hyperleukocytosis of 16400/mm3 which was predominantly neutrophilic. Both urinary and blood calcium and phosphate levels were normal. The angiotensin converting enzyme rate was normal. The QuantiFERON®-TB Gold IT test was negative.
The tests of rheumatoid factor, antinuclear antibodies, antiphospholipid antibodies, antineutrophil cytoplasmic antibodies, antithyroperoxidase antibodies and thyroglobulin antibodies were all negative. The serologies of hepatitis B and C, HIV and syphilis were negative as well. The ASLO rate was normal. The stool culture and parasitological examination of stool were without abnormalities.
The chest X-ray was normal, it showed no signs of tuberculosis or sarcoidosis, a pulmonary high resolution CT scan was normal as well.
The mammography showed a dense ill-defined opacity in the outer quadrants of the right breast. The mammary ultrasound pointed out an irregular ill-defined mass in the junction of the outer quadrants of the right breast, measuring approximatively 51 × 25 mm. It was hypoechoic, heterogeneous and non-attenuating, it also had a starting fistulous opening through the subcutaneous tissue in the peri-mammillary region, and was associated to a diffuse fatty infiltration and some inflammatory looking ipsilateral adenomegalies with a fatty hilum. The MRI was in favor of a right mastitis (Figure 2).
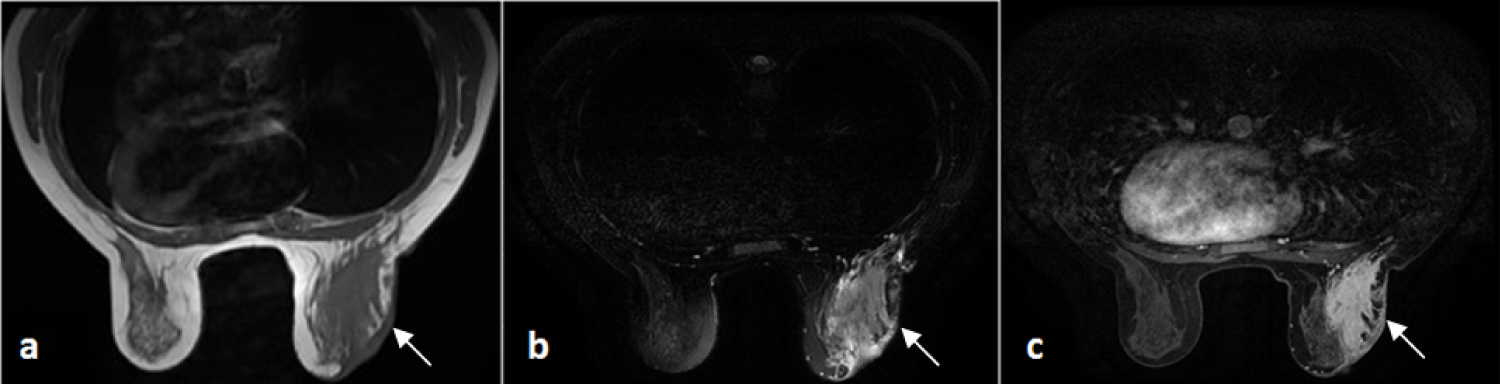 Figure 2: Axial sections in T1-weighted scanning sequences (a) T2; (b) After injection; (c) Showing a right mammary infiltration that's isointense T1, hyperintense T2 and strongly enhanced after injection, associated to a skin thickening, a mammillary retraction and ipsilateral axillary adenopathy.
View Figure 2
Figure 2: Axial sections in T1-weighted scanning sequences (a) T2; (b) After injection; (c) Showing a right mammary infiltration that's isointense T1, hyperintense T2 and strongly enhanced after injection, associated to a skin thickening, a mammillary retraction and ipsilateral axillary adenopathy.
View Figure 2
The mammary biopsy, that found no signs of malignancy, was in favor of a granulomatous mastitis. It showed an inflammatory granulomatous reaction with epithelioid follicles in different sizes without caseating necrosis within the mammary tissue (Figure 3). A biopsy of accessory salivary glands was performed, and it was normal.
