Klebsiella pneumoniae invasive syndrome (KPIS) is a life-threatening condition with rising incidence across the globe. It is characterized by a monobacterial primary pyogenic liver abscess with or without additional dissemination. Some of the possible metastatic complications include endophthalmitis, lung nodules, meningitis, and potentially inflammation of any organ. Despite the wide distribution of common K. pneumoniae, invasive syndrome is often overlooked due to low incidence of hypervirulent strains, which usually affect immunocompetent or diabetic, young individuals from Asian descent without any underlying biliary or abdominal pathology. In this article we present an unusual case of a 53-year-old Hispanic male in South Florida, USA who presented with acute onset of shortness of breath, fever, and diarrhea. His workup revealed a monobacterial K. pneumoniae pyogenic liver abscess complicated with bacteremia and septic pulmonary nodules. This presentation is highly suggestive of K. pneumoniae invasive syndrome. The abscess was inaccessible for drainage but it was successfully treated with a 4-week course of ceftriaxone and a complete recovery was documented. Awareness of K. pneumoniae invasive syndrome is paramount, as its presentation can be atypical or can be mistaken with other infections or malignancies. Early recognition is expected to reduce mortality and other complications, particularly when involving multiple organs and systems.
Klebsiella pneumoniae, Hypervirulent, Liver abscess, Lung nodules, Sepsis
Klebsiella pneumoniae is a gram-negative, non-motile, capsulated bacillus [1] from the Enterobacteriaceae family. It is a common cause of respiratory and urinary tract disease in the nosocomial setting and in immunocompromised patients [2,3]. However, in the past decades the emergence of hypervirulent K. pneumoniae (hvKp) isolates has been concerning due to its life-threatening presentation and worldwide dissemination. As opposed to conventional K. pneumoniae (cKp), hvKp strains are frequently community-acquired [4] and occur in immunocompetent, middle-aged individuals often from Asian descent [5], although there have been a few reports of this strain among other ethnicities. These strains produce a syndrome characterized by a primary pyogenic liver abscess with or without additional metastatic complications like endophthalmitis, lung nodules and meningitis.
We present a case of a 53-year-old Hispanic male in South Florida, USA, with a clinical presentation suggestive of K. pneumoniae invasive syndrome (KPIS), complicated with septic pulmonary metastasis. We hope this article assists clinicians in their decision-making process and allows them to sooner consider this clinical entity as part of their differential diagnosis, since it can mimic other infections or malignancies. An additional review was performed to complement our case presentation.
A 53-year-old otherwise healthy Hispanic male from Colombia arrived at the emergency department presenting a 3 day history of progressive shortness of breath, non-productive cough, subjective fever, nausea, vomiting, and watery diarrhea, initially treated at another center with amoxicillin/clavulanate with no improvement. Past medical history includes diverticulosis and polypectomy 3 years prior (unavailable histology). The patient is married and sexually active with male partner. Reports occasional marijuana use, but no pets or recent travel. On admission, physical examination was remarkable for tachycardia (135 bpm), fever (T-max 102.7 °F), pulse oximetry 95% on room air, bilateral decrease in breath sounds, and mild tenderness to deep palpation in left lower quadrant (LLQ). No guarding or rebound. Laboratories: Hemoglobin (13.3 g/dL); WBC (3,200/μl); lymphopenia (6%); thrombocytopenia (67,000/μl); hyperglycemia (171 mg/dL); lactate (1.93 mmol/L); procalcitonin (4.39 ng/mL); urinalysis showed sub-nephrotic range proteinuria (500 mg/dL). HIV, Influenza A & B, Mycoplasma, Legionella, stool studies were negative. On imaging, chest X-ray showed infiltrates in left mid-lung and right perihilar marks. He was admitted in the context of a sepsis and community-acquired pneumonia and was treated empirically with ceftriaxone and oral azithromycin. Abdominal ultrasound showed right liver lobe with heterogeneous mass (up to 2.3 cm) and CT chest confirmed bilateral pulmonary nodules with ground-glass opacities, mediastinal lymphadenopathy, and bilateral pleural effusion (Figure 1). TTE and CT brain scan were normal. Empiric antibiotics were later switched to cefepime.
