Prescriptions for opioid medications has increased during the past two decades. In 2016, there were 17,087 deaths involving prescription opioids, or approximately 46 deaths per day. This is a significant increase from 15,281 in 2015 (p < 0.05). The use of injectable opioids are often associated with skin infections, such as Methicillin-resistant Staphylococcus aureus (MRSA). The purpose of this study is to examine the association between opioid dependence and MRSA colonization or infection in hospitalized patients in Florida during 2009 - 2016.
Florida's Agency for Health Care Administration (AHCA) database was used for this study and includes discharge data from 299 hospitals in Florida. Patients 18 years or older with diagnoses of opioid dependence or MRSA infection or colonization were identified. Admissions to psychiatric and rehabilitation hospitals were not included in the analysis. Data was aggregated by the 11 Local Health Council (LHC) regions and includes all 67 counties.
We examined more than 17 million hospitals admissions reported to AHCA between 2009 and 2016. We identified 177,752 (1.0%) admissions of patients with opioid dependence diagnosis, and 359,420 (2.1%) admissions of patients with MRSA. The rate of opioid dependence increased from 5.3 per 1,000 hospital admissions in 2009 to 16.6 in 2016. Substantial increases were evident in all LHC regions. MRSA infections were identified in 8,345 (4.7%) of the admissions of patients with opioid dependence, and in 351,075 (2.0%) of the patients without opioid dependence. The patients in opioid dependence group were 2.4 times more likely to have a MRSA diagnosis compared to the patients in non-opioid dependence group (OR = 2.38, 95% CI 2.33, 2.43, p < 0.001). Significant association between opioid dependence and MRSA was found in all LHC regions.
This study identified significant associations between opioid dependence and MRSA infection or colonization, overall, and in all LHC regions. Although preventive efforts such as screening, isolation, and handwashing are taking place in hospitals and communities, the findings illustrate the importance of implementing routine screening for MRSA in people with opioid dependence, as well in bringing awareness about MRSA transmission within communities.
Opioid dependence, MRSA, AHCA, Local health council
AHCA: Agency for Health Care Administration; CDC: Center for Disease Control and Prevention; CA: Community-Associated; HACO: Health Care-Associated Community-Onset; HO: Hospital-Onset; LHC: Local Health Council; MRSA: Methicillin-Resistant Staphylococcus aureus
Extensive use of opioids, prescribed or not, may lead to opioids dependence, abuse, or death. According to the Center for Disease Control and Prevention (CDC)'s classification, the opioids are grouped into four categories: 1) Natural opioid analgesics, including morphine and codeine, and semi-synthetic opioid analgesics, including drugs such as oxycodone, hydrocodone, hydromorphone, and oxymorphone; 2) Methadone, a synthetic opioid; 3) Synthetic opioid analgesics other than methadone, including drugs such as tramadol and fentanyl; 4) Heroin, an illicit (illegally-made) opioid synthesized from morphine that can be a white or brown powder, or a black sticky substance. In 2016, the opioid related deaths accounted for 66.4% of all 63,632 drug related deaths [1]. In Florida alone, 4,728 all drug overdose deaths occurred in 2016, a 46.5% increase from 3,228 deaths in 2014. The number of drug overdose deaths in the United States involving any opioid significantly increased from 33,091 in 2015 to 42,249 in 2016, which is equivalent to a 27.9% increase in the rate of drug overdose deaths involving any opioid (p < 0.05) [2]. When reporting deaths involving opioid analgesics, CDC's standard analysis approach combines the natural, semi-synthetic opioids, and methadone, also referred to as prescription opioids. Using this method, there were 17,087 deaths involving prescription opioids in the United States in 2016, equivalent to about 46 deaths per day. This is a significant increase from 15,281 in 2015 (p < 0.05). While the rate in deaths involving Methadone increased slightly (from 3,301 in 2015 to 3,373 in 2016, about 2%), the overdose death rate involving natural/semi-synthetic opioids increased 13.8% (from 12,727 in 205 to 14,487 in 2016) [3,4]. However, the data show that the death rates for synthetic opioids other than methadone, such as tramadol and fentanyl, increased 100% from 9,580 in 2015 to 19,413 in 2016, and the heroin death rates increased 19.5% from 12,989 in 2015 to 15,469 in 2016.
