Aim: To study the joint management of paediatric trauma by adult and paediatric surgeons, in an adult trauma system with an embedded paediatric component.
Materials and methods: We looked at the trauma registry data from January 2019 to June 2020 at Sheikh Khalifa Medical City in Ajman, United Arab Emirates (UAE). The medical records, radiology findings and post discharge outpatients visits records were studied. We had total of 137 paediatric trauma patients (excluding burns). These ages range was between 6 weeks to 16 years. There were 41 female patients.
Results: Out of a total of 744 trauma patients who required admission for management of their trauma at our institution, 137 (18%) were paediatric trauma patients. The common mode of injuries included; road traffic accidents (RTA) and pedestrians hit by car (44%), falls (42%), heavy object related (11%), and assaults (2%). Trauma levels at presentation included; four level 1 trauma, 81 Level 2 and 50 level 3 patients. One in four had injuries to more than one organ systems.
There was 1 death as a result of fall from a height and many life threatening injuries in our cohort. One child was brought dead on arrival following a fall from height. All the other children were managed in a multidisciplinary manner with various teams getting involved based on necessity of their expertise. A review of all in patient records confirmed appropriate management of these paediatric trauma patients with majority of children being discharged between 24-48 hours.
Conclusion: We conclude that Paediatric trauma can be managed by the adult trauma surgeons in an adult trauma system with the availability and back up of paediatric surgery expertise in a non specialised paediatric trauma centre. Strict adherence to the basic advanced paediatric and adult trauma life support (APLS and ATLS) principles is, however, mandatory.
Our series shows high incidence of road traffic and falls related injuries. Community education and safety campaigns will certainly be beneficial in reducing the number of such injuries.
Paediatric trauma is the leading cause of death in children over the age of one year [1] and traumatic brain injury is the most common mode of death or disability in these children [2]. This is true for the developed as well as the developing world. The rapid economic progression and cheap fuel prices in the UAE has resulted in the use of a large number of vehicles. Many of these include sports utility and 4 wheel drive vehicles. Because of their mere height and the small size of subject (children), the impact very often results in serious chest or abdominal trauma or running over of the child. Additional factors which contribute to these injuries are the lack of sense of judgement in children when on the roads or when crossing roads [3]. Grivna, et al. reported 103.7 deaths per year in the UAE between 2000-2008 which equated to a mortality of 13.6/100,000 population [4].
The emotional and the physical disability associated with the whole incident may be lifelong in some children or their families. Majority of the deaths in children occur at the scene or very early on after the trauma [5,6]. Treatment after severe trauma, thus, is always time critical and hence the importance of management by appropriately trained team at the right facility. There is enough evidence that children with complex trauma who are managed in dedicated trauma centres will have better outcomes including survival [7].
United Arab Emirates (UAE) has a high incidence of trauma including paediatric trauma. Though the trauma related financial implications in the UAE are unknown but what we know for sure is that appropriate care in the "Golden Hour" following the trauma results in the best possible outcome for the child. This then results in significant decrease in the morbidity and mortality that is associated with severe trauma and helps reduce the financial burden on any healthcare system.
According to Batt, et al. trauma is the second major cause of deaths in UAE and accounts for about 20% of all deaths amongst locals as well as the expatriates. According to the 2018 WHO figures, population of UAE was 9 million. Emiratis form only 11-12% of the total UAE population. However when we look at the paediatric trauma data in our series, Emirati children are highly over represented as they comprise about 44% of all children in our study (Figure 1). Batt, et al. also highlight that road traffic incidents in USA are responsible for 22% of all deaths as compared to 67% of road traffic accident related deaths in Abu Dhabi, the UAE capital [8].
