Tuberculosis is one of the major global public health problems. Each year, there are around nine million new cases of tuberculosis, and close to two million deaths. Ninety eight percent of TB deaths are in the developing world affecting mostly young adults in their most productive years. Providing quality care for pulmonary tuberculosis patients is crucial in prevention and control of the disease. Studies show that consistent compliance with evidence-based guidelines can significantly improve patient safety and quality of care.
The objective of this study was to assess Tuberculosis Diagnosis and Treatment Services in Health Centers of Sekoru Woreda, Jimma Zone, South West Ethiopia in 2012.
The study was conducted from June 25 - July13/2012 and used Cross-sectional study design. The data was collected from 753 program documents (191 from follow up charts of HIV patients, 445 from OPD patients' cards, and 117 from unit TB registers) of Sekoru and Deneba health centers. Eleven health professionals were also interviewed. Descriptive analysis was used to analyze quantitative data using SPSS 16.0 for window and the qualitative data was analyzed in themes and supplemented to the quantitative data.
In this study 445 OPD cards with cough of ≥ 2 weeks, 117 TB patients' information from TB register unit, follow up charts of 53 patients on pre-ART care and 138 patients on ART treatment were reviewed. Of the total 445 patients who visited outpatient with cough of greater than or equal to 2 weeks, 263 (59.1%) were sent to lab and lab results were registered for 209 (47%) patient. 29 (6.5%) were diagnosed as smear negative pulmonary tuberculosis patients and 60 (13.5%) were diagnosed as smear positive pulmonary tuberculosis. The diagnosis of pulmonary tuberculosis positive patients was considered correct in 90% of the patients and none of the diagnoses for the pulmonary tuberculosis negative patients was considered correct based on the national guideline. Correct drugs and correct doses were prescribed in both intensive and continuous phases for 96.1% and 84.5% of the patients respectively. From the total 103 sputum smear positive patients who were on treatment, sputum conversion test was done at the end of 2nd, 5th and 6th/7th months for 87.5%, 84.8% and 79.3% of patients respectively. Treatment outcome of majority of patients were cured (76.1%) and outcome was not written for 3.4% of the patients.
There is under diagnosis of TB after patients come to health centers but once patients are diagnosed, there is good treatment service and high likelihood of getting cured or successfully completing the treatment. A lot remains to be done to improve the service delivery and process of case findings specifically for negative PTB patients so as to reach the performance targets set in the TBL guidelines. This could be ensured through strict adherence to the elements of DOTS strategy. Thus, health workers should be encouraged to adhere to the national guidelines, Quality of reagents should be maintained, and all categories of anti TB drugs should be availed all times. Training, Supervision and follow up should also be strengthened.
Tuberculosis, Jimma, DOTS
Tuberculosis (TB) - an infectious airborne disease - is believed to have been present in humans for thousands of years. However, due to the variety of its symptoms, it was not identified as a unified disease until 1820's, due to the variety of its symptoms, and was not named as tuberculosis until J.L. Schonlein named it as TB in. In 1854, Hermann Brehmer proposed the idea that tuberculosis was indeed a curable disease [1].
Worldwide, tuberculosis (TB) is one of the top 10 causes of death, and the leading cause from a single infectious agent (above HIV/AIDS); millions of people continue to fall sick with the disease each year. In 2017, TB caused an estimated 1.3 million deaths (range, 1.2-1.4 million) among HIV-negative people, and there were an additional 300,000 deaths from TB (range, 266,000-335,000) among HIV-positive people. There were an estimated 10.0 million new cases of TB (range, 9.0-11.1 million), equivalent to 133 cases (range, 120-148) per 100,000 population. Nevertheless, 85% of cases occur in Africa and Asia. The burdens for Africa and Asia accounted for 30% and 55% respectively, while India and China alone represent 35%. If left unchecked, within 20 years TB will kill a further 35 million people. It especially affects the most vulnerable such as the poorest and malnourished. TB is also a leading killer among young women, especially in Africa. In 2008, 3.6 million women fell ill with TB and 700,000 women died from TB including 200,000 women with HIV. TB is the third leading cause of death worldwide among women aged 15-44 [2-4].
Ethiopia ranks seventh among the world's 22 high-burden tuberculosis countries. According to the World Health Organization's (WHO's) Global TB Report 2011, the country had an estimated 156,928 TB cases in 2010, with an estimated incidence rate of 261 and prevalence rate of 394 cases per 100,000 population [5].
Studies show that consistent compliance with evidence-based guidelines can significantly improve patient safety and quality of care [6].
At the most basic level, health workers may simply not be familiar with standards because they have not been clearly communicated. In other cases, health workers may lack the necessary supplies or equipment to perform according to standards. Commonly, providers are aware of standards but may hold beliefs or attitudes that inhibit them from adhering to standards. Health workers may doubt the efficacy of or disagree with specific standards or reject the idea of explicit standards in general, believing that practice guidelines restrict provider autonomy or compromise the "art" of medicine [7].