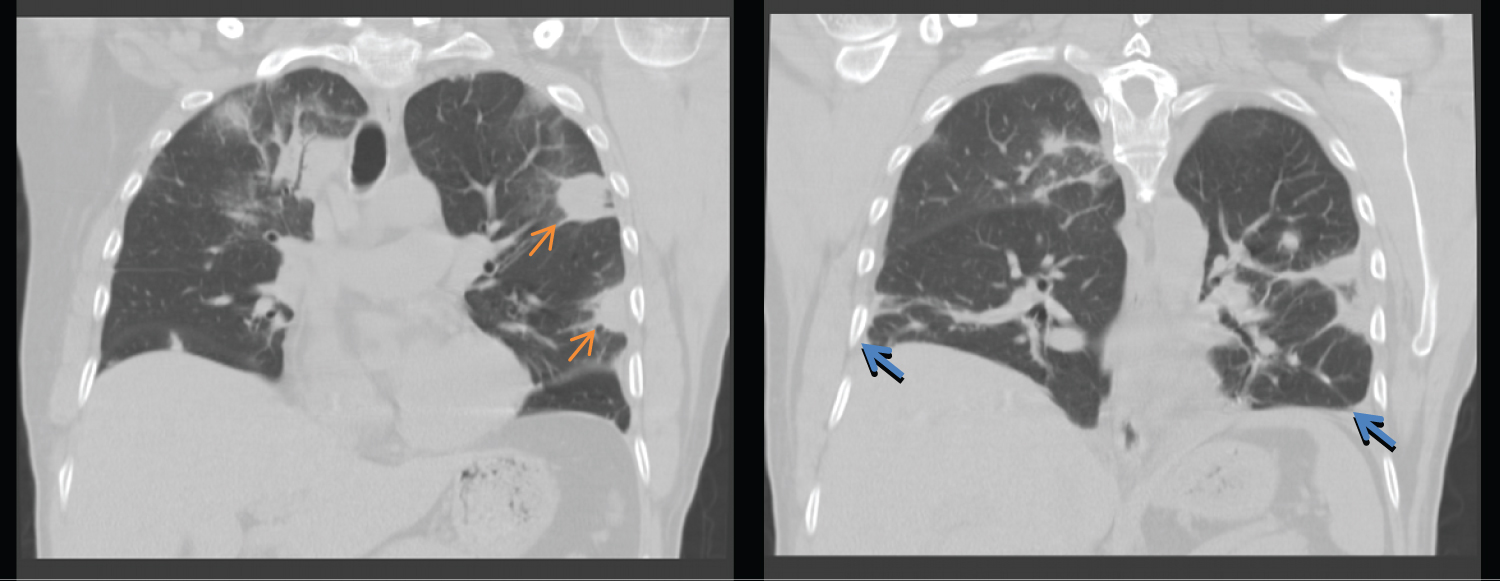 Figure 1: CT chest without contrast. Multiple bilateral pulmonary nodules with hazy surrounding ground-glass opacities (orange arrows) and pleural effusions bilaterally (blue arrows).
View Figure 1
Figure 1: CT chest without contrast. Multiple bilateral pulmonary nodules with hazy surrounding ground-glass opacities (orange arrows) and pleural effusions bilaterally (blue arrows).
View Figure 1
On day 3, blood cultures grew pan-susceptible K. pneumoniae. Patient was hospitalized for 9 days and workup included a CT-guided liver biopsy, also positive for pan-susceptible K. pneumoniae (culture susceptibilities in Table 1) and atypical glands with necrosis and acute inflammatory exudate. Because of multilocularity and location, a decision was made not to perform percutaneous drainage (Figure 2). Genomic testing was not available at our institution, but the clinical course was highly suggestive of KPIS and therefore it was decided to continue treatment for this entity.
