COVID-19, short for coronavirus disease 2019 is responsible for causing coronavirus disease that has been declared as a pandemic. On 30th January it was declared as the worldwide emergency crisis. It is very similar to its previous strain SARS-CoV that was known to cause an outbreak in 2002. Another strain MERS-CoV was first identified in Saudi Arabia in 2012. COVID-19 is first identified in Wuhan, China then it spread to multiple countries and become a significant danger for the globe. On 26th February 2020, the first case of coronavirus emerges in Pakistan. The predominant symptoms of this viral illness are fever and cough, but there is a range of symptoms, while some patients may be asymptomatic.
This study aims to evaluate the awareness of the population regarding this deadly virus. To understand the public behavior, beliefs, their understanding regarding precautionary practice, their indulgent about the situation, and their attitude towards the pandemic.
A cross-sectional online survey was conducted from 31st March to 6th April 2020. Our study target residents of Karachi Pakistan, who were 18 or above, could read and understand English and had filled the complete questionnaire. The sample size was calculated using www.openepi.com with a confidence interval of 95% and absolute precision of 5%. Data was collected by a self-designed online questionnaire, consisting of 38 closed-ended multiple-choice questions. The questionnaire was divided into two sections 1) Demographic section 2) Knowledge, Attitude, and Practices (KAP) related questions. A pilot study was conducted to validate the questionnaire. Data was analyzed by Software Statistical Package for Social Sciences (SPSS) version 21.0.
A total of 330 participants were included in the study, out of which 184 females (55.8%) and 146 males (44.2%). The maximum number of the participants (326; 98.8%) were aware regarding the origin of coronavirus disease, almost (326; 98.8%) participants agreed to the fact that COVID-19 is contagious and can be transmitted. Respiratory droplets (287, 87%) was considered as the most common route of transmission. An enormous amount of participants (318, 96.4%), knew that lungs are the major body part affected by COVID-19. Almost all (326, 98.7%) of our participants are practicing social distancing.
Participants from Karachi have an overall reasonable knowledge regarding the COVID-19. But still, further awareness is needed to improve the condition and to stop the spread of the virus. Virtual awareness sessions should be arranged to provide maximum information to the public regarding handwashing steps, and to maintain a hygienic environment as well as encourage them to practice social distancing and avoid social gatherings.
COVID-19, Coronavirus disease, Pandemic, A global emergency
Corona Virus Disease-2019 or COVID-19, which primarily affects the respiratory system was first identified after an epidemic of pneumonia in Wuhan, China in December 2019 [1]. This disease is caused by the virus named SARS-CoV-2 [2], a member of the Coronaviridae family and it shares great similarity with SARS-CoV that was known to cause an outbreak of Severe Acute Respiratory Syndrome in China in 2002 [3]. Another member of this family, MERS-CoV caused a pandemic of Middle East Respiratory Syndrome in 2012, being first identified in Saudi Arabia [4]. Early reports link the origin of SARS-CoV-2 to the animal market in Wuhan, where it possibly emerged from bats [5,6], since this virus falls in the beta-coronavirus genus [6], one of the two genera of Cornonaviruses which can infect mammals [7]. From Wuhan, the virus continued to spread in other parts of the country, which confirmed its person to person transmission [8]. The predominant symptoms of this viral illness are fever and cough, but there is a range of symptoms, while some patients may be asymptomatic [8].
Soon after its emergence in China, COVID-19 spread to numerous countries and was declared a pandemic by WHO in January 2020 that posed a significant danger to global health [9]. A large number of cases are emerging globally; as of April 28th, there are 2,954,222 cases of infection worldwide with 202,597 total deaths [10]. The rapid expansion of the virus has put health-care, economic, and social systems under great pressure throughout the world. Data from International Labour Organization (ILO) shows that there has been a 5.4% loss of global working hours in the initial months of 2020 and this reduction is likely to continue for the rest of the year [11]. The global economy is in crisis as COVID-19 shuts down the world [12], whereas the healthcare system, which is already overwhelmed with the growing number of cases, faces a shortage of personal protective equipments [13] and ventilators [14]. More and more countries are falling prey to this virus. The affected countries are developing strategies at national, local, and state levels to combat the growing Coronavirus crisis and to ensure a pragmatic response from the public during this critical time, which would help in the prevention and control of the virus spread.