Study done in 2008 at Jimma zone using facility based cross sectional design to assess quality of care delivered for infectious pulmonary tuberculosis patients, showed that 6 (60.0%) of the health facilities had sufficient laboratory reagents and slides for sputum smear microscopy. Only 5 (50.0%) of the Health facilities had a copy of TLCP manual and teaching material (flip charts) on TB. All the health facilities 10 (100.0%) under the study had at least one health professional with special training on DOTS, while 5 (50.0%) of them had two. All of them had at least one laboratory technician and in 8 (80.0%) of the facilities the laboratory technician had special training on DOTS program. 7 (70.0%) and 6 (60.0%) of the health facilities had adequate toilet and sufficient room for the patient load, respectively [8].
Another study done on the quality of tuberculosis diagnosis in districts of Tigray region of northern Ethiopia, the diagnosis was considered correct in 33 of the 42 smear-positive PTB patients and incorrect in 9 patients. Of 101 smear-negative PTB patients, 31 (31%) were diagnosed as per the national diagnostic guideline. In more than half of patients treated for lymph node tuberculosis, their diagnosis was inconsistent with the national diagnostic guideline. Non-adherence to the national guidelines was a major problem in district hospitals. This called for action to promote clinicians' adherence to the national diagnostic guidelines [9].
Study done on Quality of tuberculosis care and its association with patient adherence to treatment in eight Ethiopian districts showed that TB care providers were untrained in 18 (44%) of 44 facilities and daily outpatient TB care was not given in 13 of 44 (25%). Among the 237 patients, 43% interrupted treatment for 15 days and 30% had at least 1 day's dose of TB drugs unused. Patients tended to interrupt and default from treatment when their care provider had been inadequately supervised by district TB control experts and was incapable of dealing with patients' minor illnesses. Unavailability of daily TB care in health facilities was associated with missing daily doses [10].
The general objective of the study was to assess Tuberculosis Diagnosis and Treatment Services delivery in Health Centers of Sekoru Woreda.
1. To assess compliance of health workers to the NTP guideline in the diagnosis of TB.
2. To assess compliance of health workers to the NTP guideline in the treatment of TB patients.
3. To determine the availability of adequate resources for TB-DOTS program implementation.
Sekoru Woreda is one of the 18 Woredas and one town of Jimma Zone. It has an estimated area of 925.1 km2 and is located 105 Kms East of Jimma town. It has 2 urban centers, including Sekoru town which is the district's administrative center. The total population of the Woreda was about 152,253, of which 137,259 were rural and 14,994 were urban populations. Livelihood depends upon agriculture and the average family sizes for rural and urban area are 4.7 and 4.6 persons respectively. The district's crude population density is estimated at 129 persons per km2.
The study was conducted from June 25 to July 13, 2012.
Institutional based Cross-sectional study design was used which involved two health centers (Sekoru health center and Deneba health center) that provide DOTS-TB diagnosis and treatment services in the Woreda. Both quantitative and qualitative methods were employed. The quantitative data was collected on variables like TB suspects that were correctly identified, diagnosed and treated to check adherence to the standards. The Qualitative was to complement the data which was collected by the quantitative method as well as to check quality of service provide and to triangulate the data.
Source population: The source population of the study were TB program documents (outpatient department cards; documents of patients from unit TB register; Pre antiretroviral therapy (Pre ART) and ART follow up charts) and health professionals in Sekoru and Deneba health centers.
Study population: The study population was all OPD cards with cough of ≥ 2 weeks from 11-09-2010 to 10-09-2011; information of PTB patients on unit TB register from Sep 2010 to June 2012; follow up charts of HIV patients on Pre ART care and ART treatment in 2012 and selected staff providing TB diagnosis and treatment in the two health centers.
Study units and sampling units: The study units were individual health experts in the selected two HCs, OPD cards, TB register and Pre ART and ART patients' follow up chart of the two selected health centers. In this study, health centers providing diagnosis and treatment for at least the last two year were involved in the study from the Woreda to have at least one year outcome data.
Sample size determination:
Table 1: Sample size and its determination, Sekoru Woreda, Jimma zone, Ethiopia: June 2012. View Table 1
Sampling procedure/Technique: In the woreda there are 5 HCs giving TB treatment but only 3 have diagnosis service. One health center started the diagnosis service only before three months before data collection. Thus purposively health facilities providing both diagnosis and treatment services for at least the last two years were included in this study so as to have a one year outcome data.
For expert interview Woreda TB coordinator, 1 clinician from OPD, 1 lab technician, 1 DOTs service provider, one pharmacy professional and head of health facilities were selected purposively from each health center so that rich information can be obtained.
Inclusion criteria:
• Charts of all pulmonary tuberculosis suspects (cough ≥ 2 weeks) with age of ≥ 15-years-old who were diagnosed in the study health centers in the year 2010/2011 for patients' card review
• Information of all PTB patients that were on drug treatment in the study health center from Sep 2010 - June 2012 for TB register review.
