Hypertension has reached epidemic proportion among people living with HIV (PLHIV) and this could have a negative bearing on the quality of life and survival of these patients.
The aim of this study was to develop and validate a risk prediction model for incident hypertension among HIV patients on antiretroviral therapy (ART) in Fako Division, South West Region of Cameroon.
A 5-years retrospective cohort study was used to review the records or patient files of 1640 HIV patients enrolled between the years 2013-2015. These files were reviewed in 3 HIV treatment Centers (HTCs) which measured a recorded blood pressure routinely.Data was entered in Excel 2010 and analyzed using stata 13. Log rank test and cox proportional hazard regression were used to identify independent risk factors. The model's accuracy was assessed by the area under the receiver operating characteristic curve (AUC) Statistical significance was set at p < 0.05.
Among 1640 ART-naïve, eligible subjects, 344 (21.0%) were hypertensive at recruitment. The remaining 1296 individuals were then used to develop and validate the model. The derived risk prediction model for hypertension had a sensitivity, specificity, cut-off value and diagnostic accuracy of 80.0%, 60.0%, 404 and 0.701 respectively. Incident hypertension increased significantly (χ2trend< 0.001) with increase in the risk score in the validation dataset.
The proposed risk score prediction model for hypertension had a good diagnostic accuracy and can be used in HTCs to identify patients with a high risk of developing hypertension. This will contribute to efforts in providing clinical decision-making that will improve on the clients' health and quality of life.
Development, Validation, Predictive model, Incident hypertension, Retrospective cohort, HIV, ART, Fako division
AIDS: Acquired Immuno-Deficiency Syndrome; AUC: Area Under the Curve; ART: Anti-retroviral Therapy; COVID-19: Coronavirus Disease 2019; CVDs: Cardiovascular Diseases; HTCs: HIV Treatment Centers; HIV: Human Immunodeficiency Virus; HTN: Hypertension; LMIC: Low- and Middle Income Countries; NCD: Non-Communicable Disease; NPV: Negative Predictive Value; PPV: Positive Predictive Value; PLWH: People Living With HIV; SBP: Systolic Blood Pressure; BMI; Body Mass Index; VL: Viral Load; ROC: Receiver Operating Curve; SWR: South West Region; SSA: Sub-Saharan Africa; UTT; Universal Test and Treat; WHO: World Health Organization
The burden of non-communicable diseases (NCD) and their modifiable risk factors is on the rise in Sub-Saharan Africa (SSA). Among people living with HIV (PLHIV), epidemiological studies have revealed a trend of increasing prevalence of four major risk factors of NCDs; hypertension, hyperglycemia, dyslipidemia and obesity [1-3]. With the increasing availability of antiretroviral therapy (ART), the ageing HIV population is susceptible to traditional risk factors for NCDs. Furthermore, both the HIV virus and prolonged ART use have been associated with dyslipidemia, insulin resistance, and atherosclerosis, interacting with traditional risk factors to increase the risk of NCDs among PLHIV [3,4]. The increased NCDs risk among PLWH has the potential to threaten the success of ART use, causing morbidity, poor quality of life and premature mortality.
In Cameroon, the universal test and treat approach was instituted in 2016. This novel approach requires placing all persons testing positive for HIV on ART irrespective of their immunological and clinical statuses. Since the institution of this novel strategy in Cameroon, very few studies have investigated the epidemiology of NCDs among PLHIV in the context of the universal test and treat strategy. Approximately more than 35 million deaths are caused by non-communicable diseases (NCDs) on an annual basis. Morbidity and mortality due to NCDs contribute significant threat globally on health and economy of individuals, societies and health systems [5,6]. The four main NCDs which are being targeted for control globally are cardiovascular diseases (CVDs), chronic respiratory diseases, cancers and diabetes and the selected NCD risk factors also targeted for control are tobacco use, harmful alcohol use, salt intake, obesity, raised blood pressure, raised blood glucose and diabetes, and physical inactivity [6,7].
The prevalence of HIV in Cameroon was 3.9% in 2015 [8]. The World Health Organization (WHO) estimates for deaths attributed to Non-Communicable Diseases (NCD) in Cameroon was 35.0% in 2018 [9]. The prevalence of HIV is 3.6% and that of hypertension is 31.1% in the South West Region (SWR) of Cameroon [2,8]. The prevalence of hypertension (38.0%) and dyslipidemia (51.0%) in HIV patients on ART have reached epidemic levels in Fako Division, SWR of Cameroon [2,3]. Fako Division as well as the other fast urbanizing divisions in Cameroon is experiencing a double burden of HIV and NCDs. Although evidence from high-income countries is definitive as to the emerging importance of NCDs in PLHIV, there are far fewer data and research advances regarding such conditions in low and middle income countries (LMICs).