The first case of this disease in Karachi, which was also the first case in Pakistan, reached through Iran on 26th February 2020 [15]. With limited healthcare resources in hand, the country needed to take quick and adequate steps to contain the spread of the virus and minimize the chances of a vast number of possible casualties. This virus rapidly transmits from human to human via respiratory droplets [16] so to lower the transmission rates, limiting close contacts among people became the principal step. This could include restricting social mixing and gatherings, closing all public places, and avoiding crowded areas. Pakistan, in its attempt to deal with the outbreak, decided to impose lockdown in its major provinces, with the suspension of all the flights and sealing of the borders with Iran and Afghanistan. Currently, the country's main provinces are still under lockdown and except for few special flights for bringing stuck Pakistanis home, the rest are still closed. At present, no vaccine is available against the virus globally and potential treatment options are still being explored and tested [17]. This means that the control of disease primarily depends upon preventive measures. The cases of COVID-19 and death toll in Pakistan continue to rise; according to WHO situation report of April 28th, the total confirmed cases in Pakistan are 13,915 and total deaths are 292 [10], whereas Province Sindh which includes the big city Karachi is heavily affected with several cases and deaths 5,291 and 92 respectively [18]. Therefore, strictly adopting prevention measures including the practice of social distancing, maintaining personal hygiene, and following stay-at-home orders [19] is of immense importance to keep the virus transmission rate as low as possible and thus reduce the burden on the healthcare system. How well the public abides by these instructions depends on their knowledge and perceptions about this problem [20]. During pandemics or at times of emergency, it is not uncommon to see misinformation and false theories spreading among the public which add to their fears and lead them into wrong practices. Inadequate knowledge hampers their understanding of the nature of the disease-causing them to seek help late [21]. Thus, identifying the misconceptions at the right time would aid in correcting the beliefs of citizens and their attitude towards this pandemic. And all these measures can reduce the magnitude of the epidemic in the country.
We conducted this online questionnaire-based study aiming to assess the level of awareness regarding COVID-19 among the people of Karachi, the beliefs that make them follow or abandon any precautionary practice, their understanding of the situation, their attitude towards the pandemic, the prevailing misconceptions and the ongoing practices. This KAP study would help to evaluate the preparedness of population and most importantly its findings would help to understand what particular areas of public behavior need attention, which in turn would help in setting priorities in information dissemination and would also help in creating a better national response during our fight against this highly contagious disease.
A cross-sectional online survey was conducted from 31st March to 6th April 2020, two weeks after the lockdown was announced in Karachi, Pakistan in context to the COVID-19 outbreak. Taking into consideration the current situation of the country, it was practically unachievable to conduct an inter-city face to face community-based survey; therefore data was collected using an online Google form. Our study included residents of Karachi Pakistan, who were of 18 age and above, who could read and understand English and had filled the complete questionnaire. Whereas, Healthcare officials, dentists, paramedics and all the persons related to medical background were excluded from this study, as this research was solely meant to assess the level of awareness about COVID-19 among the general population (i.e people who belong to non-medical background living in a particular place at a specific time) of Karachi, Pakistan. In addition to that people not having internet access for Google form were also excluded. Furthermore, ethics approval for this specific study was not required.
The sample size was calculated using www.openepi.com [22], keeping the anticipated frequency of 70.4%, in a view of a study done in Saudia Arabia which estimated that 70.4% of participants felt at risk of contracting the MERS-CoV infection at work [23]. A confidence interval of 95% and absolute precision of 5% gave the total sample size of 330.
During the study period, the participants were enrolled based on convenient sampling. Voluntary participation with informed consent was appreciated and those unwilling to take part were excluded from the study. Moreover, to ensure participant's privacy data was collected anonymously and complete confidentiality was assured.
A Self-administered validated online questionnaire was designed, consisting of 38 closed-ended multiple-choice questions in the English Language. The questionnaire was classified into two sections: A) demographics related questions that were queried by the following variables (gender, age, and qualification) and B) Knowledge, Attitude and Practices (KAP) related questions. To assess the validity of the questionnaire, an online pilot study was conducted on 20 participants and their feedback was used to modify the questionnaire accordingly.
Twenty-one Knowledge questions were generated which were about general COVID-19 virus characteristics, its transmission, risk factors, symptoms, and its related treatment and precautionary modalities.
