Primary hyperparathyroidism (PHPT) in pregnancy is uncommon and poses challenges in managing it with desired good maternal and fetal outcomes. We report two cases of PHPT in pregnancy with challenges in localizing the lesion, one localized successfully using low dose 99mTc-sestamibi and the other patient required neck exploration.
Primary hyperparathyroidism, Pregnancy, Hypercalcemia
PHPT in pregnancy is uncommon, with prevalence rates ranging from 0.03% to 0.05%, particularly posing a greater risk for women aged 45 and above [1,2]. Parathyroid adenomas are the main cause of PHPT, similar to cases not related to pregnancy [1]. During pregnancy, physiological changes such as increased intestinal calcium absorption and enhanced bone resorption can aggravate hypercalcemia in those with PHPT [3]. Rapid absorption of calcium by the fetus through the placenta in the third trimester can be protective against hypercalcemia in the pregnant mother [4]. However, maternal hypercalcemia can result in more calcium crossing the placenta, which can hinder the development of the fetal parathyroid gland and reduce PTH secretion [4]. Fetal complications as result of PHPT during pregnancy includes early miscarriage, stillbirth, intrauterine growth restriction, and fetal hypocalcemia while in pregnant women hypercalcemia can cause preeclampsia, nephrolithiasis, pancreatitis, depression, and seizures [1,5].
Managing PHPT during pregnancy can be challenging and significantly differs in various ways from non-pregnant patients. Scientific evidence regarding this issue is very limited, especially concerning maternal care and fetal outcomes [4]. Complications were found to be higher among patients receiving medical treatment although the evidence for this association is not robust [6]. When it comes to conservative treatment or parathyroidectomy during pregnancy, the decision can be challenging and largely depends on the individual circumstances and the expertise available.
Localizing the parathyroid lesion linked to PHPT prior surgery enables targeted, minimally invasive surgery. Ultrasound of the neck is preferred method as it avoids radiation exposure during pregnancy compared with functional imaging such as 99mTc-sestamibi, 18F-fluorocholine PET/CT, or methionine PET/CT [4]. Herein, we report two cases of PHPT in pregnancy with hypercalcemia with one localized successfully using low dose 99mTc-sestamibi, following a multidisciplinary consensus, as ultrasound had not succeeded in this regard and another patient needing neck exploration.
31-year-old Malay lady with background history of well-controlled bronchial asthma managed with salbutamol and budesonide inhalers, gravida 3, para 1 + 1 (previous first trimester miscarriage in 2016) was referred at 16 weeks of amenorrhea for management of primary hyperparathyroidism. Her first pregnancy in 2017 was complicated by hypercalcemia, which was detected late in the course of the pregnancy. The highest corrected calcium level observed during admission in May 2017 was 3.5 mmol/L (2.20-2.65). In June 2017, prior to delivery, the calcium level was found to be 2.61 mmol/L, with concurrent hypophosphatemia and elevated intact parathyroid hormone (iPTH) level of 14.18 pmol/L (1.58-6.03). The condition was managed conservatively, but she was lost to follow-up after delivery.
In February 2024, she presented to the district hospital with a five-day history of vomiting accompanied by poor appetite and fatigue. She did not report any other symptoms, such as palpitations, fever, or signs of infection. Initial laboratory results indicated elevated calcium of 3.55 mmol/L, accompanied by phosphate of 0.86 mmol/L and 25-hydroxy vitamin D: 16.30 nmol/L (< 50 - Deficient). There was no documented history of calcium supplement consumption, traditional medicine/ lithium use, or familial occurrences of calcium-related issues or cancer.
Despite an initial favorable response to saline treatment, her calcium levels demonstrated fluctuations between 2.92 and 3.49 mmol/L. Subcutaneous calcitonin at a dose of 300 units administered twice daily (weight 60 kg) for 3 days. The corrected calcium levels improved from an initial measurement of 3.49 mmol/L to 3.05 mmol/L. Given the persistent hypercalcemia despite treatment with saline infusion and calcitonin, Cinacalcet was introduced at a dosage of 25 mg administered twice daily. The patient was counselled on the associated risks and benefits and was informed about the limited safety data available regarding its use during pregnancy.