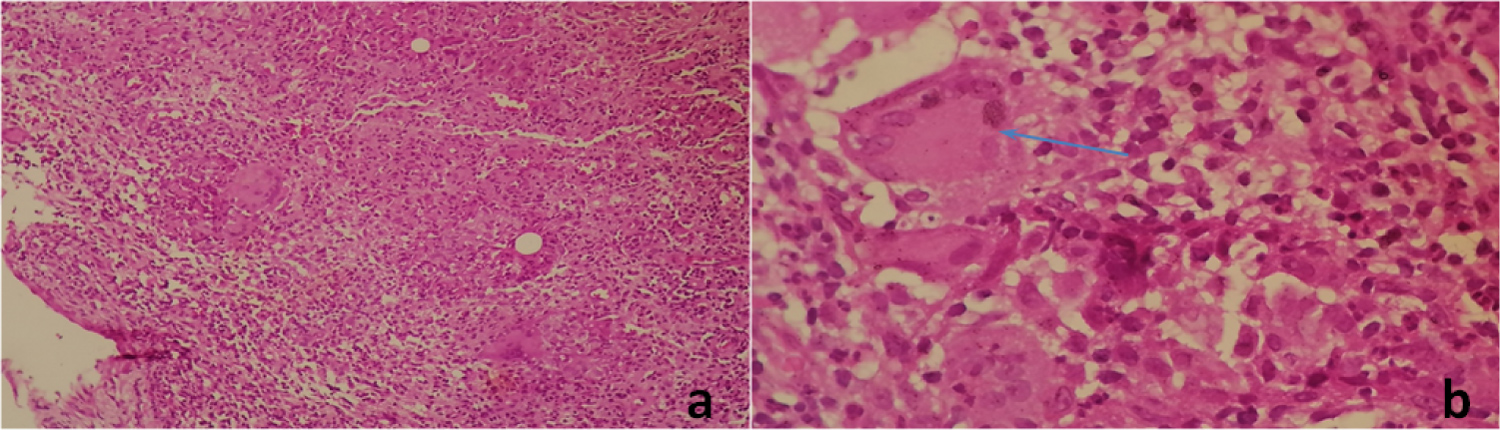 Figure 3: (a) Breast parenchyma with granulomatous inflammation (HE x 100); (b) Epitheliogigantocellular granuloma rich in giant cells (blue arrow) (HE x 400).
View Figure 3
Figure 3: (a) Breast parenchyma with granulomatous inflammation (HE x 100); (b) Epitheliogigantocellular granuloma rich in giant cells (blue arrow) (HE x 400).
View Figure 3
The cytobacteriological study of percutaneous drainage liquid of the abscess under ultrasound guidance showed an important reaction consisting of polymorphonuclear cells. Aerobic and anaerobic cultures were negative.
The KB research in sputum as well as the direct examination of the collected pus was negative for Mycobacterium tuberculosis. The culture of the percutaneous drainage liquide in a Lowenstein-Jensen media was still negative in the third week.
The anatomopathological study and the elimination of other affections that can cause a granulomatous inflammation, allowed to retain the diagnosis of idiopathic granulomatous mastitis associated to erythema nodosum and arthritis. An oral corticotherapy was initiated, based on prednisone at a dose of 1 mg/kg per day; an oral potassium supplementation was prescribed as well. The treatment allowed a quick regression of the symptoms.
However, after 5 weeks of culture on Lowenstein-Jensen medium, colonies of acid-fast bacilli (AFB) started growing at the number of 3, and thanks to differential tests, Mycobacterium tuberculosis was finally identified. The MT was then confirmed based on the positive tuberculosis culture and a positive polymerase chain reaction (PCR) that also affirmed the absence of any mutation encoding for a rifampicin resistance.
The diagnosis was then corrected and the treatment was adjusted by initiating antibacillary treatment including: Isoniazid (H), 5 mg/kg per day, rifampicin (R) 10 mg/kg per day, pyrazinamide (Z) 30 mg/kg per day, ethambutol (E) 20 mg/kg per day. The treatment regimen consisted of: 2 months of quadruple therapy associating RHZE, followed by 4 months of dual therapy associating RH. Corticosteroids were stopped following a rapidly progressive decrease. The evolution was very favorable, the physical and radiological examination were both normal after 6 months with no signs of residual disease.
MT is a chronic granulomatosis due to an infection by Mycobacterium tuberculosis. Since it was described for the first time in 1829 by Sir Astley Cooper as a cold breast tumor or a mammary scrofulous swelling in a young women with a breast tumefaction, about 1000 cases of MT were reported in literature [1,2].
MT comes in last in frequency of visceral locations: it represents 0.06%, and affects essentially women in age of procreation [3]. It's especially found in regions with high tuberculous endemicity, such as sub-saharan Africa, Asia, and North Africa [4]. It represents 0.5 to 4.5% of mammary pathology and its frequency changes depending on geographical regions [2,5,6].