• Follow up chart of HIV patients on ART and Pre ART care in 2012.
Data collection feild work: Two data collectors in each study health center and one supervisor for the two health centers were assigned. The total data collector team consisted of 1 principal investigator, 1 supervisor, and 4 data collectors.
Record review and observation of service delivery at TB unit was done by the data collectors. In-depth interview for health professional and inventory of drugs, supplies and other infrastructure was undertaken by the principal investigator. The supervisor was supervising and checking the data collected in both health centers for their consistency and completeness on daily basis and stores in appropriate and secured place.
Data quality and management: Two days training was given for supervisor and the data collectors before the pretest of the data collection tool. The training included briefing the general objective of the study, discussing the data collection tool, and explaining the technique of patient chart review, document review and ways of provider service delivery observation. Data collection tools were prepared after reviewing different relevant literatures. The tools were pre-tested before the data collection at Ascendabo Health Centre which out of the study area to reduce bias from providers. There was also a regular supervision throughout the data collection period. In a daily basis, data was checked for completeness and consistency by the supervisor and principal investigator. The data was first cleaned manually and checked for its completeness and consistency then coded, entered into a computer using SPSS 16.0 for windows. Multiple copies were maintained so as to recover if any problem occurred to the data.
Data analysis: Descriptive analysis was done using SPSS 16.0 for windows and frequencies, percentage, tables and charts were used to present the descriptive result. Data from the quantitative method was supplemented by qualitative data. The qualitative data was organized and analyzed in major thematic areas.
Ethical clearance and approval was first obtained from the Ethical Review Committee of Jimma University. Support letter to the Woreda was also obtained from Health Service Management department. From the Woreda office letters were written to the health centers. In addition, each subject of the study was fully and clearly informed about the aim of the study and the confidentiality of their information. Verbal consent was obtained from each participant involved in the in-depth interview after informing every participant the right to stop at any point, and the right to escape any question. The data collection instruments for the purpose of this study don't constitute personnel identifiers such as respondent's names and other particulars unnecessary for the study. The privacy, anonymity and confidentiality of information obtained from the documents of the patients was kept throughout the whole study process by collecting and analyzing the data using the codes.
In the two health centers 445 cards of patients were identified as having symptoms of cough for greater than or equal to two weeks that makes them eligible for PTB screening. Review of the clients' documents showed that 238 (53.5%) were males and the remaining were females. The mean age of patients was 34.58 (± 15.66 SD) years. Chest examination was performed for 197 (44.3%) of the patients. These patients had at least one or more signs and symptoms of TB as shown by the Figure 1.
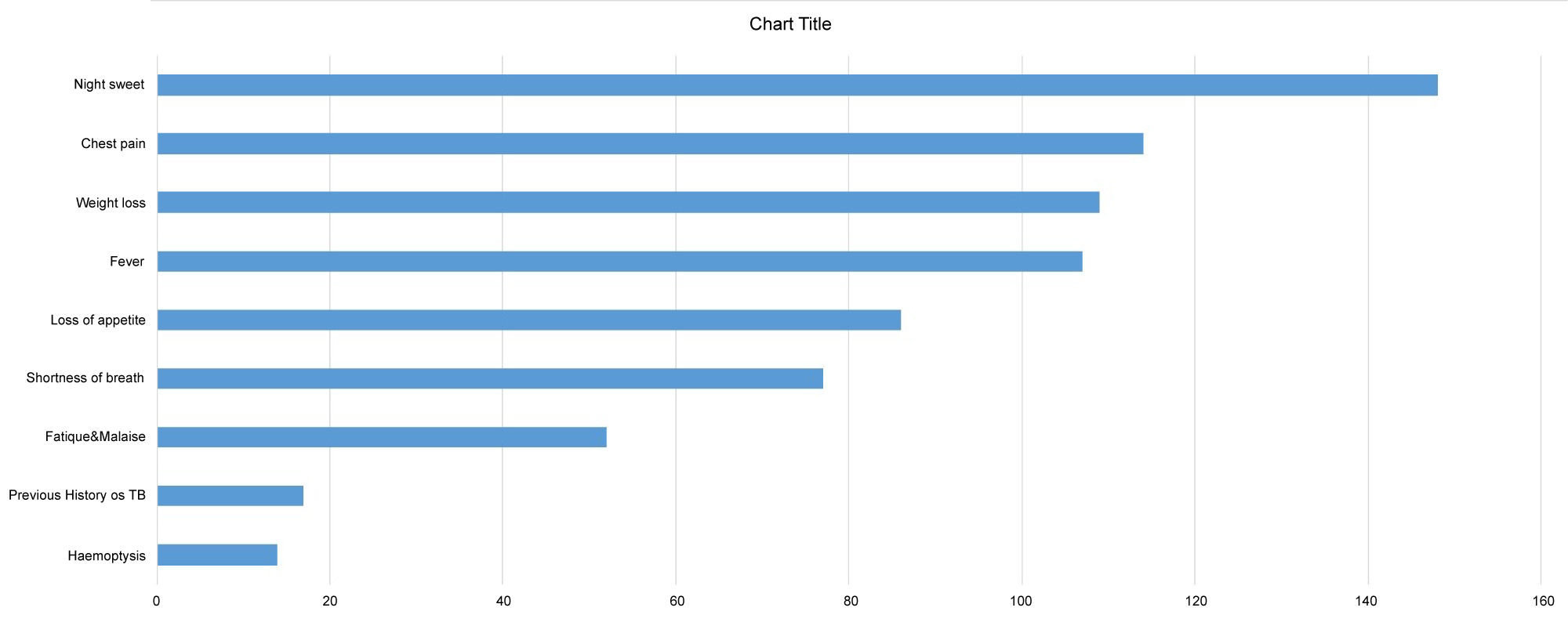 Figure 1: Clinical Presentation of the patients with cough ≥ 2 weeks in Sekoru and Deneba health centers, Sekoru Woreda, Jimma Zone, Ethiopia: June 2012.