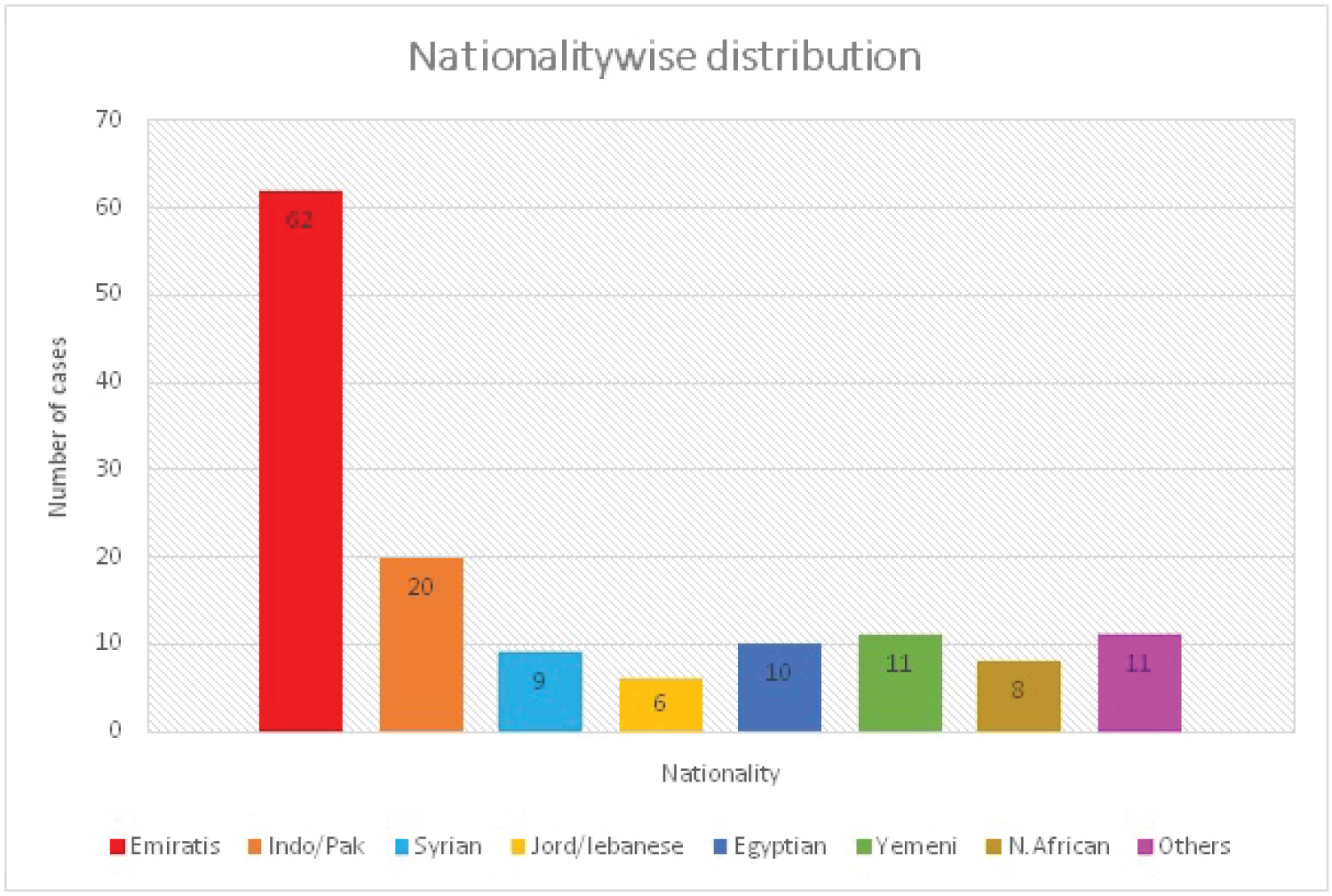 Figure 1: Distribution of cases based on different nationalities. View Figure 1
Figure 1: Distribution of cases based on different nationalities. View Figure 1
A retrospective review of our hospital trauma data between January 2019 to June 2020 was made. Individual case notes of all children who were admitted to Sheikh Khalifa Medical City (SKMCA) in Ajman were reviewed. The radiology images, reports and the treatment received in the ED of all patients in our study were verified.
All children between the ages of 6 weeks to 16 years who were admitted to SKMCA following trauma were included in this study. Children who were observed and discharged from emergency department and those transferred from another unit were excluded. Since we are not a burns unit, all paediatric burns have not been included in this study though we treated many children with first and second degree burns during the study period.
