COVID-19 has presented unprecedented challenges due to the sparse availability of information surrounding the novel virus; continuing to gather data on the disease is vital for preventing further devastation. Remdesivir has been introduced as a potential treatment for the viral disease. The goal of this study was to identify the effects of Remdesivir on mortality in critically ill, mechanically ventilated COVID-19 patients.
This observational study analyzed outcomes of ventilated COVID-19 positive patients during April 2020 at a community hospital in New Jersey. Data was collected by retrospective chart review and was reported through hospital discharge or expiration. Patients were classified based on whether they received a 10 day course of Remdesivir, a partial course, or none.
Data from 48 intubated COVID-19 patients was reviewed. Median age was 57-years-old. 40% of patients received a full 10-day course of Remdesivir, and 50% did not receive any. 49% of patients expired in the hospital, and with a significantly higher rate of hospital discharge for those that received a full course of the drug compared to none at all (rate ratio 2.9, CI 1.12-8.30, p = 0.012). Earlier initiation of Remdesivir treatment was associated with sooner extubation (r = 0.75, CI 0.42-0.90, p < 0.001) and shorter hospital stay (r = 0.65, CI 0.21-0.87, p < 0.001).
This data supports the use of Remdesivir in COVID-19 and suggests a significant mortality benefit of the treatment.
COVID-19, Coronavirus, Mechanical ventilation, Survival, Remdesivir
COVID-19: Coronavirus Disease 2019; RNA: Ribonucleic Acid; SARS-CoV: Severe Acute Respiratory Coronavirus; MERS-CoV: Middle East Respiratory Syndrome Coronavirus; PCR: Polymerase Chain Reaction; GFR: Glomerular Filtration Rate; ALT: Alanine Transaminase
The COVID-19 pandemic, a result of the novel severe acute respiratory coronavirus-2 (SARS-CoV-2), has tested the stamina and resources of medical professionals, healthcare systems, and communities worldwide since it first presented in December 2019 [1,2]. This disease has impacted a broad population of individuals in nearly 200 countries. Children to the elderly, males and females, with or without comorbidities have been significantly impacted [3]. The disease manifests commonly with respiratory symptoms ranging from mild to severe, however many inflicted with the virus have been asymptomatic or developed symptoms such as anosmia, gastrointestinal symptoms, chest pain, renal dysfunction, and some even go on to develop multiorgan failure [3,4]. In an attempt to combat this rampant virus, various treatment regimens and protocols have been developed which are still changing to this day [5-7]. The National Institutes of Health have officially recommended the antiretroviral Remdesivir for management of those with severe disease requiring supplemental oxygen [6]. This prodrug, which ultimately inhibits RNA polymerase activity, has been known to be effective against other forms of coronavirus including SARS-CoV and MERS-CoV [8,9]. Data from the compassionate use of Remdesivir early in the pandemic was promising, with the majority of patients having improvement in oxygenation status while on the treatment [10]. Preliminary data from the double-blinded, randomized, placebo-controlled trial of Remdesivir also indicated that this drug was efficacious for reducing recovery time [11].
In order to add to the growing knowledge and information surrounding this treatment option for the novel coronavirus, we performed a retrospective review of the outcomes of critically ill COVID-19 positive patients at a community hospital in New Jersey during the peak of the region's outbreak.
The facility first gained reliable access to Remdesivir for use in COVID-19 patients in early April of 2020. Infectious disease doctors and the hospital research committee identified patients who met criteria to receive the drug. These criteria included being over 18 years of age, hospitalized with confirmed SARS-CoV2 by PCR, requiring invasive mechanical ventilation, with adequate renal function (GFR ≥ 30 ml/min) and ALT ≤ 5 times the upper limit of normal. Patients that were excluded were those with evidence of multiorgan failure, pressor requirements for blood pressure maintenance, renal failure, and pregnant females. If patients were started on the medication and subsequently developed any of the exclusion criteria the treatment was stopped. Informed consent was obtained from all patients or their legal representatives prior to treatment initiation.
The planned treatment regimen for patients consisted of a 10-day course of Remdesivir; an initial dose of 200 mg daily followed by 9 days of 100 mg daily. Prior to Remdesivir initiation some patients were prescribed other therapies at the discretion of the infectious disease, critical care, and primary doctors following the patients. Common additional medications included hydroxychloroquine, azithromycin, and lopinavir/ritonavir, which were discontinued once Remdesivir was started. Some patients also received doses of tocilizumab and, when available, convalescent plasma was used as a supplemental therapy.
Retrospective analysis of deidentified patient data was performed through standardized chart review, including factors such as intubation period, treatment regimens, length of stay, and overall outcomes. Patient data was analyzed throughout the entire admission until hospital discharge or expiration.
