The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has been reported to cause cardiac complications including myocarditis, acute myocardial infarction (AMI) and various tachyarrhythmias. We present a 63-year-old male who developed nonreversible symptomatic bradycardia due to advanced atrioventricular block (AV) requiring pacemaker placement in the setting of severe SARS-CoV-2 pneumonia.
COVID-19: Coronavirus disease-2019; SARS-CoV-2: Severe acute respiratory syndrome coronavirus; IV: Intravenous; AMI: Acute myocardial infarction; ARDS: Acute respiratory distress syndrome; ACE2: Angiotensin converting enzyme 2; AV: Atrioventricular; AF: Atrial fibrillation; PCR: Polymerase chain reaction; ICU: Intensive care unit
SARS-CoV-2 is a novel coronavirus identified as the pathogen responsible for causing the coronavirus disease 2019 (COVID-19) global pandemic; with number of cases rising and in the absence of an effective treatment, it remains a major health care concern. The clinical course of SARS-CoV-2 infection has been heavily characterized by lower respiratory-like symptoms which include fever, cough and dyspnea as a result of pneumonia or the feared complication of acute respiratory distress syndrome (ARDS) [1]. As the disease continues to spread worldwide, there has been evidence of extrapulmonary manifestations of COVID-19. The cardiovascular system can also be targeted with complications including myocardial injury, myocarditis, arrythmias, heart failure and acute myocardial infarction [2]. Data from the Wuhan, China cohort demonstrate that myocardial injury is common finding that presents in 19.7% of patients and it is associated with more complications and higher mortality rates [3]. The effect on the conduction system resulting in bradyarrhythmia's and atrioventricular blocks remains poorly understood. We describe a case of nonreversible bradycardia resulting from high grade atrioventricular block in patient with COVID-19 infection requiring pacemaker implantation.
A 63-year-old male presented to the emergency department with worsening dyspnea, fevers and cough for 1 week after traveling from New York. His past medical history was significant for hypertension and paroxysmal atrial fibrillation (AF) not on anticoagulation. His home medications include amlodipine 5 mg daily and metoprolol succinate 100 mg once daily. Upon presentation, vital signs were notable for fever of 100.5 °F, elevated blood pressure of 172/84 mmHg, heart rate of 101 beats/min, respiratory rate of 35 and oxygen saturation of 75% breathing ambient air. Physical examination is significant for a well-developed man in severe respiratory distress, normal S1/S2; tachycardia; regular rhythm without murmurs, rubs, gallops, jugular venous distention or peripheral edema. Pulmonary auscultation revealed rales bilaterally.
Laboratory testing revealed leukocytosis of 17.2 K/μl, elevated lactate dehydrogenase of 812 U/L, elevated C-reactive protein of 26.8 mg/dL, and an elevated D-dimer level of 19.56 mg/L. Serum chemistry reveled a potassium of 5.1 mmol/L, magnesium of 2.6 mg/dL, calcium of 8.3 mg/dL and an elevated creatinine of 2.62 mg/dL without an available baseline with a GFR of 25 mL/min. Influenza A/B polymerase chain reaction (PCR) and viral respiratory panel were negative. PCR testing for SARS-CoV-2 returned positive. Electrocardiogram revealed sinus tachycardia with a heart rate of 111 beats/min and no evidence of atrioventricular block (Figure 1). Initial troponin was negative at 0.02 ng/mL. Chest X-ray post-intubation demonstrated a small right apical pneumothorax with bilateral diffuse ground-glass infiltrates (Figure 2). N-terminal-pro-B-type natriuretic peptide elevated at 8860. Echocardiogram revealed mild concentric left ventricular hypertrophy with left ventricular ejection fraction of 60-65%, normal left atrium size, normal right ventricle size and function, trivial pericardial effusion and moderately elevated pulmonary artery systolic pressure. He was noted to have grade I diastolic dysfunction with diastolic parameters of E/e' of 9.14 cm/s, TR velocity of 3.3 m/s, E/A of 0.7 and left atrial volume index of 24.7 ml/m2.