View Figure 1
Figure 1: Clinical Presentation of the patients with cough ≥ 2 weeks in Sekoru and Deneba health centers, Sekoru Woreda, Jimma Zone, Ethiopia: June 2012.
View Figure 1
From the total documents showing patients with cough of greater than or equal to 2 weeks and other symptoms suggestive of TB, 263 (59.1%) were sent to laboratory for sputum exam and the result of sputum exam was registered for only 209 (47%) of the patients. 29 (6.5%) were diagnosed as smear negative PTB and 60 (13.5%) patients were diagnosed as smear positive PTB (Figure 2).
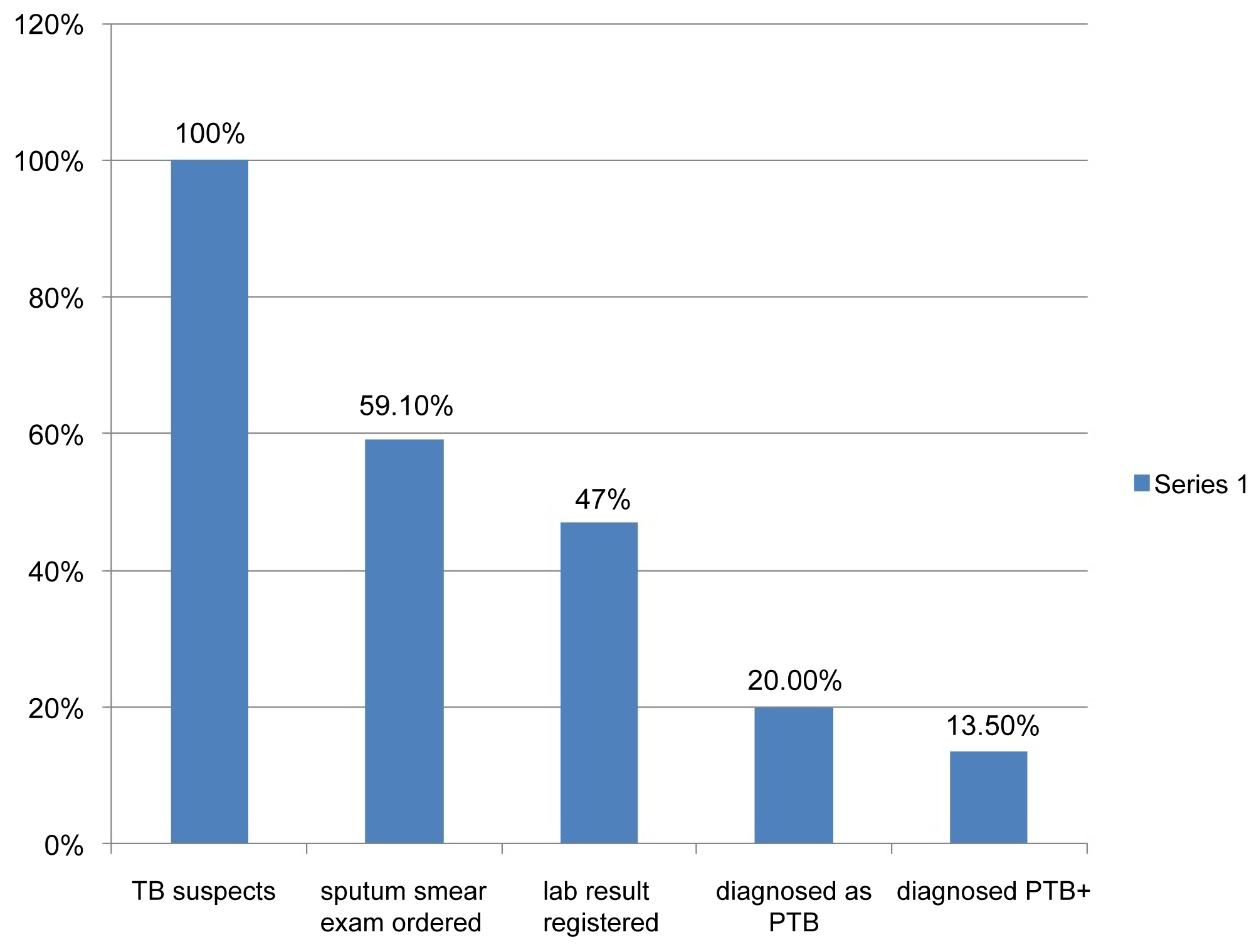 Figure 2: Diagnostic characteristics of patients that visited OPD of Sekoru and Deneba HCs, Sekoru Woreda, Jimma zone, Ethiopia, June 2012.