The analysis population included all patients who received their first dose of Remdesivir from April 8th until April 30th, 2020. Any patients who were pending final outcomes (hospital discharge or expiration) after 50 days of hospital admission were omitted. Associations between variables such as treatment onset, hospital stay, and intubation period were made using Pearson correlations. Survival data was described with Kaplan-Meier analysis.
In total, there were 49 COVID-19 patients that required mechanical ventilation in the critical care unit of this hospital during the review period. 1 patient's outcome was still pending at the time of this review, and so their data was excluded. Of the remaining 48 patients, 42 were confirmed COVID-19 positive by PCR, and 6 were PCR negative however with high clinical suspicion as deemed by infectious disease specialists. 19 patients (40%) received a full 10 day course of Remdesivir, 5 (10%) received a partial course, and 24 (50%) did not receive any. Of those who received a partial course, treatment was incomplete due to expiration in 4 of the patients and worsening renal function in 1 patient. Table 1 shows the baseline demographic and clinical characteristics of the patients included.
Table 1: Baseline demographic and clinical characteristics of patients. View Table 1
Treatment with Remdesivir did not significantly impact the number of days intubated or length of hospital stay in COVID-19 patients in this analysis. Average length of stay for all patients was 28.46 days (SD +/- 13.45). Patients who received the full course of Remdesivir, those that were started on the treatment earlier in their intubation period tended to have a shorter course of intubation (r = 0.75, CI 0.42-0.90, p < 0.001) as well as a shorter length of hospital stay for those who were discharged (r = 0.65, CI 0.21-0.87, p < 0.001). Mean days to discharge after initiation of Remdesivir was 17.93 days (SD +/- 8.87). Fewer patients who received Remdesivir required reintubation compared to those that did not (1 patient compared to 4 patients).
Half of these critically ill patients in this review expired in the hospital, however only 12.5% of those deaths were in patients who received a full course of the drug. 85% of patients who tolerated the entire treatment course were discharged, whereas only 29.2% of those who did not receive Remdesivir were discharged. The rate ratio for hospital discharge between those with Remdesivir compared to those without was 2.9 (CI 1.12-8.30, p = 0.012). Kaplan Meier survival analysis by 50 days for these patients is shown in Figure 1. Those over 65-years-old had a significantly higher mortality rate than younger patients, 70.83% compared to 29.17% in the younger (CI 13.37 to 61.81, p = 0.004).
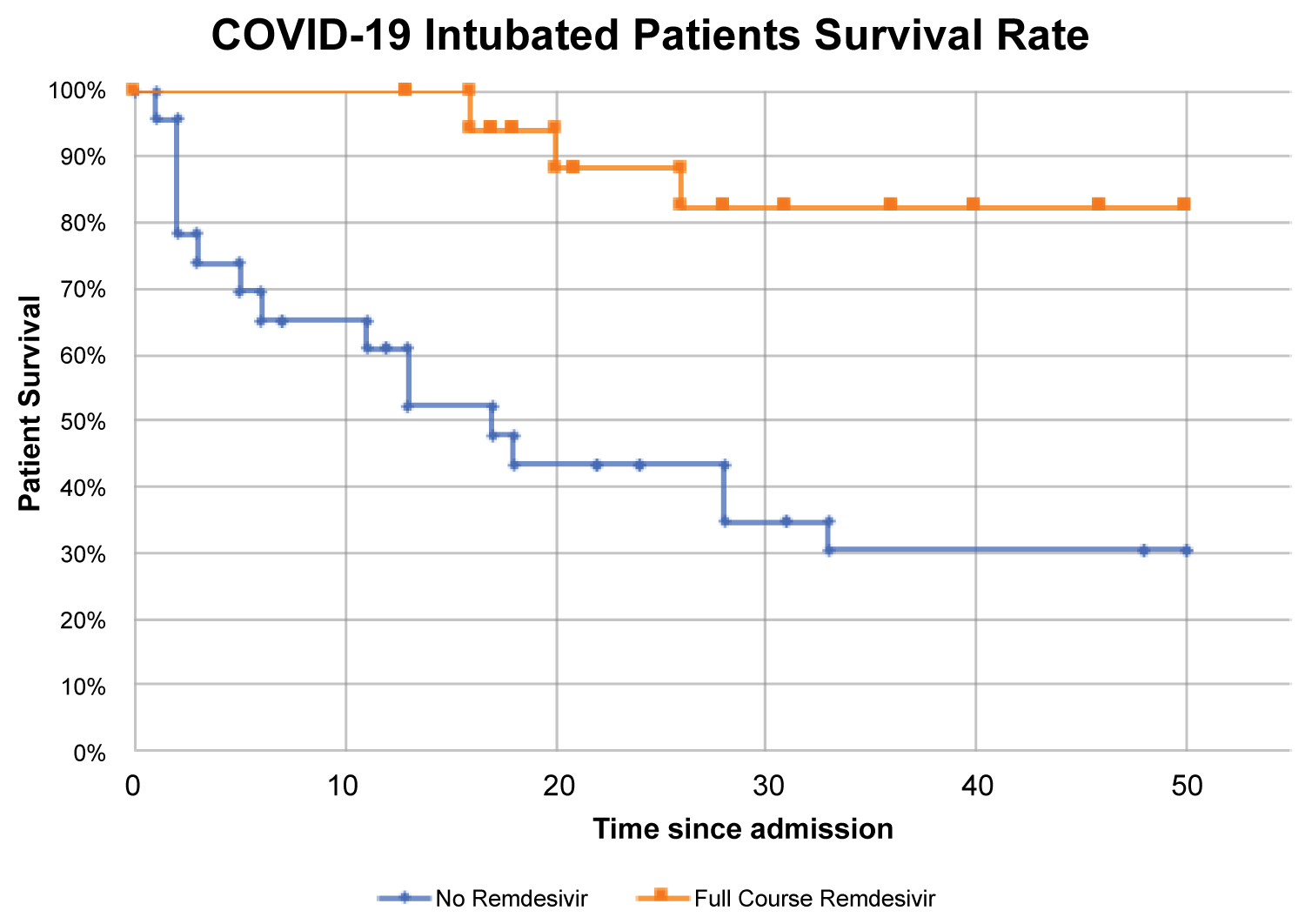 Figure 1: Kaplan-Meier analysis of intubated patients that received Remdesivir compared to those that did not receive Remdesivir. Outcomes followed up to 50 days following admission.
View Figure 1
Figure 1: Kaplan-Meier analysis of intubated patients that received Remdesivir compared to those that did not receive Remdesivir. Outcomes followed up to 50 days following admission.
View Figure 1