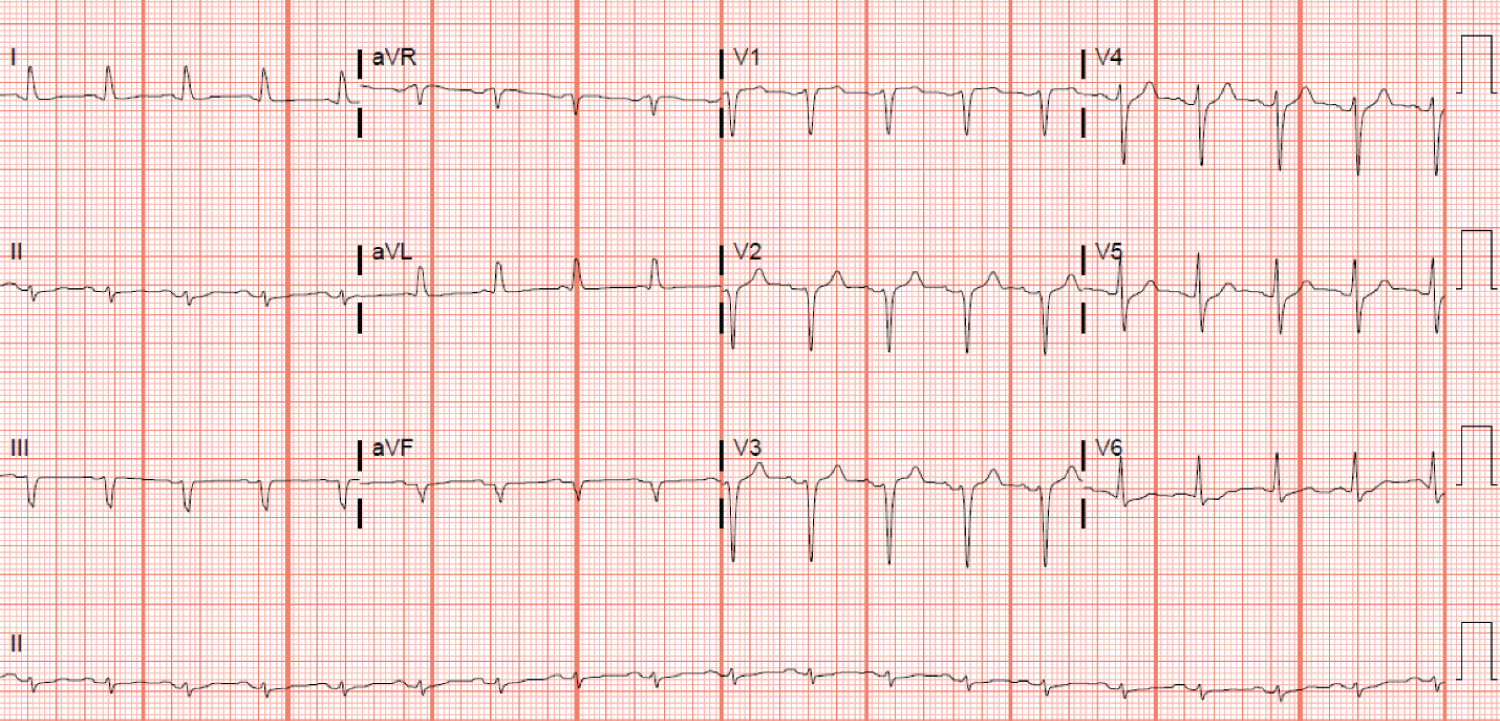 Figure 1: Electrocardiogram: Electrocardiogram showing sinus tachycardia.
View Figure 1
Figure 1: Electrocardiogram: Electrocardiogram showing sinus tachycardia.