Rapid changes in lifestyle, together with a hypertension-prone genetic background in black Africans, are leading to the unfolding of a hypertension epidemic of presumably distinct characteristics from those observed outside the continent [10]. Indeed, age-adjusted prevalence of hypertension in the region have already reached the highest levels in the world with an estimated prevalence of 30% [2,3]. While there is consensus in the field about the increased risk of cardiovascular events among HIV patients, the relation of hypertension with HIV infection and ART remains controversial. Indeed, inconsistent and often contradictory reports of associations between HIV infection, ART exposure, specific antiretroviral drug regimens and HIV-related factors have been successively reported in the literature [11]. Interestingly, some widely used antiretroviral drugs have been linked to renal and cardiovascular adverse effects (i.e. tenofovir disoproxil fumarate [TDF] and nephrotoxicity; abacavir [ABC] and myocardial infarction), but their relevance in the hypertension scenario is not well defined [12]. This degree of uncertainty on the burden and epidemiology of hypertension is even higher for sub-Saharan African HIV populations, where only a limited number of studies have approached the subject from a mostly cross-sectional perspective. Thus, unraveling the epidemiology of hypertension among HIV patients in sub-Saharan Africa stands out as an urgent task, and could potentially set the ground for a more optimal clinical management. In this context, our study aimed to explore the prevalence, incidence and risk factors of hypertension development among adult HIV patients on ART in Fako Division, Cameroon.
The underlying causes of incident hypertension and diabetes among adult HIV patients are not fully known, however accurate prediction of patients at increased risk of hypertension and diabetes could lead to better monitoring, management and a reduction of complications from these conditions. Although very few prediction models for hypertension and diabetes have been developed in high-income countries, they may not be suitable for LMICs because of genetic variability and differences in the availability and the cost of diagnostic tools. It is thus imperative to develop and internally and externally validate a contextually appropriate and low cost risk prediction model for hypertension among HIV patients on ART for use in primary care settings in Cameroon and potentially other LMICs.
For administrative approval, the study protocol was read and approved by South West Regional Delegation of Public Health and heads of the health facilities hosting the HTCs. Ethical clearance (No 5231/FHSIRB_UB/02/2020) was obtained from the Faculty of Health Science Institutional Review Board, University of Buea, Cameroon.
The study was a 5-years retrospective cohort involving the records and patient files of HIV patients receiving ART (2013-2015 cohorts) in Fako Division, SWR of Cameroon.
The study was carried out in 3 high-patient load HIV treatment centers in Fako Division that screen and record blood pressure routinely (Figure 1). These hospitals are specialized HIV treatment centres that provide free anti-retroviral therapy in addition to HIV counseling and testing services. According to the RTG of the Regional Delegation of Public Health for the South West Region report for 2020, a total of 18,000 HIV patients were receiving treatment in Fako Division [13]. Patients report every 1, 3 and 6 months for antiretroviral therapy refill depending on the availability of drugs. The number of HIV patients on ART has seen a hick because most patients have been transferred-in from the highly hit conflict areas to Fako Division which is relatively safer. The patients who attend the facility are of different socio-economic statuses. Information on NCDs is not collected in routine care at the facility during patient visits. Hypertension is sometimes screened for at every clinic visit, diabetes mellitus II, asthma, cardiomyopathy and osteoporosis are usually screened for when a patient complains of certain symptoms during the routine follow up visits. Renal impairment is screened for among patients upon being started on tenofovir based regimen. However, some NCDs are screened for as a result of participation in research projects that require screening for certain ailments/medical conditions.