A total of seven hundred and forty four patients required admission through our emergency room for management of their trauma between January 2019 and June 2020. They were classified between level 1 and level 3 injuries based on the adult trauma scoring system.
Out of these there were 137 (18%) paediatric trauma patients (Figure 2). The male to female ratio for children was approximately 2:1 (Figure 3).
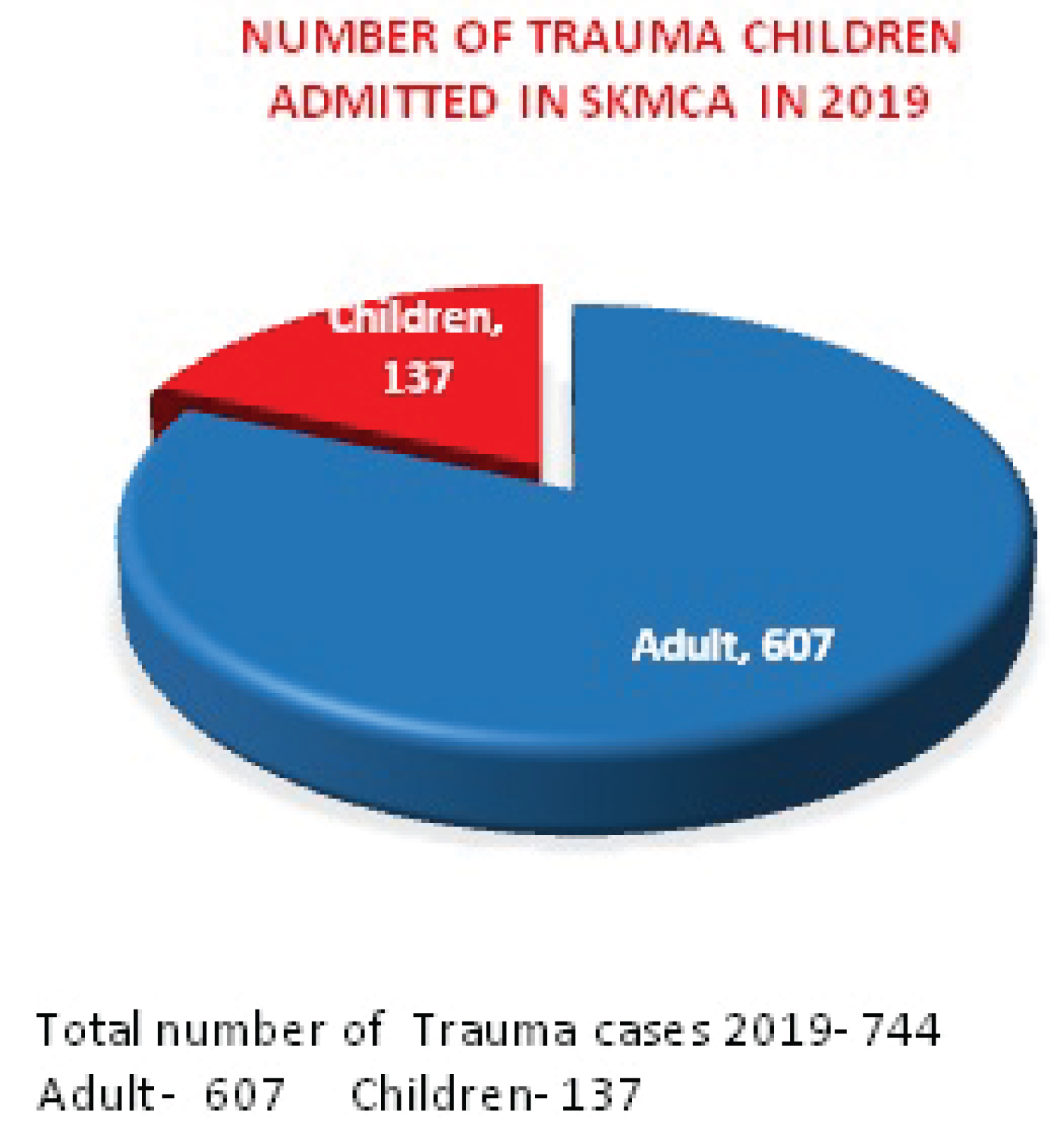 Figure 2: Graph showing Adult vs. Paediatric cases during the study period. View Figure 2
Figure 2: Graph showing Adult vs. Paediatric cases during the study period. View Figure 2
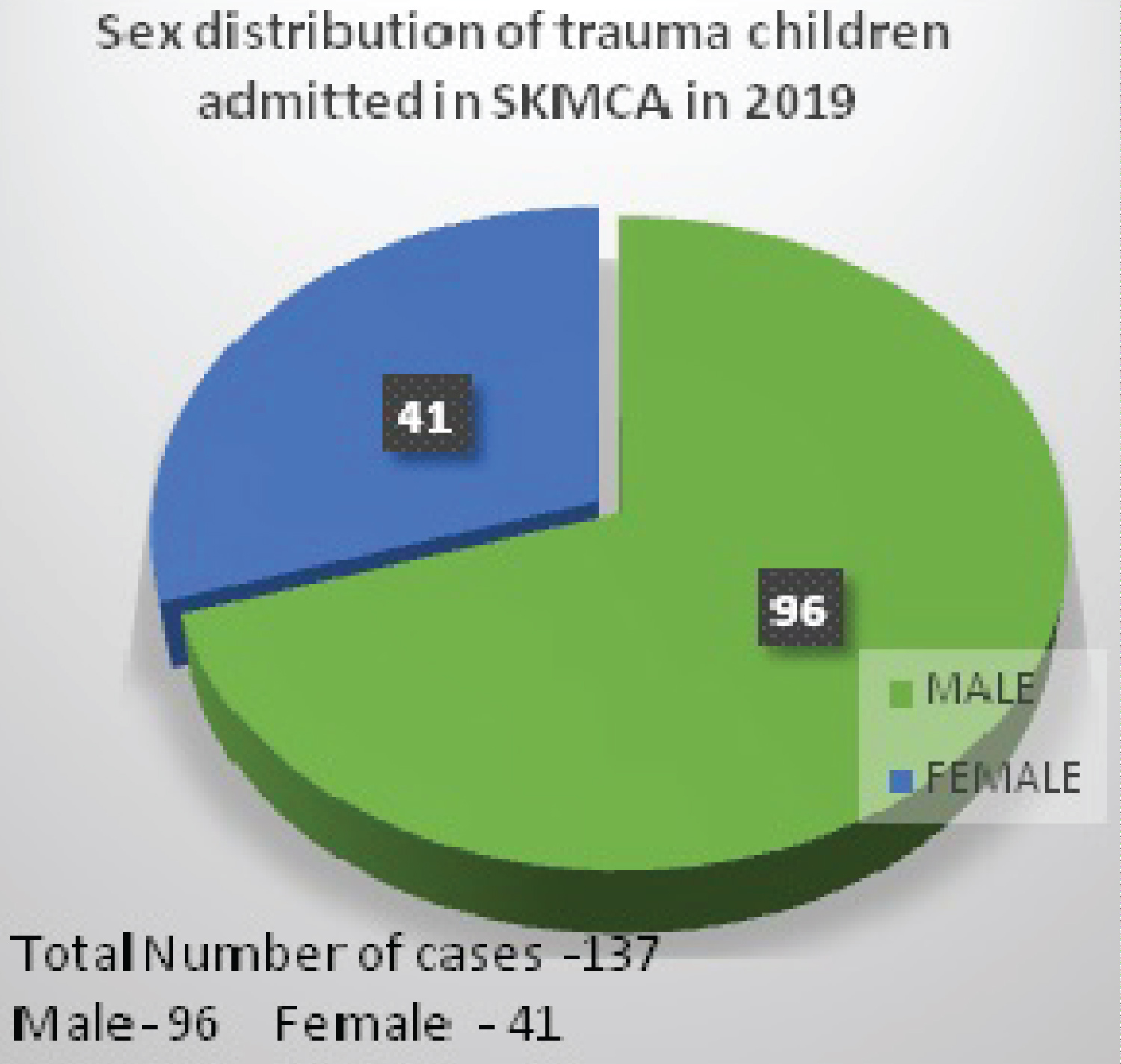 Figure 3: Distribution of Male vs. Female Patients. View Figure 3
Figure 3: Distribution of Male vs. Female Patients. View Figure 3
The age range of the admitted children was between 6 weeks and 16 years. The most common mode of injury was road traffic accidents (44%) followed by falls (42%), heavy object related (11%) and assaults (2%) (Figure 3). Most falls were at home and minor but required admission for observation based on the NICE (National Institute of Clinical Excellence) guidelines. In the head injury cohort, twenty four children required admission with vomiting, drowsiness or loss of consciousness. Another worrying twenty seven had more severe head injuries with one or more of the following features; simple, depressed or extensive intracranial fractures, intracranial bleeds or major orbital fractures. One death following admission and one child who was brought in dead, both, had severe head injuries.