View Figure 2
Figure 2: Diagnostic characteristics of patients that visited OPD of Sekoru and Deneba HCs, Sekoru Woreda, Jimma zone, Ethiopia, June 2012.
View Figure 2
Among 60 patients who were diagnosed as smear-positive PTB, 54 (90%) were properly diagnosed based on national and 6 (10%) were not diagnosed according to national diagnostic algorithm (Table 2).
Table 2: Results of diagnostic review among patients diagnosed as Smear positive PTB in Sekoru and Deneba HCs, Sekoru woreda, Jimma zone, Ethiopia: June 2012. View Table 2
Of the patients who were diagnosed as smear-Negative PTB, none of them were diagnosed according to national diagnostic algorithm. Here patients diagnosed with 3 criteria (3 initial sputum Neg+no response to antibiotic+repeat sputum negative) were classified as an incorrect diagnosis as the guidelines puts one additional criteria that is chest X-ray. There was no X-ray in the health center but they could have referred to jimma for chest X-ray so as to confirm as smear negative pulmonary TB (Table 3).
Table 3: Results of diagnostic review among patients diagnosed as Smear negative PTB in Sekoru and Deneba HCs, Sekoru woreda, Jimma zone, Ethiopia: June 2012. View Table 3
For smear negative PTB diagnosis to be correct, there should be X-ray before the health care provider decides it in addition to the three criteria that are presented in the above Table 3.
Follow up chart of patients with HIV infection either on pre-ART care or ART treatment in 2012 were also reviewed to see if they were screened for active PTB during their most recent visit. Among patients who were on pre-ART care and on ART treatment, 41.5% and 82.6% were clinically screened for PTB during their most recent visit to the clinic respectively. Table 4 shows summary of this information.
Table 4: TB Screening among patients on Pre-ART and ART, Sekoru Woreda, Jimma zone, Ethiopia: June 2012. View Table 4
In in-depth interview with heads of health centers about problems related to compliance of health workers to guidelines in diagnosing TB, they reported that clinicians sometimes do not consider detail signs and symptoms of TB correctly where they may miss TB cases. One of the health providers shared his experience on when to suspect a patient for TB also said "previously we suspect a patient only if he/she came with cardinal signs like cough and upper respiratory tract problems. So a lot of TB patients may have been missed. The health providers may not have been aware of this but now we have started to screen for cough every patient that came for any case".
One expert reported that deviation from standard guidelines during diagnosis can also occurs in the lab where proper amount of sputum for screening may not be taken because of the provider/patient factor. Gap in the skill of lab professionals was also raised as another factor for the non compliance to the guidelines. He added "This is because, in quality control usually what they confirm here as negative becomes positive when taken to regional lab".
In response to their suggestion on how to tackle these problems, they raised that health professionals should be updated through training in order to ensure proper screening for cough and other symptoms of TB to every patient visiting the HC. NTBL guideline, IEC materials, the necessary drugs and reagents with their quality should also be fulfilled.
A treatment review was made for 117 charts of Pulmonary TB patients, who completed anti TB treatment between September 2010 and June 2012. Of these patients that completed their treatment in that period, 103 (88%) were smear positive PTB and 14 (12%) were smear negative PTB.
For 96.1% of patients correct drugs were prescribed in both the intensive and continuous phases. However, correct dose of drugs were prescribed for 84.5% in both intensive and continuation phases of treatment.
Weight at two months were measured for 102 (87.2%) of the PTB patient. The mean weight of these patients was 44.1 (± 8.8 SD).
From the total 103 sputum smear positive patient, sputum conversion test was done to 87.5% at the end of two months, to 84.8% at the end of five month, and to 79.3% at the end of sixth/seventh months. Name of the contact person was written in 97.4% patients, but the full address is not written for almost all contact persons of the patients.
Among the patients' records that were reviewed from the TB register, HIV test was done for 113 (96.6%). The result of the test was non reactive for 108 (95.6%) and reactive for 5 (4.4%).
Regarding the diagnostic category of the patients that were on treatment, majority of the patients (97.4%) were new followed by relapse (1.7%).
Treatment outcome of majority (76.1%) of the patients was cured while for 3.4% it was not recorded. The treatment success rate, (those cured + treatment completed) was 101 (86.4%) (Table 5).