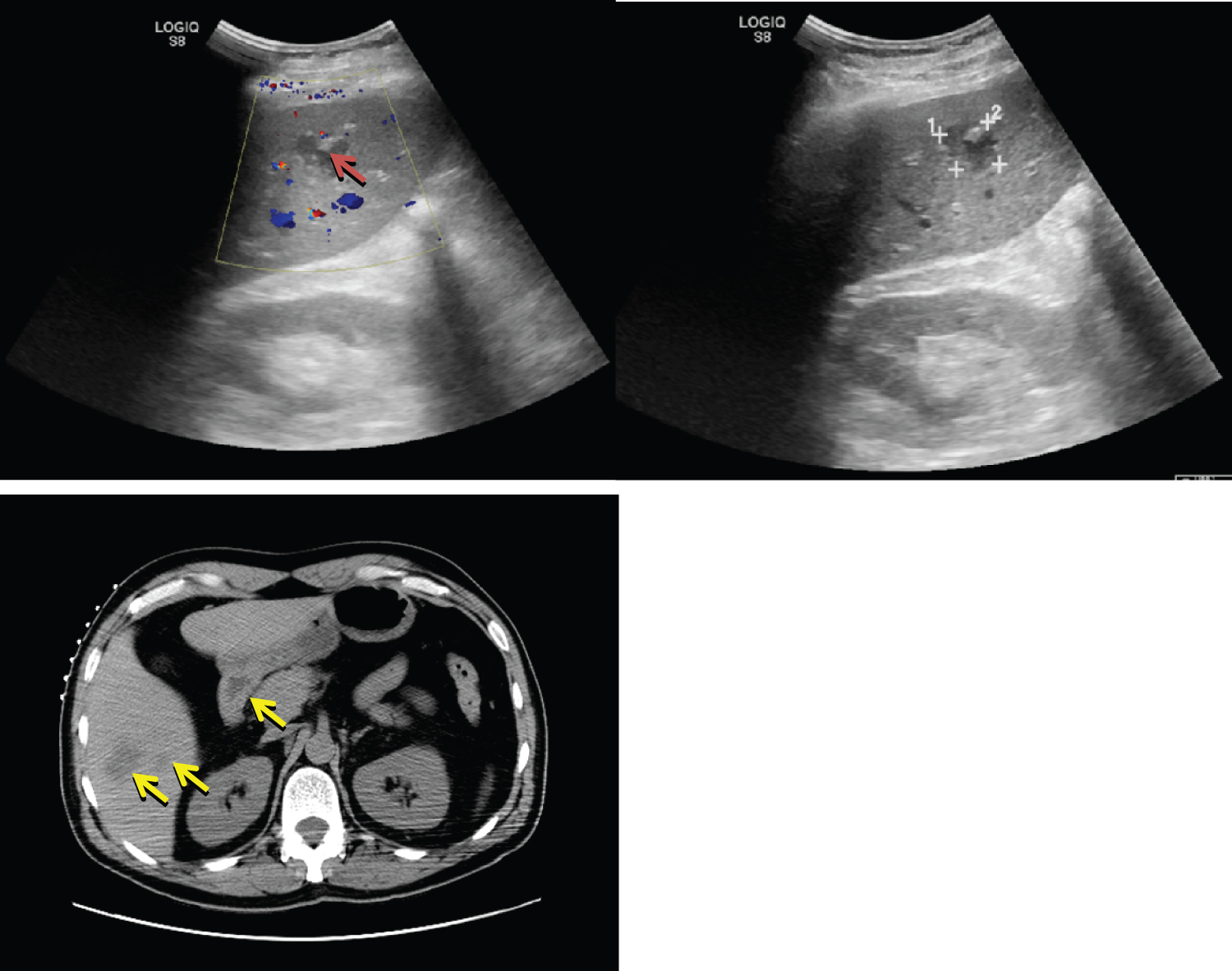 Figure 2: Abdominal ultrasound & CT abdomen with contrast. Several cystic liver masses, largest measuring 3.6 cm on CT (yellow arrows), and 2.3 cm on ultrasound (red arrow).
View Figure 2
Figure 2: Abdominal ultrasound & CT abdomen with contrast. Several cystic liver masses, largest measuring 3.6 cm on CT (yellow arrows), and 2.3 cm on ultrasound (red arrow).
View Figure 2
Table 1: Liver biopsy culture and susceptibilities. View Table 1
Despite his initial convoluted presentation, the patient continued to improve from a clinical and paraclinical standpoint and was discharged with a Peripheral Inserted Central Catheter (PICC). Cefepime was discontinued - after 9 days as inpatient- and Ceftriaxone was scheduled for 4 weeks in total as an outpatient. One month after discharge, he was seen at the infectious disease clinic for follow up where he continued to show persistent clinical and radiologic improvement as per CT chest, abdomen and pelvis.
K. pneumoniae is commonly found in the nosocomial setting and in immunocompromised hosts. However, a new community-acquired and hypervirulent strain was reported in Taiwan in 1986. Since then, it has been recognized globally as a cause of a life-threatening infection in immunocompetent or diabetic hosts [1,6].