Attitude and practices towards COVID prevention were assessed by participants' responses about COVID-19 spread in Pakistan and their agreement to wear masks while going outside, practicing social distancing, and washing hands after every activity. Finally, their mental state, behavior, and routine activities during the outbreak were determined via a set of questions along with their viewpoint on government policies and the healthcare system.
All the collected data was entered and statically analyzed by Software Statistical Package for Social Sciences (SPSS) version 21 using mean and standard deviations. Frequencies and proportions of the categorical variable were computed to present the data in a tabulated form. The Chi-Square test was used to assess associations between categorical variables and the Mann-Whitney U test was used to compare numerical variables with Statistical significance set at p < 0.05 (Table 1).
Table 1: Demographic characteristics of participants. View Table 1
A survey was conducted among the general population of Karachi, Pakistan, with a sample size of 330 consisting of 184 females (55.8%) and 146 males (44.2%). Participants were mostly Young adults from the age group 18-29 years (257, 77.87%), with the highest proportion of them were either doing their bachelor's (110, 33.33%) or were post-graduates (150, 45.45%).
The overall description of knowledge, attitudes, and practices regarding COVID-19 is given in Table 2, Table 3 and Table 4 according to gender, age, and level of education respectively. The utmost of the participants (326; 98.8%) were aware that COVID-19 is a Viral disease and most of them (326; 98.8%) agreed to the fact that COVID-19 can be transmitted from an infected person to a non-infected one regardless of their age, gender or qualifications. The majority of them reported accurate information about its mode of transmission; that is Respiratory droplets (287, 87%), whereas the fecal-oral route (83, 25.2%) was the second most common answer among all. 223 of them (67.6%), agreed that a COVID-19 positive asymptomatic person can transmit the infection while many females (57, 31%) and young adults (66, 25.68%) disagreed with this statement (Table 2 and Table 3 respectively). As stated by most of the participants (318, 96.4%), Lungs are the major body part affected by COVID-19, while referring to age groups, (81, 31.51%) of young adults have still no idea about it irrespective of their education (Table 2 and Table 3). Dry cough (278, 83.6%), shortness of breath (272, 82.4%), fever (275, 83.3%) were majorly selected symptoms of the COVID-19. Whereas, only (36, 24%) post-graduate knew that all of the given symptoms; dry cough, shortness of breath, fever, headache, body ache, body rash, sneezing, conjunctivitis, and sore throat were the manifestation of COVID-19 (Table 4). Furthermore, out of 350 participants; (177, 53.6%) with the highest percentage of among old adults (12, 92.3%) thought that the incubation period lasted for 2 weeks whereas (112, 33.9%) consisting of (87, 33.85%) young adults and (24, 40%) of middle-age adults were confused between 2-3 weeks.
Table 2: Knowledge, Attitude and practices regarding COVID-19 in relation to gender. View Table 2
Table 3: Knowledge, Attitudes and practices regarding COVID-19 related to Age groups. View Table 3
Table 4: Knowledge, Attitudes and practices regarding COVID-19 related to educational levels. View Table 4
Out of 330 participants, (209, 63.33%) opted Elderly group for being at the highest risk of getting COVID-19, whereas in regards of education, (48, 32%) post-graduates and (45, 40.9%) participants doing their bachelors selected all; elderly, women and children, to be vulnerable to COVID-19. The masses (305, 92.4%), acknowledged that infected patients should be kept in isolation while few of them (25, 7.6%) out of which more males (16, 11%) than females (9, 4.9%) believe that this decision should depend upon the severity of the symptoms (Table 2). Regarding the precautionary measures, a larger number of people (294, 89.1%) anticipate that all; washing hands regularly, wearing the mask during sickness and social distancing are the precautionary measures needed against the virus no matter what the age, gender or education qualification was. The majority of participants (267, 80.9%) had doubts about antibiotics being the treatment of choice. Most commonly marked pre-disposing factor was asthma (141, 42.7%), followed by smoking (115, 34.8%), then diabetes (49, 14.8%) and lastly hypertension (40, 12.1%). While (97, 29.4%) believed all of the above mentioned, were the risk factors for COVID-19.
The participants were asked about their attitudes and practices regarding the Viral disease. Irrespective of the level of education, age, or gender; social media (210; 63.6%) was the most common source of getting information, followed by television (71, 21.5%), healthcare official (26, 7.9%) and lastly, research articles (23, 7%).