Table 5: Diagnostic category and treatment outcome of Pulmonary Tuberculosis patients that were on treatment, Sekoru Woreda, Jimma Zone, Ethiopia: June 2012. View Table 5
Both health centers had separate TB treatment unit and water supply was present in Deneba HC only. There was no waiting area for the patients near the TB unit in both of the HCs. In Both of the study health HCs treatment service was provided 5 days a week and do not provide in the weekend. each of the HCs had at least one functional AFB microscope and they reported that AFB examination had been performed on daily basis.
At the time of the survey, only two types of anti-TB drugs (RHZE and RH) were available in both HCs. There was no stock out for either of them during the last six months. Nevertheless other two types of anti-TB drugs (EH and E) were found expired in Sekoru HC. Through in-depth interview a provider in the TB unit said, these are the two types of drugs majority of the patients use.
There was no shortage of lab reagents and no stock out in the last six months in both of the HCs. Also, it is confirmed that during the study period there was no expired lab reagents. But the AFB service was stopped for 2 months due to problem in the quality of reagents especially carbol fuchsine. The providers said, the problem could be related to concentration of the reagent or it might have been expired. "We don't know the exact problem because we received prepared reagent from the regional lab. We have reported about the problem to the regional lab, Woreda health office, and others concerned bodies".
TB diagnosis algorithm, Standard operating procedure for TB laboratory diagnosis, Treatment regimen and sputum follow up schedule were posted in Sekoru HC but not in Deneba HC. Copies of Tuberculosis and Leprosy Control Program (TLCP) manual were available only with heads of both health centers. There was no functional weighing scale in the TB clinics of both HCs. Lab TB register was available in Sekoru HC but not in Deneba HC.
Most of the health workers interviewed had ≥ 2 years experience. providers in TB clinic of both health centers had taken TB DOTS training in the year 2012. Concerning training of overall health professionals involved in TB diagnosis and treatment 5 out of 9 and 2 out of 6 had taken the TB DOTS training in Sekoru and Deneba health centers respectively. That means on average 46% of health workers involved in the diagnosis and treatment had training on DOTS in the past two years.
Shortage of guidelines was reported by the providers. They reported that they don't get the manuals. Moreover, during the study period there were not guidelines observed in any of the departments of the HCs and with any of the workers in the HCs.
Deneba health center started to use bin and stock card for controlling the expiry and balance of drugs and reagents but in Sekoru HC still not started (Table 6).
Table 6: Summary of availability of drugs and reagents for diagnosis and treatment in Sekoru and Deneba HC, Sekoru Woreda, Jimma zone, Ethiopia: June 2012. View Table 6
The providers in the TB clinic said there is supervision from the woreda but not on regular bases. For example there was no supervision in the last quarter, and usually when they came for supervision, they do not provide written feedback. They only check for registers, reporting formats and ask if there are problems to be solved. The woreda focal person reported that they have a plan to conduct supervision on quarterly basis but sometimes it is missed due to work load and lack of budget and transportation. It is also reported that heads of the health centers do not supervise the TB unit on regular basis. If any, the supervision was conducted without schedule and it was not supporting us with the provision of written feedback.
The primary target of DOTS strategy is to detect at least 70% of smear-positive PTB cases who are the major sources of tuberculosis transmission. Accurate diagnosis of pulmonary tuberculosis is a cornerstone of tuberculosis control. This may be achieved through compliance to national guidelines. Low detection of smear positive and over diagnosis of smear negative PTB which occur mainly due to deviation from standards has been persistent problem over the years in Ethiopia [9].
This study revealed that only 263 (59.1%) of patients with cough of two or more weeks were sent to the laboratory for AFB, indicating that there are chances for missing positive PTB cases. This can increase the burden of the disease on the community as infectious PTB can easily be transmitted by inhalation of infected droplet nuclei, which are discharged in the air when somebody with untreated sputum positive pulmonary TB coughs or sneezes. Infectious PTB patients can transmit the disease to persons living in the same household, or who otherwise are in frequent and close contact with them. Thus the objective of case finding which is mainly cutting the chain of TB transmission may have been missed.
It is also indicated in the TLCP manual (2008), all patients with chronic cough should be referred as suspects by the clinician and should be sent to Laboratory for sputum examination [11]. In this study about 41% of patients with cough of greater than or equal to two weeks returned home without having sputum smear microscopy.
If positivity rate holds the same among suspects who received sputum microscopy and who don't, the finding of this study indicates that about 42 PTB + patients missed the opportunity of being diagnosed during their visit to the Health Centers. Such delays are critical as infected individuals remain untreated in the community, providing more opportunities for transmission of the disease and adversely affecting the epidemic.
Effective management of TB involves early and accurate diagnosis, and appropriate treatment of patients to reduce transmission, morbidity, mortality and development of drug resistance. Thus, once patients come in contact with a health facility, prompt diagnosis of TB and subsequent laboratory confirmation should be performed, which in turn depends on the type of diagnostics available and the skills of the professionals. Early detection and effective treatment are key strategies to control TB. However, this could be achieved only if the health system detects TB patients within a reasonable time once TB patients report it. In this process, if something goes wrong, then patients may remain undetected leading to more severe disease manifestations in the individual, delayed initiation of treatment with high morbidity and mortality as well as continued disease transmission in the community. This could pose a big challenge in tuberculosis control, as someone with infectious TB can transmit the disease to 10-15 people in a single year [12].
