Left atrial thrombus (LAT) formation is a feared complication of atrial fibrillation, as it can lead to thromboembolic stroke or thromboembolism to another peripheral region causing ischemia. Despite therapeutic anticoagulation, recurrence of thrombi is still possible, although unlikely. Prevention strategies may include reducing left atrial size along with treatment by surgical removal. We present a case of a patient with a large left atrial thrombus in the setting of previous mitral valve stenosis and current atrial fibrillation.
LAT: Left Atrial Thrombus; TEE: Transesophageal Echocardiogram; INR: International Normalized Ratio; DOAC: Direct Oral Anticoagulant
57-year-old female with a history of bioprosthetic mitral valve replacement 6 years prior (27 mm Carpentier Edwards), rate-controlled atrial fibrillation s/p dual-chamber pacemaker on warfarin, and nonischemic cardiomyopathy with reduced ejection fraction of 35%. Patient presented to the hospital for 3 days for worsening shortness of breath. Given concerns of known upper extremity thrombosis, a computerized tomography scan of the chest with contrast was used to rule out a pulmonary embolism and showed an enlarged left atrium with large filling defect. INR on admission was 2.8. On transesophageal echocardiogram (TEE) the next day, there was found to be multiple large left atrial thrombi (largest measuring 7.48 × 3.12 cm), with a significantly dilated left atrium thought to be secondary to a severely stenotic mitral valve. On discussion with the multidisciplinary heart team, we decided to proceed with redo surgical mitral valve replacement and thrombus removal (Figure 1).
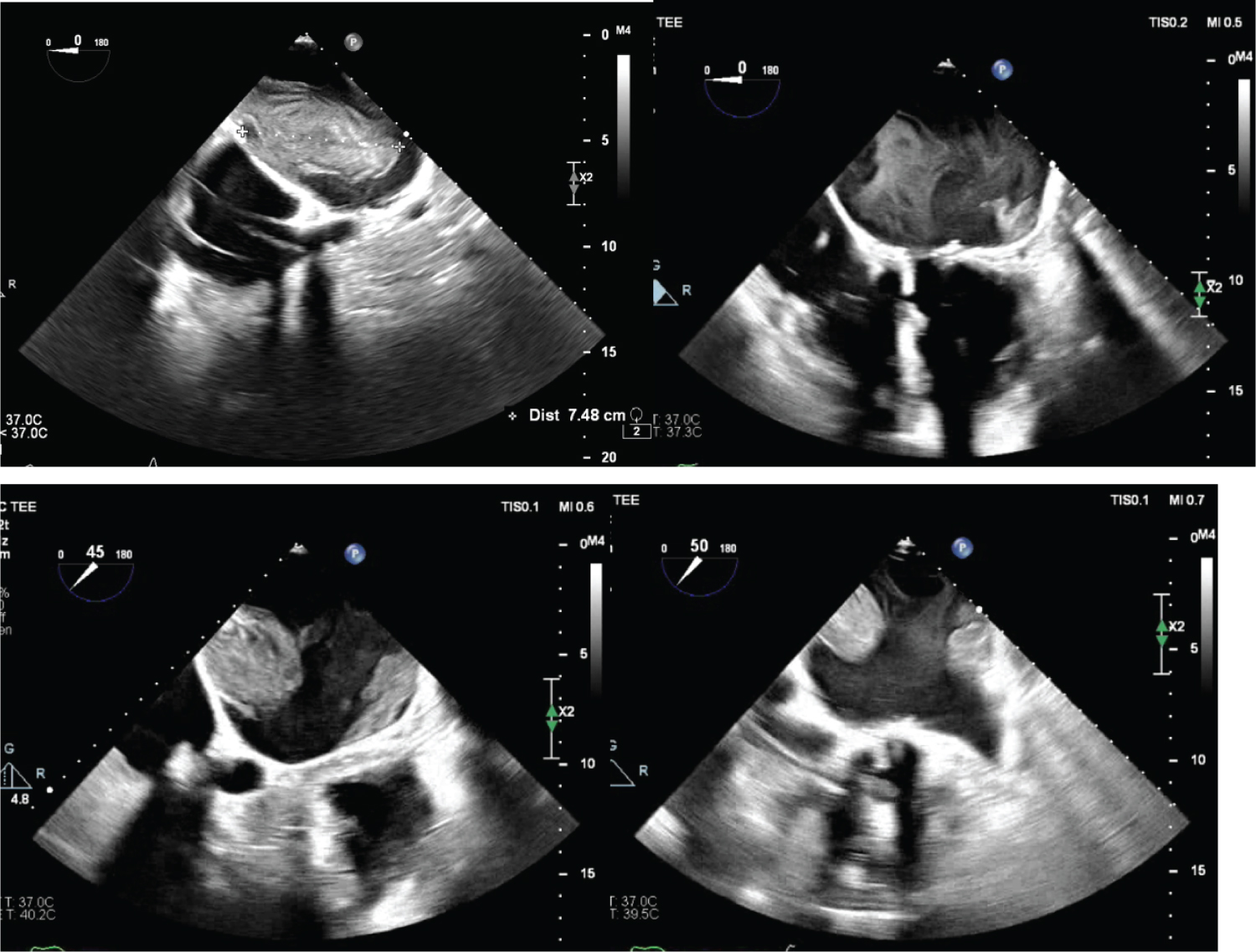 Figure 1: Left atrial thrombus seen on transesophageal echocardiogram.