Most of the road traffic accidents were as a result of a pedestrian being hit by a car (Figure 4). Two of these injuries were a result of cars rolling over and another two were a result of a car rolling over a child. The youngest child in our series was a 6-week-old who sustained a skull fracture with an intracranial bleed following a car roll over. One boy with a haematological disorder required emergency splenectomy to control life threatening bleeding following blunt abdominal trauma.
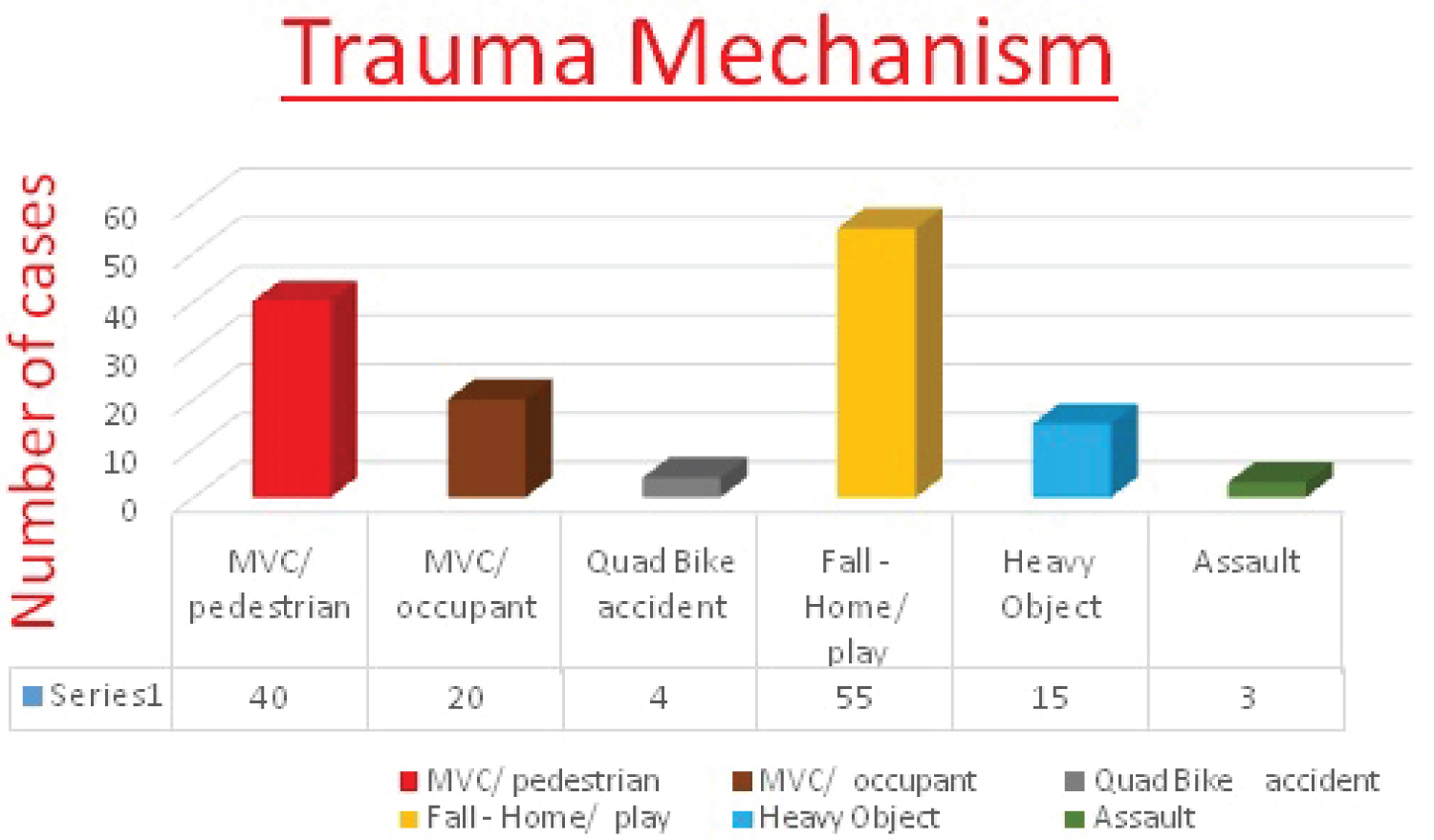 Figure 4: Various mechanisms of Trauma. View Figure 4
Figure 4: Various mechanisms of Trauma. View Figure 4
Some of the injuries were potentially life threatening and included intracranial haemorrhage, pneumothorax, and multiple rib fractures including fracture of bilateral first rib fracture, long bone fractures, spinal fractures and orbital blow out. The injury pattern is demonstrated in the graph below (Figure 5). Many children had more than one system injuries.
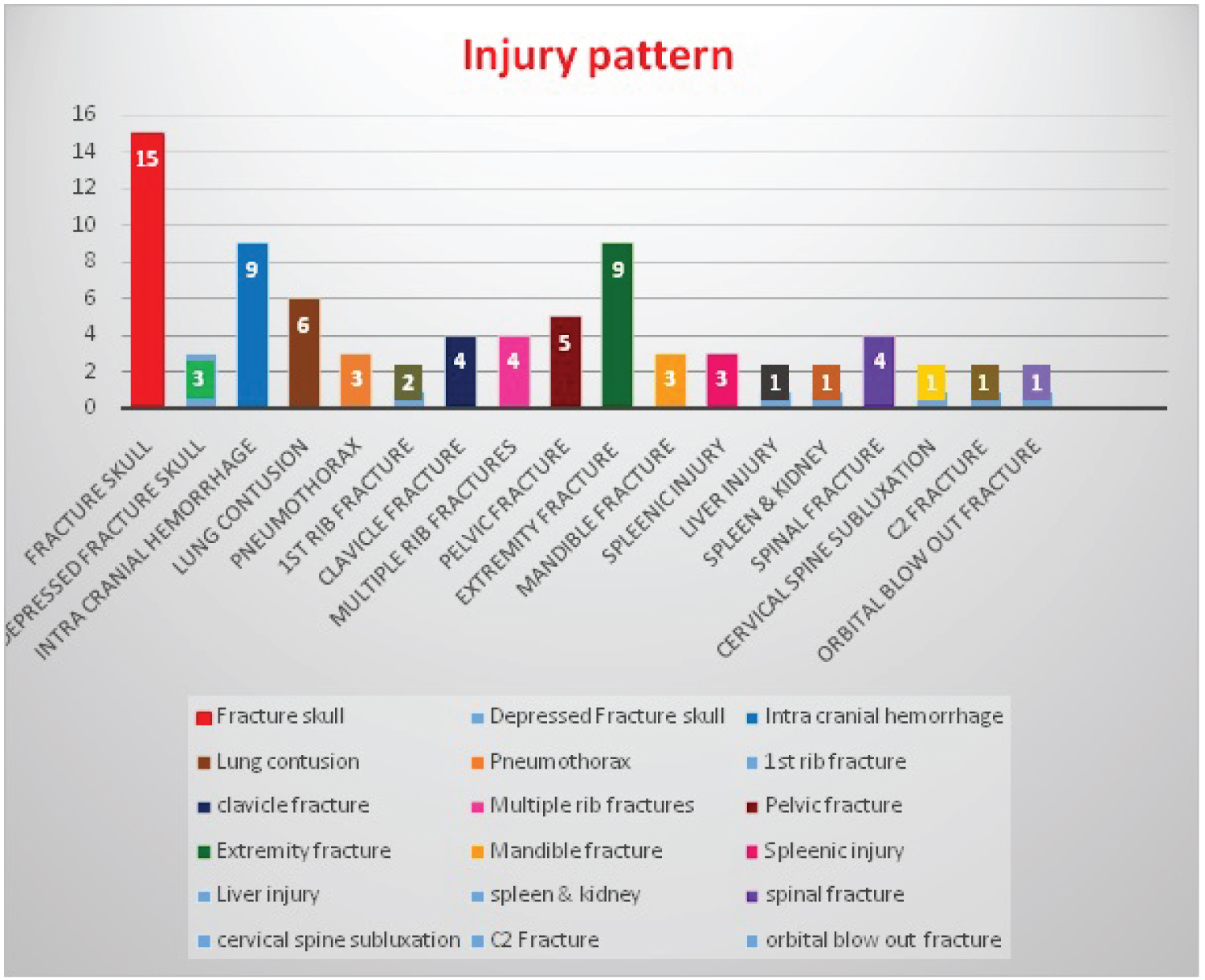 Figure 5: Injury Pattern. View Figure 5
Figure 5: Injury Pattern. View Figure 5
Paediatric trauma requires a specialised group of appropriately trained paediatric emergency department (ED) and/or paediatric surgical doctors for management. In many developed countries and even in those