Although there is no established definition of KPIS [7,8], it is classically described as a clinical syndrome characterized by a monomicrobial pyogenic liver abscess with or without extrahepatic seeding in the absence of previous biliary disease, intra-abdominal infection or recent intra-abdominal surgery [9,10]. The pathogen's source is generally the gastrointestinal tract and is acquired through fecal-oral transmission [11,12]. After colonization, enteric bacteria are believed to translocate through the portal venous circulation [10] into the liver. Intestinal colonization may serve as a reservoir for pathogenic strains although evidence can be discordant [13,14] (Figure 3).
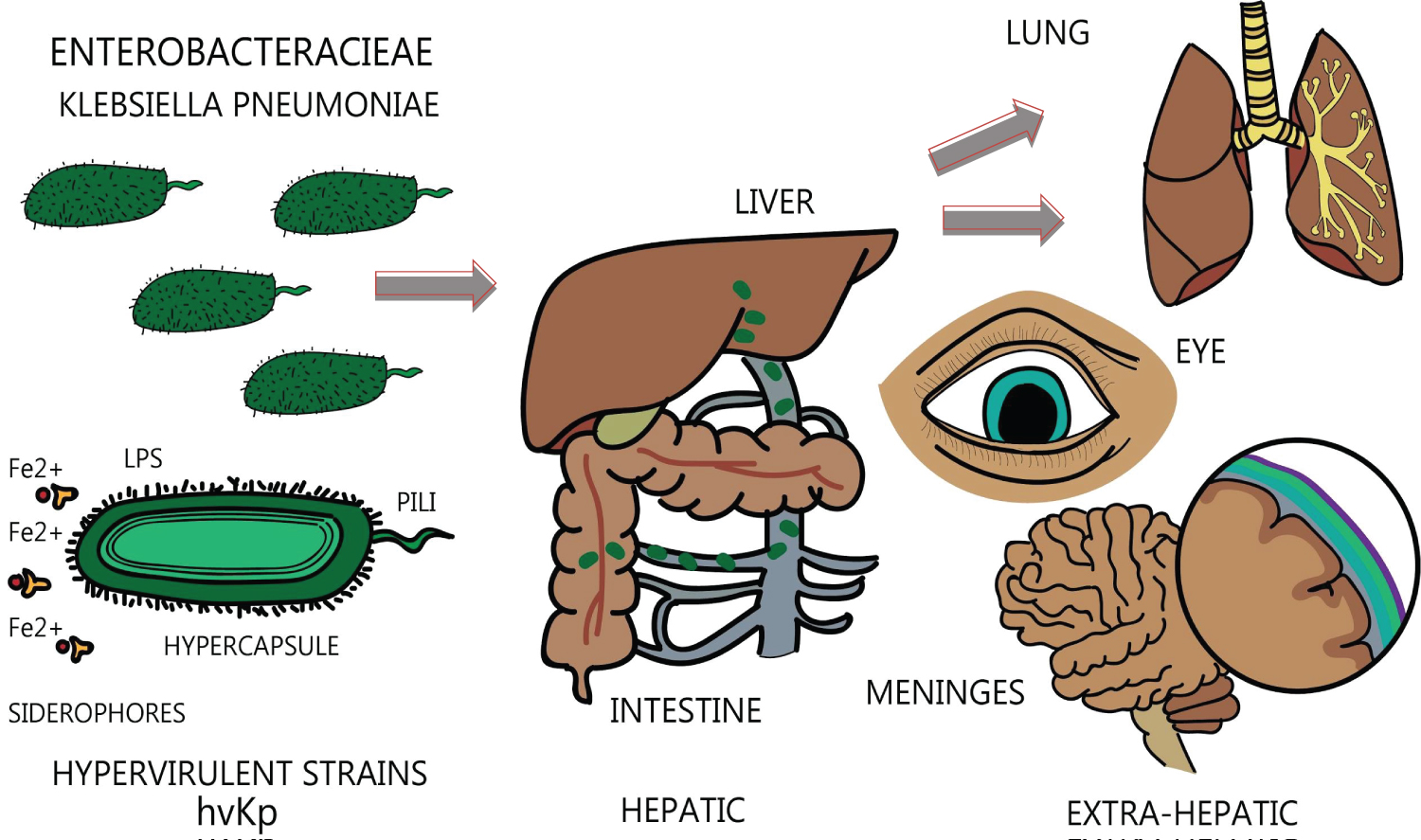 Figure 3: Illustration of pathogenesis in KPIS.