View Figure 1
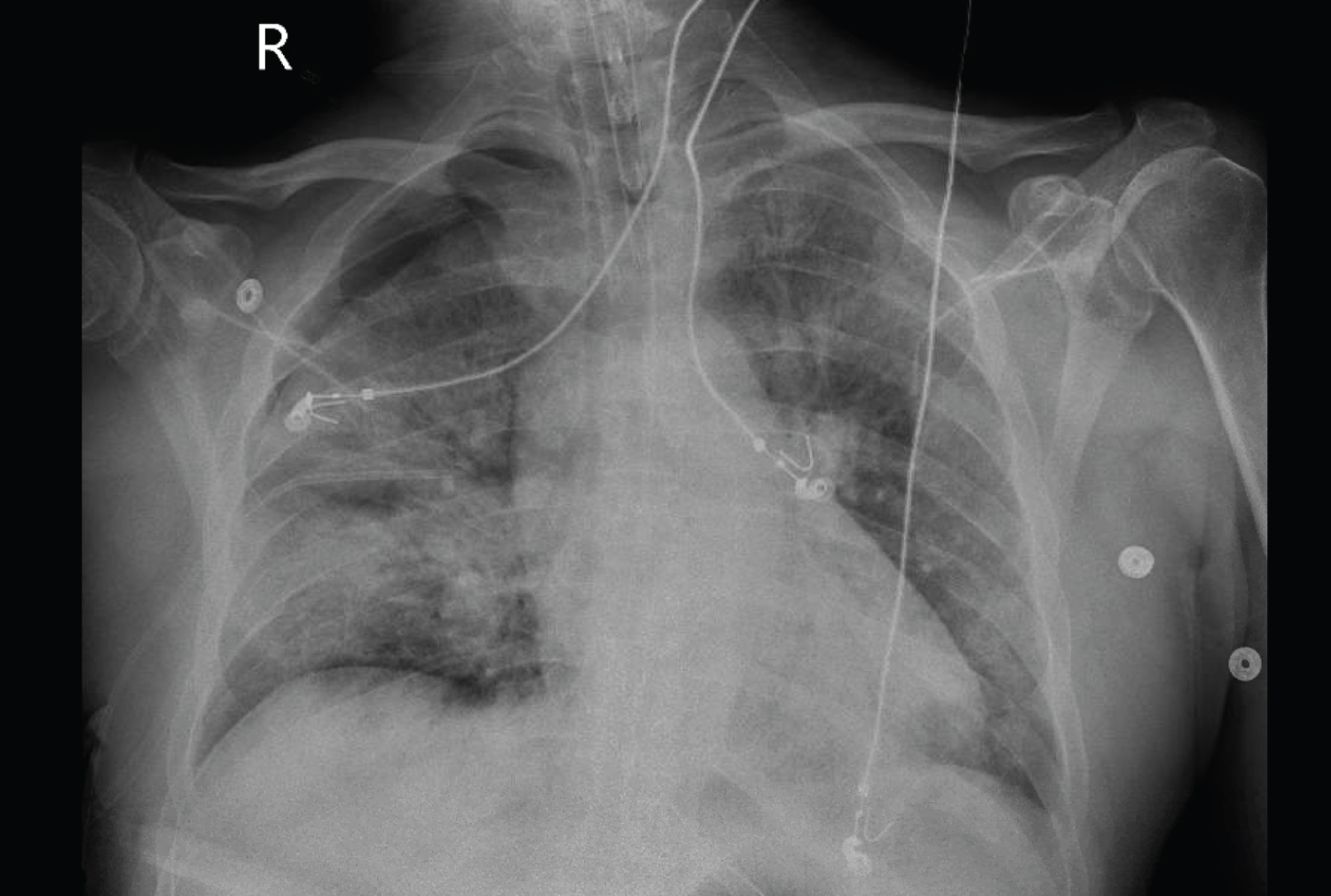 Figure 2: Chest X-Ray: Chest radiograph demonstrating diffuse lung disease, moderate right-sided pneumothorax and well positioned endotracheal tube.
View Figure 2
Figure 2: Chest X-Ray: Chest radiograph demonstrating diffuse lung disease, moderate right-sided pneumothorax and well positioned endotracheal tube.