Based on this, the finding of this study shows that in a year about 420-630 people can be affected in the study Woreda because of these missed patients. This is probably due to non adherence to diagnostic algorithms. This study finding was similar to the study report of Burkina Faso (2001) which revealed that only 66% of patients with chronic cough that visited health facilities had been referred for smear exam [13]. Cross-sectional study done at Afar region of Ethiopia also showed that about 70% of TB patients were diagnosed only after their second or third visit [14].
Clinicians must be mindful of TB as a possible diagnosis for symptomatic people presenting themselves to health facilities, and they must be able to recognize a TB "suspect" (someone with pulmonary symptoms, including prolonged cough). Then they must think to order the appropriate examinations (i.e., sputum smear examination with or without chest radiograph). The proportion of suspects who are found to be smear positive provide evidence that health facilities are making an effort in terms of case finding. Persons suspected of having pulmonary TB should be fast-tracked for rapid diagnosis and expedited services. Turn-around time for sputum AFB (acid-fast bacillus) smear results should be no more than 24 hours [15].
In this study, among the suspects only for 47% of the patients was sputum exam result registered. Of the total suspects 89 (20%) were diagnosed as having PTB of whom 29 were diagnosed as smear negative PTB and 60 were diagnosed as smear positive PTB. That means among from the total 89 cases of PTB, smear positive and smear negative PTB were 67.4% and 32.6% respectively. This is not in agreement with the national guide line of FMOH (2008), which says smear-positive PTB comprises 75-80% of PTB and smear-negative comprises 20-25% of PTB [11].
In this study the suspect positivity rate which is calculated as:
{no. of TB suspects found to be smear positive /no. of TB suspects identified clinically* 100}
was 13.5%. This indicator measures case detection effort among health staff. Increased case detection effort should lead to increased case detection. According to WHO, the target for this indicator should be around 10% and a value higher than 10% may indicate that clinicians are not well aware of TB symptoms and only send those patients at advanced stages of TB for sputum examination [15]. Thus, our finding on low rate of sputum microscopy screening among TB suspects explains the higher smear positivity rate observed in the study health centers.
This was lower compared to report from Burkinafaso in 2001, for which the positive diagnosis was made in 22.5% of the suspects [13].
From our study it is evident that patients can be missed at different levels of care. For example, a lot of patients that had symptoms of cough were not sent to lab. Again, among those sent for AFB, lab result was not recorded for a large proportion of patients. Study done in Burkinafaso in 2001 on the PTB case detection also showed that the losses of cases occur at each of the stages leading to the diagnosis of TB [13].
In this study, the diagnosis of smear positive PTB patients was considered as correct (i.e. Cases with at least 2 initial positive sputum smears or Cases with at least 1 initial and 1 repeat positive sputum smears) for 54 (90%) of the patients and the diagnostic procedure in smear negative PTB was considered incorrect for all of the patients. This may be due to lack of motivation and non adherence of the providers to diagnostic algorithm. Correct diagnosis among smear positive PTB patients in this study is found to be better (90%) than that reported from districts of Tigray region (78.6%). Whereas, diagnosis of smear-negative PTB patients is found to be much lower than the same study (31%) [9].
This may be due to non-compliance of the health professionals to the guidelines in the diagnosis of TB, or due to lack of training of the health professionals involved in the diagnosis. In this study, only 44.5% of health professionals had taken TB DOTS training in the past 2 years. This was comparable with the finding of another study which show that TB care was provided by 44% of untrained health workers [10].
One of the objectives of TB control program in Ethiopia is to reduce burden of TB among people living with HIV; and Reduce HIV burden among TB patients. Thus all HIV patients should be screened for TB in each of their visit and also all TB suspects should be screened for HIV.
In this study, among patients that were on pre-ART care, 41.5% were screened and among those on ART treatment 82.6% were clinically screened for TB. The regular screening for TB among HIV-positive clients, at every stage of the disease, is one key TB/HIV collaborative activity, with the aim to reduce the burden of TB in PLWH. Similarly all TB suspects should be screened for HIV to reduce the burden of HIV and AIDS among TB patients [11].
In study done in Oromia region the prevalence of HIV infection was significantly associated with the incidence of TB. Similar associations were also seen for the prevalence of HIV infection with the incidence of smear positive tuberculosis, smear negative tuberculosis and extra-pulmonary tuberculosis [16].
Heads of labs reported that internal quality control is done by them by rechecking what one has done by the other. External quality control is also done by the regional health bureau. In the Sekoru they maintain all positive AFB slides and 25% of the negative slides. Whereas in Deneba they maintain only 5 positive and 5 negative AFB slides for regional lab. This contradicts what is in TLCP manual that says the laboratory should keep all positive and 25% of negative slides to facilitate the Quality Assurance procedures [11].