Prescriptions for opioid medications has increased substantially from 2002 through 2010 in the United States but then decreased slightly from 2011 through 2013. Reported heroin use generally increased over time. The rate of heroin-related poison cases started increasing in 2006 and appeared to accelerate in late 2010 [5].
Along with the immediate medical problems, opioid dependence can lead to violence, affecting relationships and the quality of life of everyone around the person with opioid dependence [6].
Methicillin-resistant Staphylococcus aureus (MRSA) is a bacteria that is resistant to many antibiotics. MRSA can cause a variety of problems ranging from skin infections to invasive infections like sepsis and pneumonia [7]. MRSA is a central cause of healthcare-associated infections in the United States and serious infections in the community. A study conducted in 2012 aimed to describe the epidemiology of invasive MRSA in Connecticut and trends over time (2001 to 2010) by place of illness onset (community vs. hospital) and relationship to health care [8]. The researchers classified MRSA cases as hospital-onset (HO) MRSA cases if the blood cultures were collected three or more days after hospital admission, as health care-associated community-onset (HACO) cases if the cultures were collected from outpatients or before the third day after hospital admission from patients with a history of hospitalization, surgery, dialysis, or residence in a long-term care facility in the year before the culture date, or a central venous catheter present at the time of culture. Patients with community-associated (CA) cases had none of the HO or HACO risk factors listed above. The authors found that overall incidence of all MRSA, HO MRSA, and HACO MRSA decreased from 2001 to 2010 by 14.2%, 48.4%, and 3.8%, respectively, while the incidence of CA MRSA increased by 124.8%.
The Emerging Infections Program-Active Bacterial Core surveillance system (EIP-ABCs) at the Centers for Disease Control and Prevention has been tracking invasive MRSA infections in nine diverse US metropolitan areas (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon, and Tennessee). In 2011, fewer invasive MRSA infections occurred among patients during hospitalization than among persons in the community without recent health care exposures. An invasive MRSA case was defined as a positive MRSA culture from a normally sterile body site in a resident form the surveillance area, culture obtained at least 30 days apart of an initial invasive MRSA culture. Normally sterile sites included blood, cerebrospinal fluid, pleural fluid, pericardial fluid, peritoneal fluid, joint/ synovial fluid, bone, internal body site, or other normally sterile sites. Since 2005, adjusted national estimated incidence rates decreased among HACO infections by 27.7% and hospital-onset infections decreased by 54.2%; community-associated infections decreased by only 5.0% [9]. In a different report from 2014, the CDC found that the incidence of HO and HACO MRSA incidence decreased by 36.11% from 2007-2008, and by 5.36% from 2013, while the incidence of CA MRSA increased by 1.57% [10].
The use of injectable opioids are often associated with skin infections as well as invasive infections like sepsis [11,12]. Although MRSA skin and soft-tissue infections decreased 29 percent (from 3.8 to 2.0 per 1,000 hospitalizations) between 2010 and 2014, the rates of the invasive MRSA infections, remained unchanged [13].
MRSA was reported among injecting drug users as early as 1981. Forty cases of MRSA infection occurred in an urban hospital in Michigan from March to December 1980, 24 in drug abusers and 16 in non-abusers, yet the infections were acquired in the community. Patients with MRSA infections had longer hospital stay and they also had more previous experience of antibiotic therapy compared to patients without MRSA infection [14]. In a larger and more recent study, Jackson, et al., 2018, found that 2,093 (5.4%) of the 39,050 invasive MRSA cases reported during 2005-2016 occurred in people who injected drugs. The authors found that the invasive MRSA from injecting drugs increased from 4.1% in 2011 to 9.2% in 2016 [12].
A study conducted in Sweden analyzed data from the national Swedish in- and outpatients registers. It included 73,201 individuals from 1997, 1999, 2004, 2009 and 2013. Among patients with opioid dependence, the number of MRSA cases increased from zero cases in 1997 to 64 cases (1.1%) in 2013. The authors found that opioids dependent patients were almost three times more likely to have MRSA compared to patients with alcohol dependence. This association remained unchanged when adjusting for gender and age [15].
While other US studies investigated other serious infections related to opioid abuse/dependence [16], or associations between MRSA and injecting drugs [12], we found no US studies that examined the association between opioid dependence and MRSA in hospitalized patients in Florida. The purpose of this study is to calculate the rates of opioid dependence in hospitalized patients in Florida from 2009 to 2015, and assess associations between opioid dependence and MRSA by LHC regions.