View Figure 2
The patient was admitted to the intensive care unit (ICU). Initial management included intravenous fluid, and hydroxychloroquine 400 mg once daily. Empiric ceftriaxone 2 gm once daily and doxycycline 100 mg twice daily were used for possible superimposed bacterial pneumonia in the setting of SARS-CoV-2 infection for a total of 7 days. He received one dose of vancomycin 2000 mg which was discontinued following negative methicillin-resistant Staphylococcus aureus screen. Although initially hypertensive, he became hypotensive causing hemodynamic compromise despite IV fluid administration requiring inotropic support. Inotropic support was provided with norepinephrine. He required continuous renal replacement therapy due to acute kidney injury and close hemodynamic monitoring. Hydroxychloroquine was discontinued after 5 days as a result of QTc prolongation. Additionally, a single dose of IL-6 inhibitor tocilizumab was administered. Blood, urine and sputum cultures resulted negative. Two days later, he was noted to have AF with rapid ventricular response with a heart rate of 116 beats/min with conversion pauses up to 5 seconds while on IV diltiazem drip. He was anticoagulated with heparin due to a CHADSVASc of 1. Esmolol drip was transiently started but discontinued due to hypotension. The patient's course was remarkable for tenuous hemodynamics with labile tachy-bradycardia syndrome despite gradual uptitration of metoprolol tartrate to 50 mg twice daily and low dose digoxin c IV daily in the setting of recovered renal function. He developed a 23 second complete AV block that resulted in hemodynamic instability requiring brief advanced cardiac life support protocols (Figure 3). Initially, this was thought to be secondary to a mucous plug triggering a Bezhold-Jarisch reflex while on both digoxin 0.25 once daily and metoprolol 50 mg twice daily, which were discontinued, and he underwent bronchoscopy with removal of moderate thick secretions from central airways. Despite discontinuing rate-controlling agents, 10 days later, he experienced several additional episodes of complete AV block lasting up to 15 seconds. Electrocardiogram obtained after both pauses revealed AF with normal QTc. His overall clinical course had markedly improved, yet he continued to have significant tachy-bradycardia episodes. In the absence of underlying reversible etiology, a dual lead permanent pacemaker was placed. Following pacemaker placement his clinical condition improved and he was discharged to an acute rehabilitation facility.
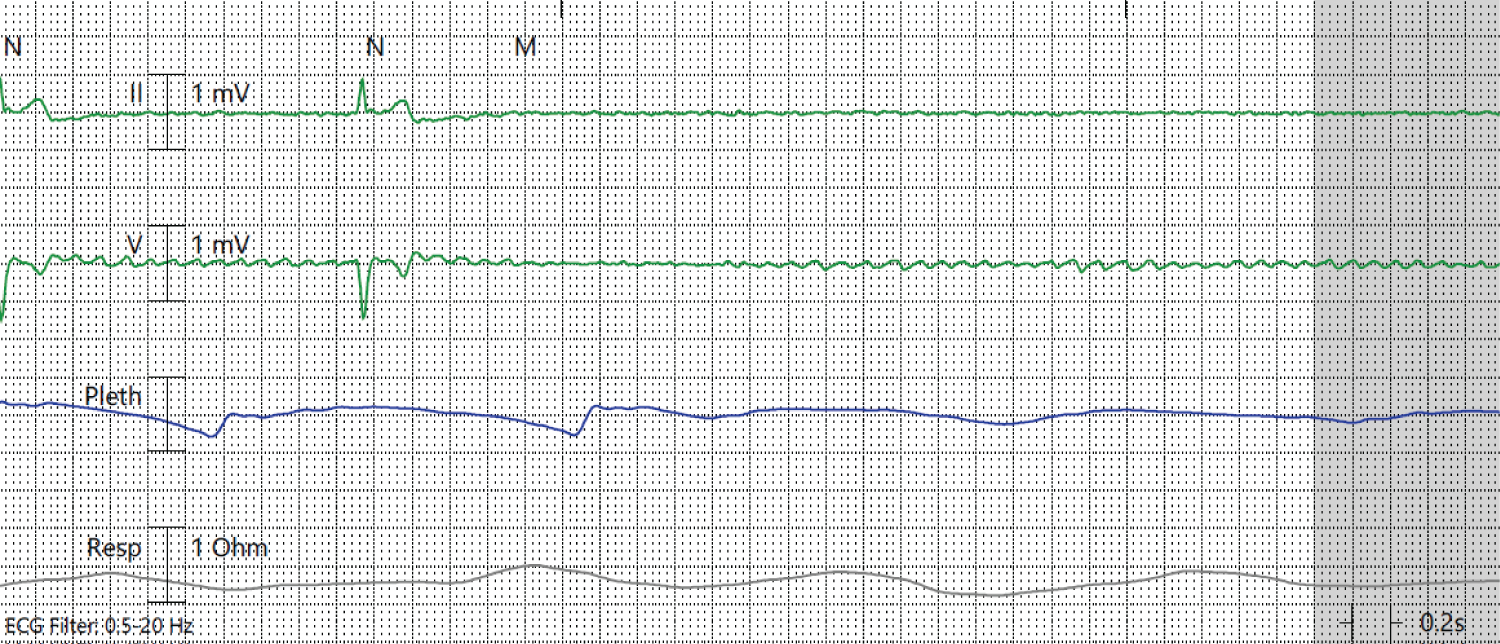 Figure 3: Telemetry: Telemetry demonstrating asystolic pause.