Figure 1: Left atrial thrombus seen on transesophageal echocardiogram.
The length of one of the thrombi is measured at 7.48 cm in the left upper image. Two separate thrombi can be seen in the left lower image. Interestingly, the left atrial appendage in the right lower image is without a thrombus.
View Figure 1
The patient was taken to the operating room in stable condition. The sternotomy reopening, fascial dissection, and cardioplegia went relatively smoothly. The left atrium was opened, revealing 2 very large masses, which were extensively debrided. The mitral valve revealed a single frozen leaflet, with the remaining 2 leaflets moving well (Figure 2). The valve was excised, and the annulus was resized using a 29 mm Saint Jude medical mechanical heart valve. The left atrial appendage was clipped. Next, a very large amount of the left atrium inferior wall was resected and closed with 2 layers of 4-0 Prolene. Additionally, the superior wall of the left atrium was dissected and oversewed closed to further reduce the left atrial size. Copious irrigation, meticulous avoiding of debris embolization, de-airing, and cross-clamp removal were tolerated well. Repeat echo showed an improved ejection fraction of 40-45%, minimal spontaneous contrast, and a mean gradient of 3 mmHg. The patient was able to wean off pressors and extubated that night. She was discharged home in stable condition on postoperative day 5.
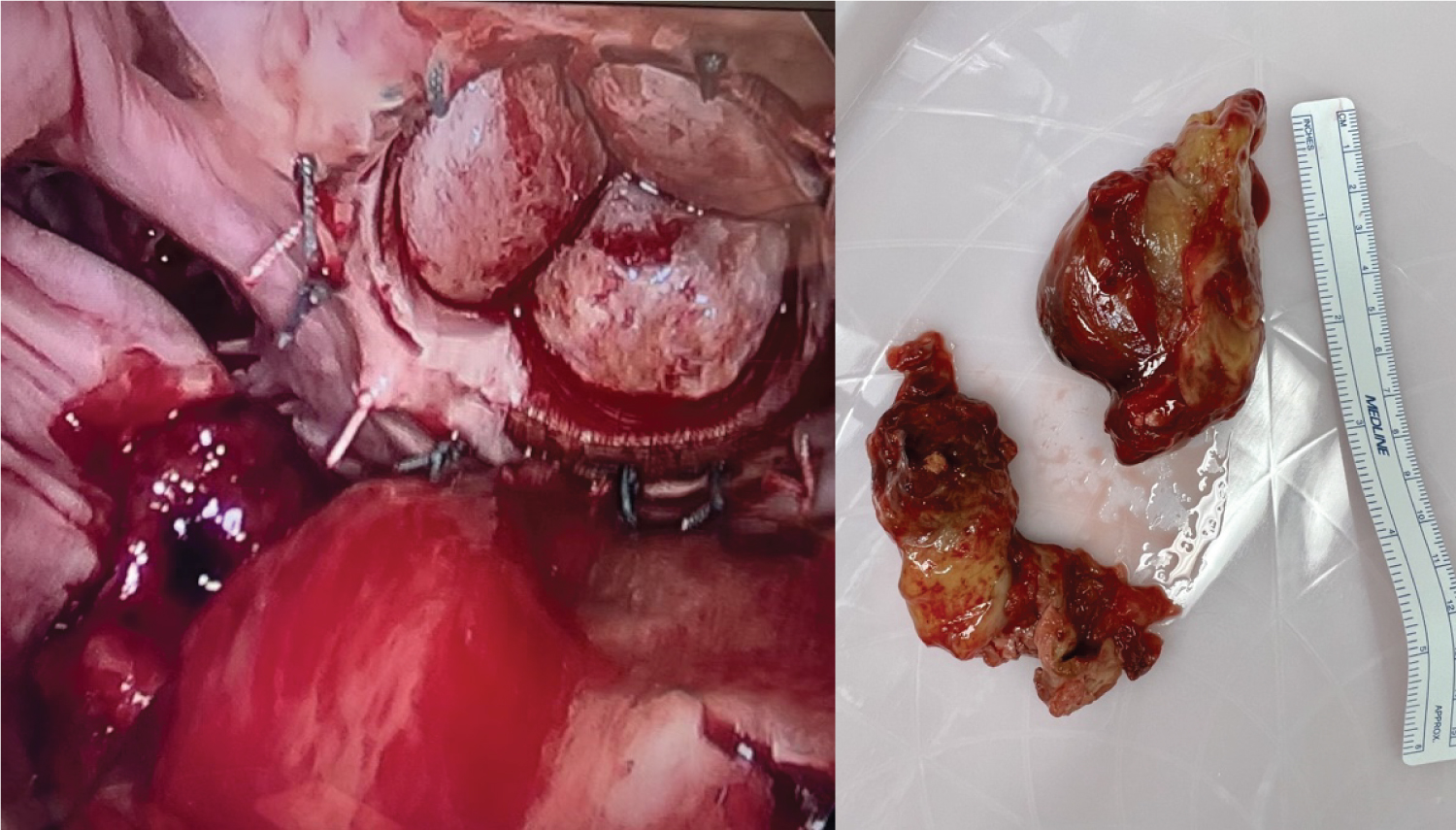 Figure 2: The left atrium and its masses.
Figure 2: The left atrium and its masses.
The left-sided figure shows the intra-cardiac views of mitral valve and masses. The right-sided figure demonstrates the size of the masses.
View Figure 2
This is a very interesting case of a relatively young patient with therapeutic warfarin, given a history of noncompliance, who presented with significantly worsening dyspnea and an extremely large left atrium with significant thrombus burden. Despite the risk of redo sternotomy, cardiothoracic surgery was essential