with mature health systems, dedicated paediatric trauma centres are only present in 75% of their tertiary referral units [9-11]. The UAE does not have any dedicated paediatric trauma centre. As most government hospitals take paediatric trauma, this dilutes the volume that some of the smaller centres experience. The ambulance usually takes the child to the nearest government hospital where the level of experience in dealing with paediatric trauma varies and hence may affect the outcome directly.
At SKMCA we have a unique paediatric trauma management approach in place. All cases of paediatric trauma are initially attended by the ED and adult surgery on call teams. They strictly follow the standard ATLS (Advanced Trauma Life Support) and APLS (Advanced Paediatric Life Support) guidelines and standardised trauma protocols. Additional trauma team training is practised regularly. The trauma team training sessions are simulated sessions to train and test various tiers of doctors who are involved in the front line management of trauma.
The adult surgical senior registrar or the ED consultants are the trauma team leaders. The trauma team comprises of a senior general surgeon, ED physician, orthopaedic surgeon, and an anaesthetist along with the nursing leaders. The paediatric surgeons are on call and off site after hours but participate actively with regards to assisting the trauma team in managing the specialised paediatric aspects of the trauma. This way the child is initially received by an able and competent team of doctors who manage each trauma in the exact same pattern every time and hence standardise trauma care in children. The experience of paediatric surgeons then comes in handy when in certain conditions (eg: liver and splenic trauma) principles of management in children differ as compared to adults or where resuscitation fluids and volumes sometimes vary or where analgesia requirement approach and assessment is considerably different in children. The neurosurgeon, paediatrician or paediatric intensive care doctor will also join the team if and when requested.
In our series we have noted that in 18 months, only one hospital in Ajman has seen one hundred and thirty seven paediatric trauma patients that have required in patient admission. The spectrum of injuries has included several life threatening conditions.
What is concerning is that (44%) were motor vehicle related accidents with majority being pedestrians hit by a car. Two injuries resulted from rollover of the cars while in two others the car was reported to have rolled over the children. Moreover, the use of seat belts by children is not commonly practised.