Ultrasound parathyroid was performed but failed to localize the parathyroid lesion. A multidisciplinary meeting (Endocrinologist, Endocrine surgeon, nuclear physician, and obstetrician) concerning fetal radioprotection addressed on the practical modalities of functional imaging, resulting in a consensus on the use of low-dose 99mTc-sestamibi for the localization of parathyroid adenomas. Imaging of the thyroid bed and mediastinum was performed using 13.4 mCi of 99mTc-sestamibi, compared to usual dose of 30 mCi. The estimated absorbed dose to the fetus is 8.9 mGy, which is considered negligible in terms of risk to the fetus. The findings reveal an increased uptake of the tracer at the lower pole of the left thyroid lobe, in favor of a single parathyroid adenoma (Figure 1).
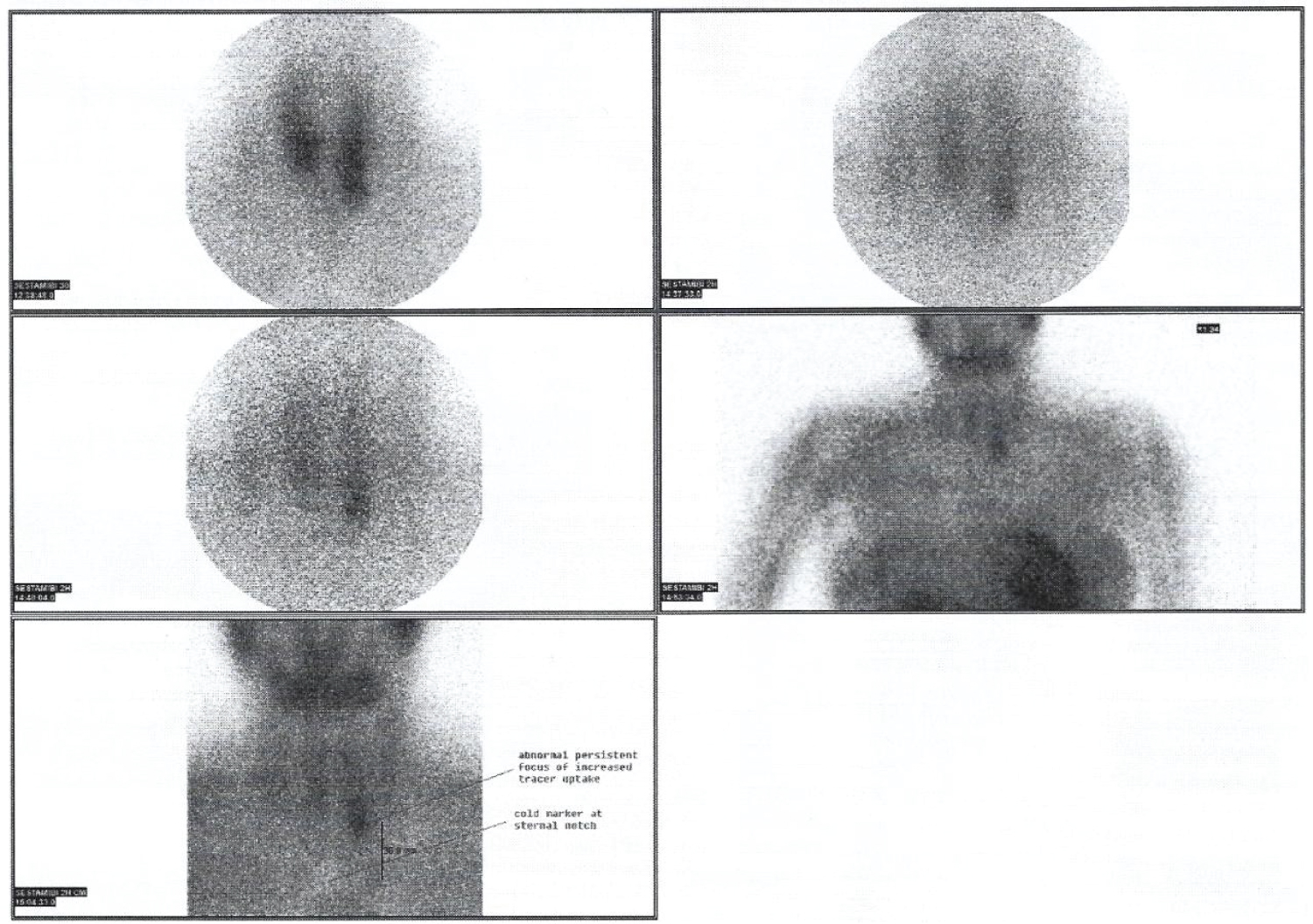 Figure 1: 13.4 mCi of 99mTc-sestamibi.