Even though the ordered drug regimen and the category were found to be correct for most (96.1%) of the patients, it was observed that about 16% of PTB patients were prescribed incorrect dose. Prompt, accurate diagnosis and effective treatment are not only essential for good patient care but also they are key elements in the public health response to tuberculosis and the cornerstone of tuberculosis control [7]. Possible reasons as observed from experts were non-adherence to treatment algorithm, and absence of guidelines.
According to the guideline of FMOH 2008, Patients must receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period of time [11].
The finding of this study was better than study done at Jimma zone in which treatment regimen conformed to guidelines in 64.7% of cases during the initial phase of therapy and 46.9% during the continuation phase [8].
Prescribing inappropriate medicines for TB patients has numerous public health implications. This includes: Treatment failure, increased morbidity and mortality rate, and development of drug resistant strain of TB infections that are more expensive and more difficult to treat [17]. Thus the relapse cases in this study may be related to the wrong drug or dose prescribed by the providers.
In this study from the smear positive PTB patients who were on treatment and eligible for sputum test, sputum follow up test was done at the end of 2nd, 5th and 7th 'month, for 84 (87.5%), 78 (84.8) and 73 (79.3) respectively. But the guide line recommend, as routine, all sputum-positive patients on SCC must have one sputum specimen examined at the end of the 2nd, 5th and 7th 'month, and this is extremely important as a tool to monitor the effectiveness of treatment. This was similar to study done in Jimma zone in which over all registration of sputum smear microscopy declined from the 1st smear to the last smear [8].
As shown in the result, the treatment outcome for majority of the patients was cured (76.1%) followed by the treatment completion (10.3%) and the death was 4.3%. There was no default reported and treatment outcome was not written for 3.4% among those reported as cured sputum exam was not done for 10 patients which shows misclassification of outcome of the treatment. According to the national guideline 2008, if the patient completes the treatment but sputum exam not done at seventh month it should be reported as treatment competition. The treatment success rate, (those cured + treatment completed) was 101 (86.4%).
In similar study done in Jimma zone the treatment outcome, was cured for 50.6%, completed for 18.5% and the treatment success rate was 69.2% [8]. The difference in the treatment success rate in the two studies may be due to misclassification of treatment outcome in the Sekoru woreda as patients for whom sputum exam was not done in their 7th month were categorized as cured.
Though 97.4% of the patients' contact persons were written, full address was not written for all of the contact persons. According to the standard HMIS formats name of the contact person, his kebele and the house no. should be written so as to search the patient during defaults. The finding of this study was relatively better than the study done in the Jimma zone. In that study address of patient and name of contact person were not registered for 92 (23.1%) and 70 (17.5%) of cases, respectively.
Concerning availability of resources there was separate TB clinic in both health centers and TB clinic of Deneba HC had tap water in the TB clinic. Waiting area near TB clinic for the patients was not available in both health centers. Treatment service was not available in the weekend in both health centers.
In the study conducted in Jimma zone on 10 health facilities, the TB drugs were available on weekend in only 1 of the Health facilities. 5 (50.0%) of the health facilities had no waiting area for patients or not sufficient for the patients load [8].
In the other study done on Quality of tuberculosis care in eight Ethiopian districts 71% of the health facilities delivering TB care on a daily basis and others gave only specific days of the week [10].
Although the availability of resources was found to be fair in this study based on pre set criteria; there was problem in quality of reagents that resulted interruption of diagnosis service in Sekoru health center.
In the in depth interview the heads of labs in both Sekoru and Deneba health center said there is no shortage and stock out of reagents but the problem in the quality of reagents frequently occur. Carbol fuchsine is not sensitive and results every sputum as positive. The AFB service was stopped in Sekoru health center and he said we reported the problem to the regional lab. In Deneba HC the head of lab said we are waiting more time than the standard to obtain the result because of problem in this reagent (carbol fuchsine).
Another problem identified was there was no category two drugs in both health centers and category II patients were given the same drugs as that of I and III. This may have resulted relapse of the disease in some patients as correct drugs and doses are very important for effective management of TB. The NTP guideline recommended that all types of anti-TB drugs and reagents to be available for at least one month of stock [11]. Expired Ethambutol and EH were also observed in Sekoru HC during the data collection. The reason given by the provider was that EH is changed by RH.
There is under diagnosis of TB in patients that come to the health centers but once patients are diagnosed, there is good treatment service and high likelihood of getting cured or successfully completing the treatment. A lot remains to be done to improve the service delivery and process of case findings specifically for negative PTB patients so as to reach the performance targets set in the TBL guidelines. This could be ensured through strict adherence to the screening guidelines for cough greater than 2 weeks and all HIV positive patients.
Thus, health workers should be encouraged to adhere to the national guidelines, Quality of reagents should be maintained and all categories of anti TB drugs should be availed all times. Training, Supervision and follow up of health workers should also be strengthened.