View Figure 3
Figure 3: Telemetry: Telemetry demonstrating asystolic pause.
View Figure 3
Although individuals with preexisting cardiovascular disease and COVID-19 have increased risk of mortality, the exact pathogenesis of cardiac involvement is poorly understood [4]. One ongoing theory involves viral port of entry. The virus invades host cells by binding Angiotensin-converting enzyme 2 (ACE2), a protein found in high concentration in pneumocytes and cardiac myocytes involved in breaking down a proinflammatory molecule called angiotensin II [5]. Once the virus binds ACE2, it dysregulates this protective mechanism leading to pneumocyte and myocyte injury. As the virus continues to replicate, a state of systemic inflammation with massive cytokine release ensues, leading to myocardial injury, ARDS and multiorgan dysfunction. Reports regarding acute cardiac injury have shown that cardiac troponin I levels were significantly higher with associated EKG abnormalities in those with severe COVID-19 [6].
Dysrhythmias, and other cardiovascular manifestations seen as a consequence of SARS-CoV-2 infections, are present in 17% of hospitalized and 44% of ICU patients infected with COVID-19 [7]. The exact mechanism is poorly understood but severe hypoxia, electrolyte derangements and cytokine surge are viewed as possible contributors. Additionally, it remains unclear what medications are beneficial for patients, as many of the treatment regimens currently being trialed can potentiate arrythmias via QTc prolongation. Our patient developed episodes of profound symptomatic bradycardia with evidence of AV block. Reversible causes such as electrolyte imbalances, medication side effects and physiological causes were initially addressed, and he continued to have these episodes despite clinical improvement from SARS-CoV-2 infection.
The proposed mechanism for COVID-19-induced high degree AV block is not well understood. An important aspect to consider is the impact of the "cytokine storm" that is produced in response to the virus which results in elevated levels of proinflammatory molecules like TNF-α, IL-1 and IL-6. Literature suggests inflammatory cytokines can modulate expression and function of ion channels by acting directly on cardiac myocytes and indirectly through systemic effects perhaps leading to conduction disturbances [8]. Another plausible explanation is direct involvement of the AV node by SARS-CoV-2 as studies in animal models have shown to the presence of ACE2 receptors throughout the conduction system [3,9-11]. New onset AV nodal disease can occur in critically ill patients, myocarditis and ischemic heart disease. Our patient had normal cardiac biomarkers except for elevated pro-BNP levels and normal left ventricular function which suggest against overt myocardial involvement. The elevated pro-BNP level is likely secondary to diastolic heart failure in the setting of hypertensive heart disease as evident by ventricular hypertrophy and diastolic dysfunction seen on echocardiogram (Figure 4). It is possible that COVID-19 infection may be a precipitating factor to progression and unmask individuals with asymptomatic heart failure with preserved ejection fraction.