The Agency for Health Care Administration (AHCA) administers and maintains a database that includes discharge and financial data from all short-term and long-term acute care hospitals in Florida. Administrative data includes diagnosis and procedure codes, charges and other patient characteristics as reported on the uniform billing form at the time of discharge. The data contain no personal identifiers. In 2016, there were 299 hospitals Florida reporting to the AHCA. Patients 18 or older were included in the study. Only admissions to a general acute care urban or rural hospital were included in the analyses. Generally, patients would go to an acute care hospital first before they are sent to a rehabilitation or psychiatric hospital. To avoid double counting these patients, admissions to psychiatric and rehabilitation hospitals were not included in the analyses. Patients with any diagnosis of 304.0 (ICD9 code) or F11.2 (ICD10 code) were classified as having opioid dependence diagnosis. Similarly, patients who did not have a diagnosis code of 304.0 or F11.2 were classified as non-opioid dependent. Patients were classified as having MRSA colonization or infection if they had a diagnosis of any of the following diagnosis codes: 041.12 (ICD9) or B95.62 (ICD10)- MRSA; V02.54 (ICD9) or Z22.322 (CD10)-Carrier or suspected carrier of MRSA; V12.04 (ICD9) or Z86.14 (ICD10) - Personal history of MRSA infection. Data was aggregated by Local Health Council (LHC) region. Florida's LHC regions were established by Section 408.033 Florida Statutes (F.S.), as a network of non-profit agencies, to conduct regional health planning and implementation activities in 11 regions that includes all 67 counties in Florida. These local health councils develop regional health plans containing data, analysis, and recommendations that relate to health care status and needs in the community. The recommendations are designed to improve access to health care, reduce disparities in health status, assist state and local governments in the development of sound and rational health care policies, and advocate on behalf of the underserved [17]. Table 1 presents the counties in each LHC region.
Table 1: Percentage of MRSA by opioid dependence group and Local Health Council location. View Table 1
Data are summarized using frequencies and percentages. Opioid dependence rate per 1,000 hospital admissions were calculated and compared between 2009 and 2016. Using the SAS procedure Proc GMAP, maps were created to illustrate the yearly opioid dependence rate per 1,000 hospital admissions. Pearson's Chi-square tests are used to compare the overall associations between opioid dependence and MRSA infection. The magnitude of these associations are described using odds ratios (OR), along with their 95% confidence intervals. All analyses were done using SAS® for Windows Version 9.4 [18].
There were 17,512,604 general acute hospital admissions in Florida between 2009 and 2016 for patients 18 years or older. Of those, 177,752 (1.0%) were patients diagnosed with opioid dependence. Across Florida, the rate of opioid dependence increased from 5.3 per 1,000 hospital admissions in 2009 to 16.6 per 1,000 hospital admissions in 2016. Figure 1 and Figure 2 display LHC region rates of opioid dependence. In 2009, the rates of opioid dependence varied across the LHC regions from 2.0 per 1,000 admissions in LHC-2 to a rate of 9.3 in patients hospitalized in LHC- 5. The next two highest rates were found in LHC-10 (6.8 per 1,000 admissions), and LHC-8 (6.2 per 1,000 admissions, Figure 1). The rate of opioid dependence increased in all the LHC regions from 2009 to 2016, with the lowest rate found in LHC-11 (7.3 per 1,000 admissions), and the highest rate in LHC-5 (123.4 per 1,000 admissions, Figure 1). The smaller increase was seen in LHC-11, from 4.3 to 7.3 per 1,000 hospital admissions, while the larger increase was found in LHC-5, from a rate of 9.3 to 23.4 per 1,000 admissions.