Figure 1: 13.4 mCi of 99mTc-sestamibi.
Increased uptake of the tracer at the lower pole of the left thyroid lobe, in favor of a single parathyroid adenoma.
View Figure 1
A solid brownish nodule, weighing 1 gram and measuring 1 × 1 mm, was located in the retro-esophageal area of the left inferior parathyroid gland was resected at 19 weeks of gestation. Intraoperative PTH measurements showed a more than 50% drop within 5 minutes confirming successful resection without postoperative complications of hungry bone syndrome. Histological examination confirmed a benign parathyroid hyperplasia. Calcium replacement (CaCO 3 1g twice daily) was instituted for 1 month to limit postoperative hypocalcemia. Post-surgery and throughout her pregnancy, calcium levels remained within the normal range. A healthy baby boy was delivered at 40 weeks, with a good start with a birth weight around the 50 th percentile and no calcium abnormalities were noted in the child.
A 23-year-old woman, gravida 3, para 1 + 1, initially presented with gestational thyrotoxicosis. During follow ups, she was found to have elevated calcium levels at 14 weeks of pregnancy. Subcutaneous calcitonin (200 IU) was started for moderate hypercalcemia of 3.14 mmol/L; however, she could not tolerate it. Fortunately, she responded well to hydration.
Further evaluation revealed PTH-dependent hypercalcemia with corrected calcium at 2.97 mmol/L, phosphate at 0.73 mmol/L, iPTH at 13.41 pmol/L (normal range: 1.3-9.3), and sufficient 25-hydroxy vitamin D levels at 79 nmol/L. The 24-hour urine calcium-to-creatinine ratio was 0.028, favoring PHPT. An ultrasound of the neck showed a hypoechoic lesion in the posteroinferior aspect of the left thyroid lobe, measuring 0.4 × 0.8 × 0.7 cm. Due to the small size of the nodule and its uncertain significance, a low-dose 99mTc-sestamibi scan with radio-guided localization was performed. During the procedure, 20.0 mCi of 99mTc-sestamibi was administered intravenously, with delayed imaging conducted 1.5 hours later. The estimated fetal absorbed dose from this single tracer, dual-phase parathyroid scintigraphy with 20 mCi of 99mTc-sestamibi, was 12.89 mGy. There was no obvious focal increased tracer uptake in the thyroid region or elsewhere in the visualized neck and mediastinum to suggest hyperfunctioning parathyroid tissue. The same day, intraoperative radio-guided localization was performed approximately 3.5 hours after injection of the radiotracer. Intraoperatively, a gamma probe was used to measure the count rate of background (at the isthmus) and suspected left parathyroid lesions. However, both lesions did not meet the count rate criteria for parathyroid adenoma.
Subsequently, she underwent left neck exploration, during which both left parathyroid glands were removed at 17 weeks. Intraoperative PTH monitoring showed a reduction of more than 50% following their removal. Post-surgery calcium levels decreased, and the patient was started on Calcium Carbonate 1 gram twice daily. She was discharged in good condition three days after the surgery. The histopathological examination revealed that the left superior parathyroid gland was consistent with a parathyroid adenoma. To date, she is in her third trimester of pregnancy, maintaining normocalemia while on Calcium Carbonate 500 mg twice daily.
Managing hypercalcemia associated with primary hyperparathyroidism in pregnancy poses considerable challenges particularly due to the lack of established protocols and the limitations of imaging techniques for pre-operative localization. Parathyroidectomy is usually performed in the second trimester as it demonstrated favorable outcomes [4]. Surgery in the first trimester can negatively impact on organogenesis from anesthesia, and surgery in the third trimester can trigger preterm delivery [7].
Conservative medical treatment in pregnant women with PHPT is fundamentally involves administration of oral and/or intravenous fluids, alongside the avoidance of excessive dietary calcium consumption [7]. Cinacalcet, a calcium-sensing receptor agonist, is an option for hypercalcemia in pregnant women, but there are no controlled studies on its use during pregnancy [7]. Cinacalcet is typically reserved for pregnant patients with severe and symptomatic hypercalcemia, primarily serving as a last resort to delay parathyroidectomy until either the second trimester or the postpartum period [7,8]. Cinacalcet was indicated in our case 1 due to severe symptomatic hypercalcemia while awaiting parathyroidectomy.