Most of the male (118, 80.8%) and females (157, 85.3%) participants chose to wash their hands after every activity (Table 2) while a majority of the middle-age (41, 68.3%) and old-age adults (11, 84.6%) tend to take food supplements to boost their immunity (Table 2). Almost all (326, 98.7%) of our participants are practicing social distancing, whereas (305, 92.42) tend to wear a mask if going outside while being sick. Most of the females (120, 65.2%) are satisfied with measures taken by the government in response to the COVID-19 outbreak in comparison to less than half of the men (67, 45.9%) are satisfied only (Table 2). Moreover, when investigated about their behavioral change during this pandemic and lockdown period majority of the participants (180, 54.5%) assured that they have become more health and hygiene conscious, while a similar number of individuals (150, 45.4%) were also becoming more isolated and depressed during world COVID-19 pandemic (Figure 1).
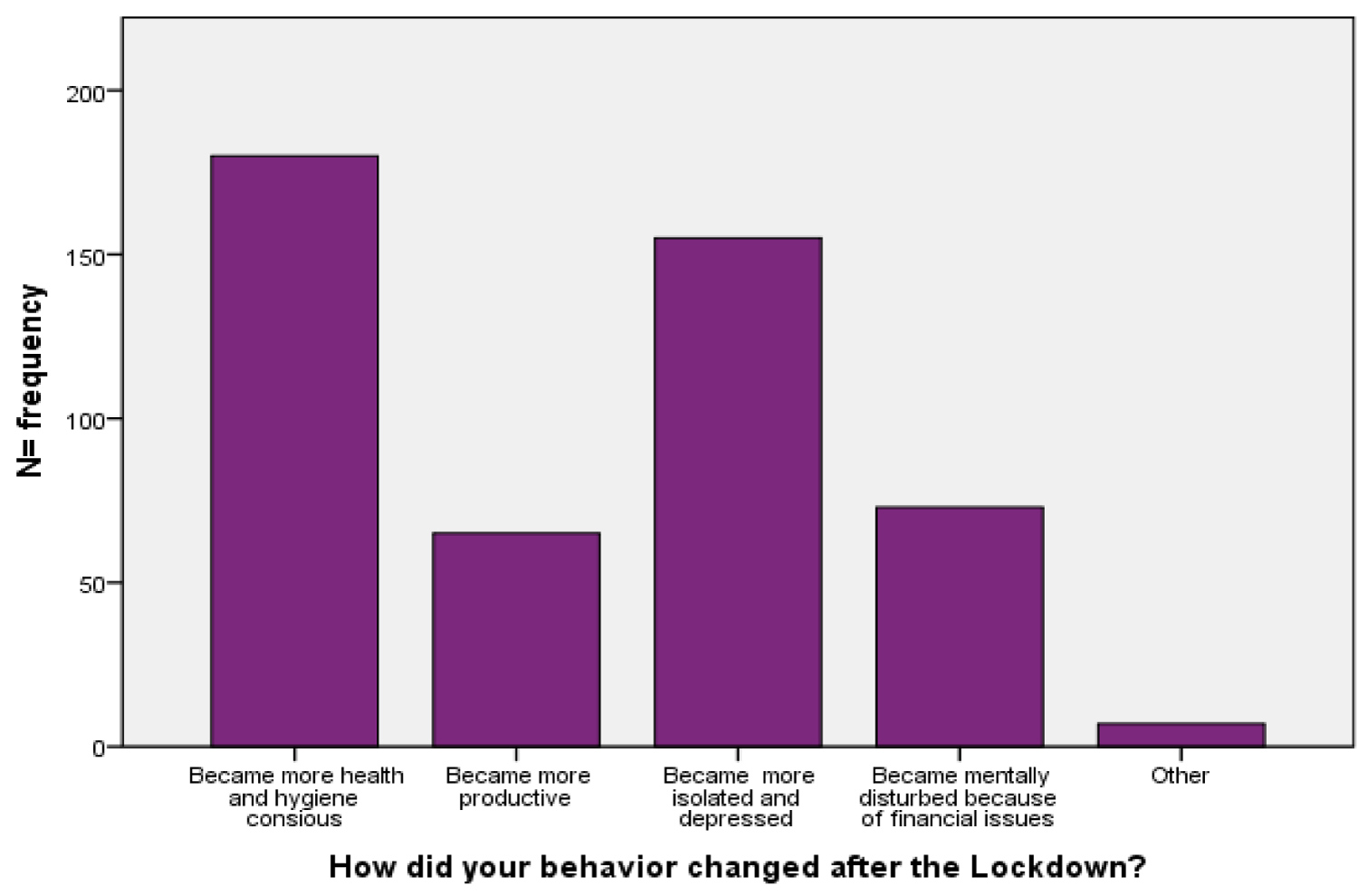 Figure 1: Behavioral changes during the Lockdown period.