Ajman is a new and young Emirate with a huge expatriate labour population. Many of them are either new drivers or are used to driving on the other side of the road in their countries and may contribute to some of these accidents. The municipal authorities and Police are working round the clock to implement measures to reduce trauma associated morbidity and mortality in the community. These include erection of and road signs and markings, speed control measures and installation of metal railings to restrict pedestrians from crossing those roads with fast moving vehicular traffic. While there is a general expectation that only government authorities are responsible for public safety, it is imperative that the public also reciprocate by obeying and practising the government's advice and instructions.
Injuries resulting from "falls" were the second most common cause of injuries in children in this series. Unfortunately the 2 deaths seen in our series resulted from children who fell from heights. Though majority of falls in our series were minor but our concerns lie with those who fell from significant heights. One child who fell off a horse sustained severe head injury which resulted in permanent disability. Four of our children sustained injuries as result of heavy objects falling on them with three injuries occurring as a result of being caught under heavy metal gates. In theory, some or all of these may have been preventable.
Our established model of trained adult surgeons attending to paediatric trauma as well works nicely for the paediatric patients that present to SKMCA. The adult surgeons see a lot more trauma than paediatric surgeons in general and are usually more confident in management of children with different types of injuries. There are very few specialised and dedicated paediatric trauma centres internationally and because of the low incidence of paediatric trauma in the western world, many paediatric surgeons will have limited experience of dealing with paediatric trauma.
Finally, many UAE centres that receive paediatric trauma have few paediatric surgeons and it is not physically possible for a paediatric surgeon to be available in the hospital 24 hours a day. Based on all of above, following standardised and established guidelines for trauma would result in standard basic treatment for all paediatric patients who attend SKMCA with any kind of trauma irrespective of the time of the day that they attend or which individual doctor treats them.
Whilst a lot of attention is being paid towards management and centralisation of major trauma in children in different parts of the world, it is imperative that equal efforts are put in place towards trauma prevention. The World Health Organization report on injury prevention has clearly documented the benefit of using safety restraints and importance of concentrating on making the roads safe [12]. This was clearly seen in the Australian population where the trauma deaths decreased from 15/100,00 to 6.9/100,000 between 1989 and 1998. During this time, additional injury prevention measures were put in place [13]. Prevention measures are far simpler and have huge financial benefits when compared with the resource utilization in management and rehabilitation of those with complicated trauma. However, despite all the evidence, safety legislations, community education, and high traffic fines, the use of safety belts, booster seats and cushions is very low in the society [4,14-16].
We also strongly believe that active involvement of social workers, legislations directed towards trauma prevention from road traffic accidents and falls and parental and community education at various levels will definitely contribute towards decreasing the incidence of paediatric trauma in the United Arab Emirates. Enforcement of seat belt use, appropriate use of car seats (rear facing children's seats), use of booster cushions and serious consequences for over speeding should be the norm in the society to safe guards the children of UAE. Whilst falls on the roads or in the play grounds do not result in serious injuries but installation of child proof door and window locks and specific height balcony frames can go a long way in minimising falls from heights.
The UAE government is working very hard in collaboration with the police and wider general public to address this issue. Community education including safety lectures in schools is an already established initiative. Considering the large number of expatriates who drive in the UAE, the issuance of driving license procedures are already very stringent and include mandatory driving lessons prior to taking the driving tests. These lessons incorporate traffic safety measures and recognition and interpretation of various traffic signs. Various UAE municipal corporations are also working hard towards establishing road safety measures. A limiting factor here may be the rapid turnover of many of these expatriates but this is being combatted by persistent efforts of the government and police to keep the new comers abreast with the traffic safety measures.
In our study and with the data that we have, we conclude that with the presence of trained ED and general surgery consultants and with strict adherence to standardised trauma management protocols, paediatric trauma can safely be dealt within the adult trauma system with the availability and back up of paediatric surgery expertise. A detailed review of all our patient records has demonstrated satisfactory management of all admitted cases with majority being discharged in 24-48 hours of admission.
Our series has highlighted a high incidence of road traffic and falls related injuries in children and lead us to believe that the causes may be multifactorial. We recommend ongoing community education and safety campaigns throughout the emirate and the country and are confident that these measures will be beneficial in reducing the number of such injuries.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.