View Figure 3
Figure 3: Illustration of pathogenesis in KPIS.
View Figure 3
Virulence is determined by capsular antigens which grant the pathogen unique hypermucoviscous properties and enables it to avert phagocytosis from the host [15-17]. A specific genomic profile upregulates capsular antigens, such as the mucosity-associated gene A (magA) and the regulator of mucoid phenotype (rmpA) gene [18]. Other virulent factors such as siderophores, pili and lipopolysaccharide are thought to be mediated through other genes and are less influential in bacterial virulence, as compared to the hypercapsule [19]. In our study, no genomic profile was performed which limited the microbiological confirmation, despite having highly suggestive clinical presentation.
This syndrome has been reported more frequently among Asians and diabetics, yet the reason for this remains unknown. It is hypothesized that diabetes decreases the host's immune response, inhibiting phagocyte chemotaxis and activation [20,21]. Increased incidence of K1/K2 hypervirulent strains in the Asian population, when compared to other ethnicities, has been reported. KPIS is rarely seen among Hispanics; however, some cases have been anecdotally reported in the United States -especially on recent travelers abroad [5,22,23] increasing the relevance of this case.
Despite their aggressive behavior, nearly all hvKp strains are susceptible to most broad-spectrum antibiotics, including beta-lactams [24]. Some reports show coexistence of extended-spectrum beta lactamases (ESBL) or carbapenem-resistance with hvKp isolates [14,21] which may be attributable to its genomic flexibility. Previous or regular use of antibiotics is related to increased Klebsiella colonization and may increase the risk for community-acquired antibiotic resistance strains of hvKp [25,26]. Nonetheless, the large majority of species causing pyogenic liver abscess exhibit a favorable susceptibility profile, as seen in our case.
KPIS presentation can mimic that of many malignancies and mycobacterial infections and initial clinical suspicion is difficult [2,27]. However, it must be considered in a patient with liver abscess and extrahepatic seeding. Endogenous endophthalmitis due to K. pneumoniae is widely reported in the literature [28-31]. Other manifestations include pulmonary involvement [32] with lung abscess [33] and ARDS [34], meningitis [35], necrotizing fasciitis [36], vertebral discitis [37], multifocal osteomyelitis [38], prostate abscess [39], splenic, neck, cerebral, and psoas muscle abscesses, otitis media, and arthritis [40]. In our case, the patient presented with liver abscess and septic pulmonary embolism which is considered in the literature as a rare extrahepatic complication [41]. Nonetheless, from our own unpublished data, pulmonary involvement is comparable to the frequency of distant seeding to the eye (24 and 22%, respectively), in individuals with KPIS in the Americas.
Imaging and bacterial isolation are the mainstay of diagnosis. A positive string test is thought to be highly sensitive [34], whereas genotypic testing is more specific and can be performed when clinical presentation is suggestive of KPIS [11]. A possible coexistence with colorectal carcinoma (CRC) is concerning and appropriate screening may be considered [42].
Standard of care is similar to conventional pyogenic liver abscess: broad spectrum antibiotics and drainage [6]. Third generation cephalosporins are generally favored over first generation, whereas percutaneous access is favored over surgical removal, unless the abscess is multifocal, loculated and large, and percutaneous access has failed [43]. Metastatic complications are managed separately depending on the affected organ and details go beyond the scope of this article.
Mortality rate, yet variable, is reported to be 2.8-8% in non-metastatic forms and up to 30% with extrahepatic seeding [44-46]. Once the infection is cleared, relapse after treatment is exceptional [39].
K. pneumoniae invasive syndrome is a rare clinical entity caused by K. pneumoniae often found in Asians, diabetics or otherwise immunocompetent individuals with no underlying hepatobiliary pathology. This must be included in the differential diagnosis of a patient with acute to subacute presentation of liver abscess and extrahepatic involvement, even in patients that have not traveled to Asia or are of non-Asian descent. Our case is limited by incomplete testing which inflicts bias to diagnosis. Nonetheless, we consider that the presentation is highly suggestive of KPIS and we can only hope that it serves as an example for future physicians to consider this condition sooner.
Dr. Maria Elisa Campos for her invaluable contribution to the illustrations in this article.
This research did not receive any specific grant from funding agencies in the public, commercial or non-for-profit sectors. The authors declare no conflict of interest.