Initial results from both the compassionate use of Remdesivir and preliminary clinical trial data have identified that this medication appears to be an effective treatment for COVID-19 [10,11]. Review of our data also showed some promising findings, particularly with regards to improved mortality rates. While some of the increased mortality in those that did not receive the treatment may be attributable to the coexisting conditions which made them ineligible for Remdesivir, the marked difference between the treatment and nontreatment group is notable. Additionally, patients who did not receive the treatment did have higher incidence of comorbidities such as hypertension and diabetes. There were relatively few patients with pre-existing lung conditions.
It is also important to highlight that initiation of treatment sooner after intubation was more beneficial to patients, and as Remdesivir has now become more accessible for use in those not requiring invasive ventilation it is reasonable to consider if early administration of the drug, prior to decline in respiratory status, may help prevent intubation in the first place. While the majority of patients that received Remdesivir within 10 days of reported symptom onset had successful outcomes, our sample size prevented us from drawing any significant conclusions in this regard. There was also insufficient data to examine if a shorter course of Remdesivir would be as efficacious as a 10 day course, however ongoing research in this area is being conducted.
As a part of this retrospective chart review, it was also noted that regardless of whether Remdesivir was administered, most patients received a combination of other medications commonly used for COVID-19 at that time including hydroxychloroquine, tocilizumab, lopinavir/ritonavir, convalescent plasma, vitamin C and zinc. Although polypharmacy as it relates to COVID-19 was common early in the pandemic, these additional agents were similarly dosed across both groups, helping to normalize some of the difference between COVID-19 management treatment plans. Due to the nature of this review, the facility did not have the ability to randomize patients for a study that would better isolate and minimize the effects of comorbid conditions on overall mortality.
This review suggests that Remdesivir treatment is associated with improved mortality outcomes in critically ill COVID-19 patients. These rudimentary findings from patients at this facility supplement what is known about Remdesivir's potential and adds to the expanding knowledge of this disease. With the acute and dramatic onset of this novel illness, there is still much to be learned regarding its pathogenesis and optimal management options.
S.A., K.L., Z.K., and N.S. had the idea for and designed the study; they had full access to all data in the study and take responsibility for the integrity of the data analysis. S.A. and K.L. wrote the first full draft of the report. Z.K. and N.S. contributed to critical revision of the report. S.A. and K.L. contributed to the statistical analysis. All authors contributed to data acquisition and data interpretation, and they all reviewed and approved the final version.
None declared.
The authors would like to acknowledge all of the health care workers at CentraState Medical Center.
None declared.
None.