as the thrombus burden in conjunction with the worsening hypoxia would make percutaneous aspiration interventions unfeasible. Additionally, despite the therapeutic INR, the patient had significant thrombus propagation, which warrants further investigation regarding potential anticoagulation failure. The final pathology results revealed two degenerating and focally calcified blood clots, calcified fibrous tissue with hemosiderin laden macrophages without acute inflammation measuring 10 × 8 × 4 cm and 1.2 × 3.5 × 0.4 cm. The mitral valve leaflet showed myxoid degenerative changes and calcifications, without acute inflammation.
Recurrence of venous thromboembolism is uncommon in patients that are treated with vitamin K antagonists and therapeutic INRs, with a risk of 2-4% at 3 months [1,2], however, this was unfortunately the case for the patient described above. While the pathophysiology of thrombus formation despite therapeutic anticoagulation is not well understood, there are some factors that may increase the risk of having recurrent thromboembolism. In an observational study done by Durmaz, et al. [3] it was found that left atrial thrombi despite oral anticoagulation were independently associated with an elevated CHA2DS2-VASc score, elevated left atrial volume, decreased left atrial flow velocity, and decreased left ventricular ejection fraction in patients with permanent atrial fibrillation. In addition, the presence of cancer, chronic cardiovascular disease, chronic respiratory disease, or other clinically significant medical diseases also increase the risk of recurrent venous thromboembolism within the first 3 months of initiating anticoagulation according to Douketis, et al. in a randomized controlled trial [4]. It is important to note that while these factors may play a role in the development of thromboembolism in patients on warfarin, the most likely cause of anticoagulation failure is non-compliance [5], so the importance of compliance should be reinforced in all patients.