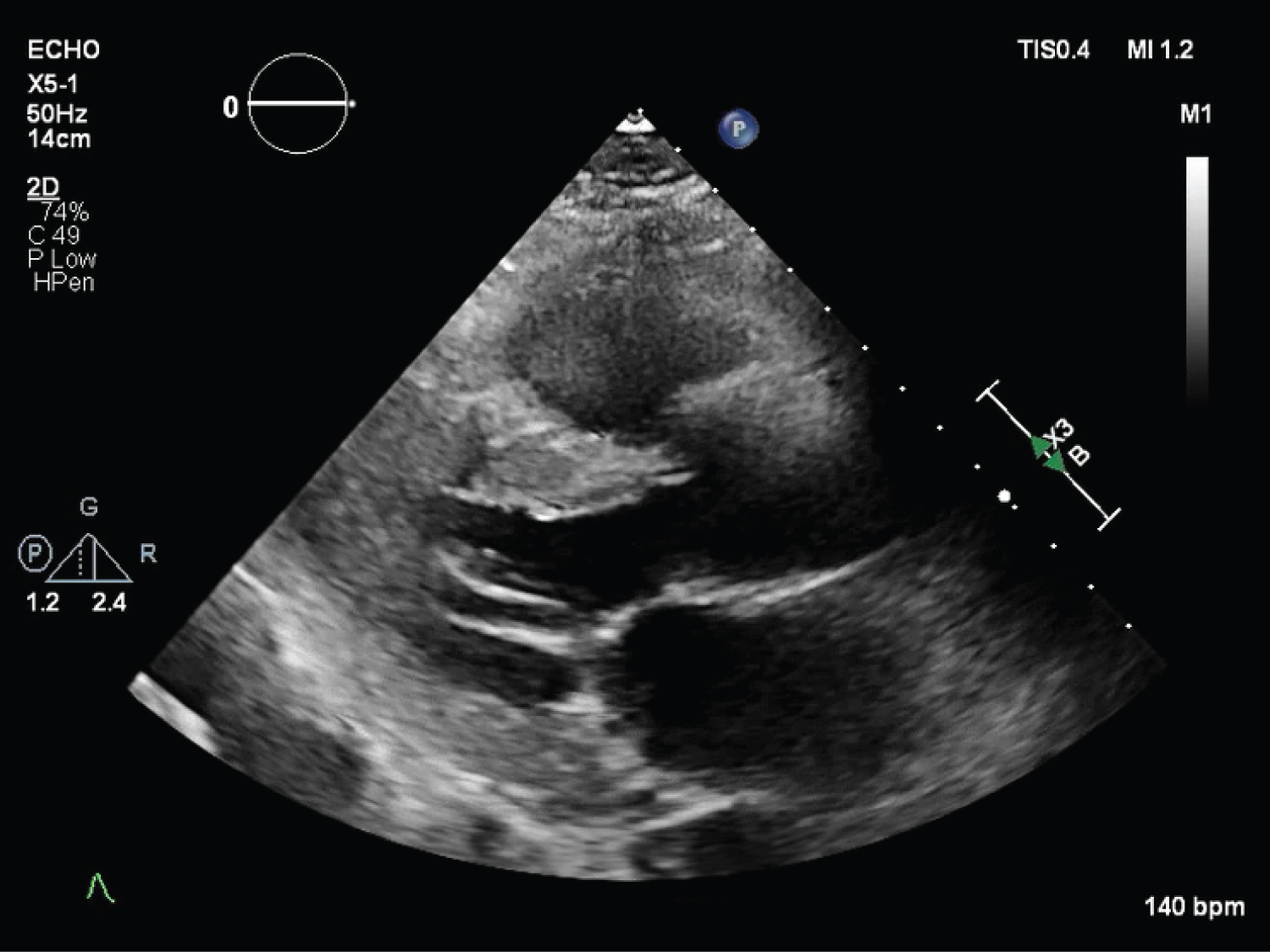 Figure 4: Transthoracic echocardiogram showing normal left ventricular size and function.
View Figure 4
Figure 4: Transthoracic echocardiogram showing normal left ventricular size and function.
View Figure 4
This case highlights the importance of monitoring for extrapulmonary manifestations in patients with COVID-19 infection, particularly unusual cardiovascular complications. We hypothesize subclinical myocarditis caused by COVID-19 resulted in AV nodal dysfunction leading to heart block. Whether the AV nodal dysfunction is due to direct viral involvement or the severe inflammatory response is yet to be determined. However, clinicians must consider a multidisciplinary approach to diagnose and monitor for myocardial injury, tachyarrhythmia and atrioventricular blocks in patients being treated for COVID-19. Further research is needed to characterize mechanism of injury and arrythmia burden to better guide developing therapies.