 Figure 1: Rate of opioid dependence in hospital admissions in 2009 AND 2016, by Local Health Council. View Figure 1
Figure 1: Rate of opioid dependence in hospital admissions in 2009 AND 2016, by Local Health Council. View Figure 1
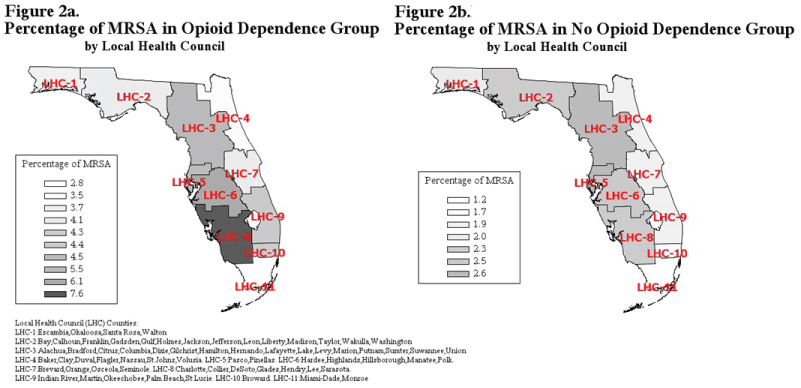 Figure 2: Percentage of MRSA in opioid dependence and no opioid dependence groups, by Local Health Council. View Figure 2
Figure 2: Percentage of MRSA in opioid dependence and no opioid dependence groups, by Local Health Council. View Figure 2
Overall, of all 2009 to 2016 hospital admissions, 359,420 (2.1%) admissions were from patients diagnosed with MRSA infection. MRSA infections were identified in 8,345 (4.7%) of the admissions of patients with opioid dependence, while MRSA infection or colonization was found in 351,075 (2.0%) patients without opioid dependence. The patients with opioid dependence were 2.4 times more likely to have a diagnosis of MRSA infection or colonization compared to the patients without opioid dependence (OR = 2.38, 95% CI 2.33, 2.43). Significant association between opioid dependence and MRSA infection was found in all LHC regions. The highest proportion of MRSA in opioid dependent patients was seen in patients admitted to hospitals located in LHC-3, LHC-6, and LHC-8 (Table 1). Patients with opioid dependence admitted to hospitals in these counties were 2.1 to 3.5 times more likely to have a diagnosis of MRSA infection or colonization compared to patients without opioid dependence.
Our results indicate that Florida hospitals have encountered a significant increase in the number of patients with opioid dependence from 2009 to 2016, overall and within each LHC region. Dart, et al. found that prescriptions for opioid analgesics increased substantially from 2002 through 2010 in the United States but then decreased slightly from 2011 through 2013. These latest reductions in opioid prescriptions might be a result of the multiple programs implemented by local, state, and federal governments to improve and control the opioid prescribing, or of an increase in the death rate involving prescription opioids, as reported by the Center for Disease Control and Prevention in 2016. The increased rate of opioid dependence found in this study is most likely due to an increase use of illegal drugs, similarly to the results reported by Dart, et al. Jackson, et al., provides evidence that person who inject drugs are more likely to develop invasive MRSA infections. Our results indicate significant association between opioid dependence and MRSA infection, across all Florida regions. Patients with opioid dependence were 2.4 times more likely to have a diagnosis of MRSA infection compared to the patients without opioid dependence. Higher risk of MRSA infection was found also by Dahlmana, et al., although they compared the opioid dependence to alcohol abuse. Previous research indicates that rates of health-care related MRSA infections decreased over time, but not the rates of community-associated MRSA infections [8]. Due to the retrospective nature of our study, causality cannot be implied. Although we cannot distinguish between health-care related or community-associated MSRA infections, the fact that there is such a large difference in MRSA rates between opioid and non-opioid dependence patients warrants future research in this area.
To our knowledge, no other study identified an association between the opioid dependence and MRSA infection or colonization in hospitalized patients in Florida. More importantly, our analysis identified regions in Florida where the opioid dependent patients are more likely to have a MRSA infection. Further research is needed to investigate the trends of MRSA infection rates over time, in both opioid and non-opioid dependent populations. Patient and hospital characteristics need to be investigated as well to see if other factors might be associated with opioid dependence and MRSA infection.
Although preventive efforts such as screening, isolation, and handwashing are already taking place in hospitals, and in the communities as well, the results of our study might be helpful for policy makers and medical providers in implementing routine screening for MRSA in people with opioid dependence, as well in bringing awareness about MRSA risks within communities.
No funding or conflict of interest.
CS: Designed the study, analyzed the data, drafted the first manuscript; LB: Generated the study's idea and implemented the study; KL-B: Analyzed data and interpreted results; JM: Designed the study and interpreted the data; SW: Designed the study and interpret the results. All authors edited the manuscript, reviewed and approved the final version, and agreed to be accountable for all aspects of the work.
Approval of this project was granted by the University of Florida IRB-03. This study was approved as exempt because it poses minimal risk.