A Moroccan study conducted by Zekri, et al. [7] found out that MT incidence is of 0.4% of all mammary affections compiled in gynaecology and obstetrics department which is a close value to that found in studies conducted in North Africa.
In fact, MT should be distinguished from other mammary affections and especially cancers giving the clinical and radiological similarities. The diagnosis can't be confirmed unless anatomopathological and bacteriological examinations were performed [7]. The main risk factors identified were: multiparity, breastfeeding, mammary trauma and chronic mastitis [6]. MT is called primary when there are no other tuberculosis locations, which is the most frequent case scenario. It is called secondary when it follows other locations [2,5,6,8,9]. The contamination pathways are represented first of all by retrograde lymphatic stream, coming most of times from axillary lymph nodes [8,10]. Hematogenic pathway is rare. The affection by contiguity from a parietal thoracic site defines the tuberculous para-mastitis. Cutaneous or galactophore pathways are possible as well but are very rare [11,12]. In our case, the affection was primary.
The symptoms of mammary tuberculosis can be very insidious and non specific and can usually mimic signs of breast cancer. According to Shinde, et al. [13] a lump in the breast with or without ulceration represents the most frequent representation of MT; the other forms include diffuse nodularity, and multiple sinuses mainly on the upper outer quadrant of the breast. Concomitant axillary lymph nodes can be found in one third of the patients [13,14]. Pal [15] reported that there was a slight tendency to have the right breast to be more affected which was the case for our patient.
Mammography and ultrasounds are useful but not very reliable to differentiate between an MT and breast cancer [4]. Same goes for CT scans and MRI that weren't able to retain the diagnosis without a histological confirmation.
The negative result of the QuantiFERON test doesn't exclude an active infection, the specificity of IGRA blood tests is low for individuals, coming from high endemicity countries, and in whom an active infection is suspected; moreover, IGRA tests are useless to support the diagnosis of active tuberculosis in populations with a high prevalence of latent tuberculosis [16].
Anatomopathological confirmation of MT needs the identification of epithelioid granulomas with caseating necrosis and giant Langhans cells with lymphohistiocytic aggregates. Our patient had a granulomatous lesion of the breast. Granulomatous mastitis is a descriptive non specific term that includes numerous specific lesions such as tuberculosis, fungal infections, sarcoidosis and granulomatous reactions in carcinoma [17].
The first diagnosis we had retained was an idiopathic granulomatous mastitis (IGM) because the histological study found no caseasting necrosis and the KB culture was still negative in the first 3 weeks. The diagnosis of sarcoidosis was also excluded, the classic Lofgren syndrome was incomplete giving that the patient only had erythema nodosum and ankle arthritis, but no mediastinal lymphadenopathies since the chest X-ray was normal; also, biological evidence was lacking (ACE, calcium and phosphates levels were normal). IGM was first described in 1972 [18], of which, tuberculous mastitis should always be considered a differential diagnosis in women with history of tuberculosis contact [19]. It generally affects women in age of procreation. Its cause is unknown, but it could probably be due to a chemical reaction associated to hormonal contraception, or have an autoimmune or infectious cause [20]. This type of exposure happens frequently in endemic countries such as Morocco.
In IGM, the granulomatous inflammatory reaction, consisting of epithelioid and giant cells, is restricted to mammary lobules in which there's also a leukocyte infiltration and formation of an abscess but without caseation [21]. In MT, the granulomes are diffused, aren't limited to the lobules, and are associated to a caseating necrosis.
Bacteriological diagnosis of MT is based on identification of Mycobacterium tuberculosis in the fine needle aspiration sample, in the biopsy or mammary fistulae secretions. The direct examination is unfortunately not very specific or sensitive, especially when it's about extra-pulmonary tuberculosis [22]. The definitive diagnosis then is based on the isolation and identification of the etiological factor. The tuberculous bacillus is only found in 25% of the cases [23,24]. The Löwenstein-Johnson (LJ) medium is the most used culture medium. The culture is slow, it needs about 3 to 4 weeks for Mycobacterium tuberculosis, and 45 to 60 days for Mycobacterium bovis and Mycobacterium africanum. However, sometimes, the duration can go up to 4 to 6 weeks to isolate the KB. Like our patient's case, the culture wasn't positive until the fifth week. The culture is declared positive right after the emergence of bacterial colonies with a characteristic morphology: The colonies are usually eugonic (when separated, the diameter is of 5 to 10 mm), with a dry "cauliflower" verrucous appearance, a cream-beige coloration and are opaque when it's about Mycobacterium tuberculosis [22]. The antibiogram allows us to evaluate the treatment chances of success, usually introduced as a probabilistic treatment for every new patient who has never received any medication [22].