View Figure 1
Figure 1: Behavioral changes during the Lockdown period.
View Figure 1
Despite an extensive literature review and to the best of our knowledge, this is the first study attempting to evaluate the knowledge attitude and practices among the general population in Karachi. As reported in a study published in the British Medical Journal in 2009 during the Swine Flu epidemic, if people have basic knowledge about the modes of transmission and the availability of vaccines, they respond appropriately during an outbreak [24]. Therefore, the authors aimed to assess the baseline awareness of the respondents along with their major self-reported sources of knowledge and their corresponding habits and influencing practices. These will help guide clinicians and policymakers to pinpoint gaps in Knowledge and identify areas where public health interventions may be targeted and patients may be educated.
The majority of our study participants, which consisted mostly of a younger age group, correctly identified the epidemiological and clinical factors related to COVID-19 with a vast majority (271 out of 330 or 82%) of subjects falling in the adequate knowledge to high knowledge bracket. These findings are similar to a study carried out by Bao-Liang Zhong, et al. where approximately 90% of the residents surveyed in an online knowledge questionnaire displayed correct answers [20]. Geltzer P, et al. found similar results during an online survey aiming to assess the KAP among participants in the United States and the United Kingdom [25]. These can also be attributed to our study population where a majority (78.8%) of our respondents' educational status was either being enrolled in a bachelor's program or higher. These findings are also not entirely unexpected considering this epidemiological survey was carried out during the exponential spread of cases in Pakistan [18], the strict lockdown in place throughout the city during this public health crisis and the overwhelming coverage dedicated to this novel disease in social media such as Facebook and Twitter, etc., television news channels and official government announcements. Because of the above factors, these subjects would have easily available access to these sources and would then be informed readily.
A study carried out by Abdallah Y Naser, et al., assessing the KAP among respondents in three Middle Eastern countries reported the mean overall knowledge score to be 66.1% [26]. This is lower than the mean knowledge score calculated among our respondents which are around 72.6%. Factors that might be responsible for the greater knowledge score in the current study can probably be attributed to early public health intervention by Local government where educational institutions were closed on February 27th, 2020 when there were only 4 confirmed cases of COVID-19 in Pakistan. This proactive step may have inspired the community to get better acquainted with the epidemiological and clinical aspects of COVID-19.
A vast majority of study participants (281 out of 330 or 85.2%) had reported that social media such as Facebook, WhatsApp, Twitter, etc. and Television to be the most common sources of acquiring information regarding this disease. While this pandemic is given global coverage in these mediums, there is minimal fact-checking, source verification, and a plethora of misinformation that is readily circulated on these platforms. Such examples would include holding your breath for 10 seconds, drinking plenty of warm water, rinsing the nose with saline, using antibiotics to treat this viral illness, etc [27]. These concerns were echoed in the KAP study by Geltzer P. where a substantial portion of those surveyed had misleading knowledge regarding this disease and planned to discriminate among people of East Asian ethnicity on these unfounded bases [25]. Some of our respondents had similar misconceptions with 19% or 63 out of 330 participants having the belief that antibiotics can be used to cure this disease. We would encourage the fact-checking of all information disseminated to help curb this menace. The prevalent misconceptions can be a potential topic for further subsequent studies.
Considering the bleak headlines perpetuated by this pandemic, it was heartening to note that a vast majority of respondents (77.3%) were optimistic about the possibility of Pakistan winning its battle against COVID19. These were however lower than the subjects in the study by Zhong, et al. where 97.3% expressed similar sentiment [20]. About 18.8% were unsure of the outcome. Factors that can be attributed to these are the relatively lower contentment in government measures with only 56.7% of the subjects in our study feeling satisfied with measures introduced by the local and provincial governments. These discontentments can be chalked up to various reasons such as the poor public health infrastructure in Pakistan and the abysmal rate of doctors, nurses, and beds per population in Karachi [28].