Once confirming PHPT biochemically, the next step should undertake imaging to localize the lesion if surgical intervention is considered. If surgery is not contemplated during pregnancy, imaging may be deferred until postpartum. To minimize radiation risks during pregnancy, neck ultrasonography is recommended as the preferred first line imaging approach. When an ultrasound exam shows negative or uncertain results, it poses a challenge to decide on the right nuclear medicine imaging technique, either scintigraphy or PET/CT. A comprehensive evaluation of the potential risks and benefits must precede the consideration of 99mTc-sestamibi, 18F-fluorocholine PET/CT, or methionine PET/CT. Notably, the radiation dose to the fetus from a 99mTc-MIBI scan is within safe limits, falling below the threshold that has been established for fetal harm. A prospective registry analysis involving 122 pregnant ladies who received 99mTc scintigraphy in the first trimester at doses of < 5 mGy found no significant association with increased birth defects or unfavorable pregnancy outcomes [9]. Fetal exposure is associated with radionuclides excreted into the maternal bladder, prompting recommendations for proper hydration and regular voiding to minimize this risk [10]. Alternatively, even though 18F-fluorocholine PET/CT potentially offers a lower radiation dose to the mother compared to 99mTc-MIBI SPECT/CT, the specifics regarding fetal radiation exposure from this technique are unclear and may necessitate careful consideration [4]. The fetal radiation dose of 50 mGy is considered safe and unlikely to cause any harm. According to the Centers for Disease Control and Prevention (CDC), radiation doses between 50 mGy and 100 mGy are regarded as inconclusive, and doses above 100 mGy, especially doses above 150 mGy, are viewed as the minimum amount of dosage at which negative fetal consequences may occur, based on observation. Therefore, a parathyroid-localizing scan that does not exceed these exposure levels is unlikely to be unsafe during pregnancy, and its use has been reported [11,12].
Parathyroidectomy is the definitive treatment for primary hyperparathyroidism and is recommended during pregnancy when serum calcium levels exceed 2.75 mmol/L, especially in patients with prior pregnancy loss. A systematic review by Sandler, et al. evaluated 382 cases of gestational hyperparathyroidism, reporting that parathyroidectomy was performed in 71.7% of cases, with non-surgical management in 28.3% [13]. The overall infant complication rate was lower when surgery was performed in the second trimester compared with conservative therapy (9.1% vs. 38.9%). In patients with negative localization (ultrasound and sestamibi scan), unilateral neck exploration with intraoperative parathyroid hormone (IOPTH) monitoring can achieve a first-time cure rate of 92.7% [14]. Following surgery, calcium levels must be closely monitored to avoid over- or under-replacement.
Genetic testing is usually recommended for patients with PHPT who are under 30-years-old or have multiglandular disease or certain syndromic features [15]. We opted to forgo genetic testing in our patients, due lack of characteristic features. However, they will be under periodic monitoring and follow up.
The choice to pursue medical or surgical intervention for PHPT during pregnancy should be determined through a comprehensive risk evaluation performed by surgeons, obstetricians, nuclear medicine physicians and endocrinologists. In cases where the neck ultrasound failed to localize, it is imperative that decisions should be derived from a comprehensive multidisciplinary consultation. The selection of an imaging protocol for this pregnant woman, it is vital to minimize radiation exposure to the fetal thyroid and the whole body to the lowest level that is reasonably feasible. Our cases illustrate that nuclear medicine functional imaging can be done according to the nuclear physician's choice of method, as the results are key for surgical management. Optimal timing for surgery can improve outcomes, underscoring the importance of tailored care for these complex cases.
• During pregnancy, physiological changes such as increased intestinal calcium absorption and enhanced bone resorption can aggravate hypercalcemia in those with PHPT.
• Cinacalcet is typically reserved for pregnant patients with severe and symptomatic hypercalcemia, primarily serving as a last resort to delay parathyroidectomy until either the second trimester or the postpartum period.
• Localizing the parathyroid lesion linked to PHPT prior surgery enables targeted, minimally invasive surgery. We emphasized two patient with PHPT in pregnancy with hypercalcemia with one localized successfully using low dose 99mTc-sestamibi, following a multidisciplinary consensus, as ultrasound had not succeeded in this regard and another patient needing neck exploration.
We would like to thank the Director General of Health Malaysia for his permission to publish this article.
All authors made individual contribution to authorship. All authors reviewed and approved the final draft.
No public or commercial funding.
None declared.
Signed informed consent obtained directly from patient.
Original data generated and analyzed during this study are included in this published article.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.