An enlarged left atrium also predisposes patients to thrombus formation. While there have been multiple definitions of a giant left atrium, recent reports have followed the definition that a giant left atrium consists of a left atrial size greater than 65 mm by M-mode on echocardiography along with a left ventricular posterobasal wall bent inward and lying between the dilated left atrial cavity, and the left ventricular cavity [6]. This is typically the result of increased pressure and/or volume as can be seen in mitral valve disease such as mitral valve insufficiency or stenosis [7]. Atrial fibrillation can also lead to an enlarged left atrium [8]. Enlarged left atriums increase the risk of thrombogenicity through fibrosis and inflammation, along with increased blood stasis in the left atrial appendage [9]. While atrial fibrillation is common in those with giant left atriums and is a risk factor for thrombus formation, fibrosis on its own is also an independent risk factor for this [9]. In addition to its thromboembolic risks, a giant left atrium may also predispose patients to hemodynamic derangements and even sudden death [10].
Prevention of left atrial thrombi is multi-faceted, with typical strategies focusing on anticoagulation, left atrial appendage occlusion or ligation, rate or rhythm control of atrial fibrillation, and mitral valve repair or replacement. In addition, reduction of left atrial size may theoretically reduce the risk of atrial fibrillation and thrombus formation as well. The primary indication for surgical reduction of a giant left atrium includes intracardiac and/or extracardiac compressive symptoms from neighboring organs, while surgical intervention can also be performed if another surgery is already being planned, such as on the mitral valve, as was seen in our patient’s case, or in the presence of a left atrial thrombus or history of thromboembolic events [6]. Surgical methods include partial plication or resection of the inferior atrial wall, Mercedes-plasty of the inferior wall, triangular resection of the inferior wall, spiral resection of the left atrial wall, or partial heart auto-transplantation [6]. However, it is important to note that giant left atriums with mitral valve disease increase the mortality rates during surgery to 7-23% [11,12], so only a small portion of these patients can safely undergo surgical treatment. While research is lacking on the prevalence of thrombi after left atrial reduction surgery, there does seem to be evidence that this procedure can increase the proportion of patients that restore sinus rhythm, although in this specific cohort of patients from Scherer, et al.’s randomized study all had reduction after radiofrequency ablation [13].
Once a thrombus is present in the left atrium, treatments include pharmacologic therapy or pursuing methods of mechanical removal. Continuing patients on their current anticoagulation regimen is an option, however there is a high likelihood that these thrombi may persist. In a study conducted by Wu, et al, in a cohort of patients with a left atrial thrombus after greater than 8 weeks or anticoagulation, up to 43% of patients did not achieve thrombus resolution [14]. Another option would be to switch from one anticoagulant to another, or more specifically, from a vitamin K antagonist to a direct oral anticoagulant (DOAC), as a meta-analysis from Cheng, et al. seemed to indicate superiority of DOACs of achieving left atrial appendage thrombus resolution compared to warfarin [15], however, this would not be able to apply to patients with valvular atrial fibrillation of with mechanical valves. Some have also suggested switching to unfractionated heparin or low molecular weight heparin or adding aspirin [16]. If pharmacologic options fail, mechanical removal can be achieved via percutaneous suctioning with devices such as the AngioVac [17], or surgical intervention can be pursued if the patient, especially if they are having a surgical procedure for another reason (such as mitral valve replacement as in the patient presented above) [18].
Left atrial thrombi can occur in patients with atrial fibrillation and giant left atriums. This occurs from increased blood stasis and fibrosis. Risk factors for recurrence of thromboembolism despite anticoagulation include an elevated CHA2DS2-VASc score, elevated left atrial volume, decreased left atrial flow velocity, and decreased left ventricular ejection fraction. Prevention of thrombus formation is essential and should be achieved with therapeutic anticoagulation, left atrial appendage occlusion or ligation. Reduction of left atrial size in those with giant left atriums can be considered. Treatment includes pharmacologic and mechanical measures of reducing or removing the thrombus.
None.
None.
All authors contributed equally to the creation of the case report.