It has been reported in various studies that during epidemics, the total number of people affected by the epidemic is lower than the number of people whose mental health is disturbed and these can lead to multiple negative consequences which can far outlast the initial epidemic [29]. Our survey touched upon this aspect where 32.3% of the respondents felt isolated and depressed and 15.2% felt mentally stressed due to financial difficulties as a consequence of the lockdown. In Pakistan with an already poor health infrastructure, there is no doubt that a sizeable majority of the population will be feeling the negative psychological impacts of the lockdown, closure of economic activity, and uncertainty about what the future holds. As such we would propose that this aspect be investigated separately and urgent measures are taken to mitigate it. Effective strategies have been published in the British Journal of Psychiatry by Omell F, et al. [30] and these can provide a framework for clinicians to educate patients to cope with the mental stresses of this pandemic more accurately.
As of yet, there is no vaccine or prophylactic medicine that can help prevent this viral illness [17]. Hence, The Government of Pakistan in collaboration with the Ministry of Health has published important guidelines for the public to follow including avoiding crowded places also known as social distancing, wearing masks going outside if available, washing hands regularly for at least 20 seconds, seeking regular medical care, etc [31]. Our study results showed that a vast majority of respondents were adhering to these guidelines with 98.8% practicing social distancing, 92.4% wearing masks when going outside and 83.3% washing hands regularly.
These results are similar to the survey carried out by Geltzer P. in the US and UK where 92.6% and 86% of the public were following these preventive methods and to the KAP study carried out by Zhong, et al. were approximately 95-96% were avoiding crowded places and 97% were wearing a mask when going outside. These results can be attributed to the high rates of knowledge regarding the disease. Also responsible can be the wide-ranging nature of these pandemic and similar social conditions in all these countries at the time of the study with the suspension of commercial and economic activity and a general lockdown in place.
Physicians can incorporate questions about these behaviors in their evaluation and history taking of a patient and can likely predict if the patient is at high risk of being infected. Standardized questionnaires can be made and administered at the first point of contact of a patient with a healthcare facility and then stratified accordingly to minimize further transmission.
Of note is the fact that our results showed a significant statistical difference in the practice of wearing masks and practicing social distancing among males and females with p values of 0.013 and 0.02 respectively with a higher number of males likely to practice these habits. These findings surprisingly digress from the findings of the KAP study by Zhong, et al. and previous studies which suggest that male gender is more likely to engage in risk-seeking behaviors and hence are likely to contract COVID-19 [20,32]. These findings can be attributed to the fact that disproportionately more males have died from COVID-19 than females [33]. The smaller sample size of our subjects may also have been a contributor.
This study has some limitations. This was an online survey with a convenient sample of mostly young aged students. Vulnerable communities mostly the elderly, homeless, and illiterate population was not represented in this survey. This limited the reach of this survey and hence is probably not representative of the general population. It might have led to an overestimation of knowledge and underestimation of preventive practices among the general public. Hence, a KAP study dedicated to these segments of the society may yield a clearer picture of the attributes which the authors have attempted to describe in this study. It is also possible that some respondents may have randomly picked out the answer choices in the shortest possible time to complete the survey as soon as possible or that they may have looked up the answers to the questions while filling out the forms. Our analysis did not account for these and they may have interfered with the results.
Secondly, economic factors may have an impact on the attitudes and practices of the respondents. These were not taken into account in our data collection. Another limitation is the subjective and unstandardized assessment of the practices of respondents towards COVID-19 which was assessed using a handful of questions only. These practices should be ideally assessed using in-depth interviews and expert opinions standardized to ensure validity.
The strength of our study lies in the fact that this provides a "real-time" assessment of the knowledge attitudes and practices of a segment of the general population during this critical period when it is needed. Hence, further studies can use this as a baseline and extrapolate from this data, and Government and Non-government entities can plan public health strategies on this basis and clinicians can stratify risky patients reporting to their clinics based on their preventive practices.
In summary, it can be said that young aged students in Karachi have an overall adequate knowledge regarding the epidemiological and clinical features of COVID-19. The majority of them have a positive attitude and are adequately following the practical measures to prevent its spread while being optimistic about the future course of this pandemic in our country.