Many other diagnoses must be excluded before retaining the diagnosis of MT. Differential diagnoses include: Fibroadenoma, cancer, ducts ectasia, giant cell reactions to a foreign body with fat necrosis; foreign bodies or an abscess, IGM, sarcoidosis, syphilitic gumma and a granulomatosis with polyangiitis [25,26], all these elements should be excluded using suitable diagnostic tests.
The treatment of mammary tuberculosis is identical to that of other extra-pulmonary locations following the national program of tuberculosis control, and it consists of a first intensive phase associating Rifampicin (R), Isoniazid (H), Pyrazinamide (Z) and Ethambutol (E) during 2 months, followed by a consolidation phase associating Rifampicin (R) and Isoniazid (H) for 4 months: 2RHZE/4RH. The antituberculosis chemotherapy is controlled and administrated mainly on an outpatient basis. Some authors prefer the treatment regimen of 9 months (2 months of RHZE followed by 7 months of RH) since it generally lowers the relapse rate. However, in some series, this therapy was administrated differently. For instance, Khanna, et al. [2] have treated 52 patients who had mammary tuberculosis for an average period of 9 months and have extended the duration to 12-18 months for 18 patients. In a study of Harris, et al. [27], one third of the patients have received a treatment for 9 months. But on a study of Silva, et al. [28], a 6 months treatment period was sufficient for patients to recover.
Before retaining the diagnosis of MT, our patient was put under corticotherapy giving the IGM diagnosis for 15 days and the evolution was spectacular during this period. We've introduced antibacillary treatment right after the bacteriological confirmation of MT. Corticosteroids were then progressively stopped over a period of 2 months. We thought after observing this case that this association really sped up the healing process of our patient.
We all know that every inflammatory reaction to Mycobacterium tuberculosis can cause tissue damage, necrosis, can even cause an organic dysfunction [39] due to the edema. Corticosteroids have been used to counter these inflammatory reactions. But, at the same time, they have an immunosuppressive effect, so the treatment using corticosteroids can facilitate the infection by Mycobacterium tuberculosis or reactivate a latent or a previous infection. Through literature, effects of corticosteroids on tuberculosis in patients treated by anti bacillary treatments are generally benefic, but the benefits are varying [30,31]. The use of corticosteroids on patients with tuberculosis is a very controversial topic. They have been used for so long for all forms of tuberculosis. However, their effects and advantages in different tuberculosis forms are very fluctuating and are entirely specific to the organ affected [32]. Admittedly, we haven't found in literature any paper discussing the relevance of corticosteroids as an adjuvant therapy of mammary tuberculosis. But, the very favorable evolution of this case made us wonder that this non programmed association was actually benefic.
Surgery can be performed for diagnostic and therapeutic purpose: Draining of a fistulized lesion to shorten the evolution, surgical removal after treatment failure or recurrence of the mammary mass, or a cleanup mastectomy for extensive and/or fistulized lesions resistant to medical treatment.
We're not wrong to call it « the big simulator », MT is still a rare affection even in endemic countries. It needs a high level of clinical suspicion and a good expertise in clinical and radiological examination in order to establish an early diagnosis. The benefit of this clinical case is to always remember to take into account tuberculous mastitis, when discussing differential diagnosis of cancer and granulomatous mastitis especially in endemic areas. The diagnosis is based on anatomopathological and bacteriological examination.
The treatment includes a minimum of 6 months of antibacillary medication and surgical intervention when indicated. And in light of some extra-pulmonary tuberculosis locations, we believe that corticotherapy used as an adjuvant therapy can improve the healing process, but it still needs to be confirmed by studies.
Mammary tuberculosis is an affection with a very good prognosis but only when its treatment is well adapted and followed up.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
This case report was written based on clinical observation without any funding.
No potential conflict of interest relevant to this article was reported.
E.K.I appointed topic, wrote and revised the manuscript. K.A was responsible for the analysis and the interpretation of the pathology. T.Z was responsible for the analysis and the interpretation of the MRI. Z.M, S.N and B.A. determined and adjusted the topic, concept and drafting of the manuscript. R.A and S.Y. involved in critically revising the final preparation.