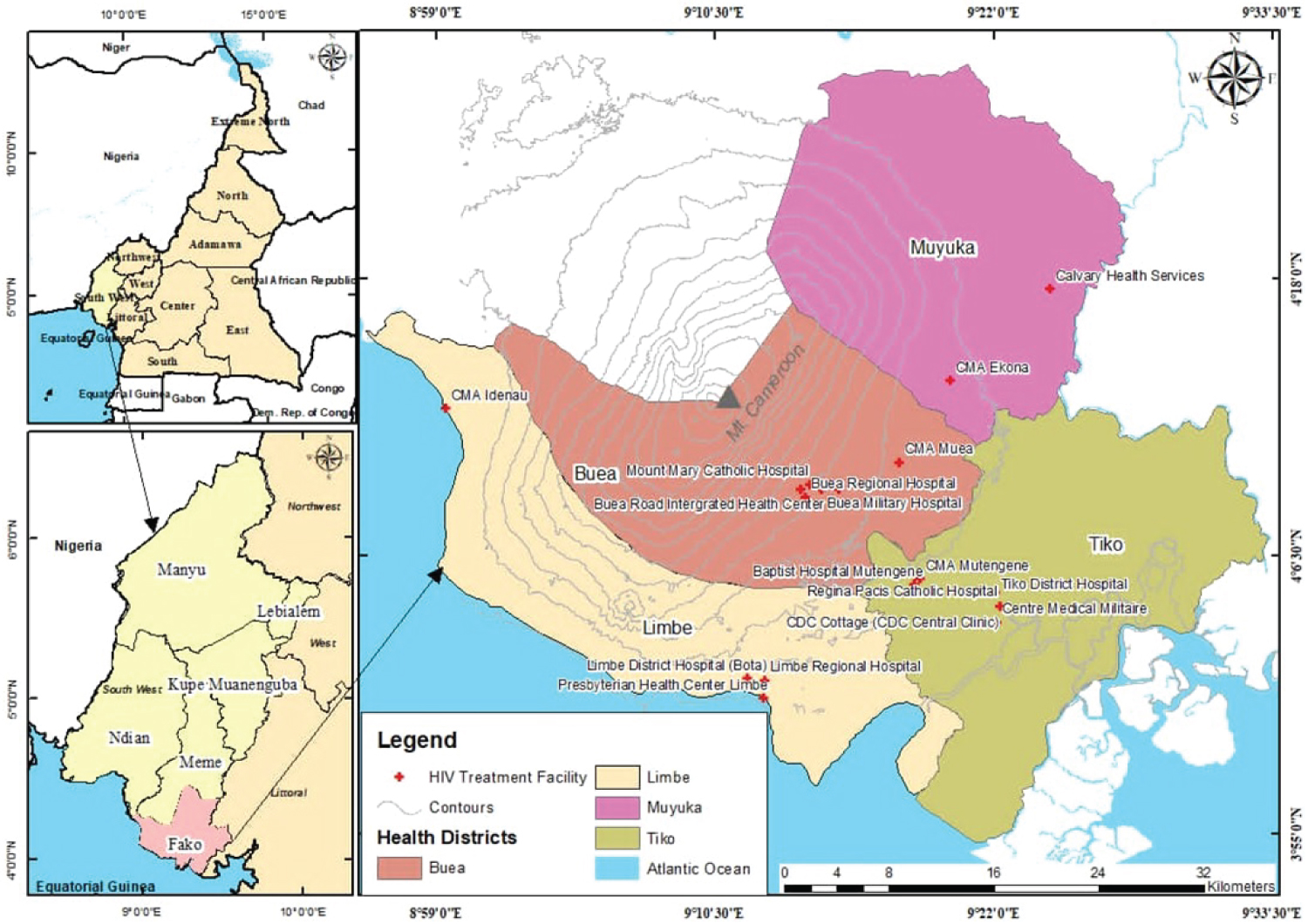 Figure 1: Map of Fako division showing HIV treatment centers.
View Figure 1
Figure 1: Map of Fako division showing HIV treatment centers.
View Figure 1
The targeted population was HIV patients aged ≥ 18 years. Their records and patient files were equally reviewed.
Records and patient files of ART-naive subjects at baseline with at least 2 registered refill or consultation sessions within 6 months since recruitment were included. Only patients aged 18 years and above.
Records and patient files of HIV patients on transit from other healthcare facilities were excluded. Records of pregnant women during the study period were not included in the analysis due to known effects of pregnancy on physiological parameters.
Incident hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg on 2 consecutive visits. Subjects with recorded previous history of hypertension and those with SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg on the first 2 blood pressure measurement sessions within 6 months since registration were classified as hypertensive at baseline.
Demographic, clinical and treatment data was anonymized and extracted from HIV patients' records or booklet. We abstracted data from all adult patients who initiated ART in the Limbe Regional Hospital and the CDC Central Clinic between January 1st, 2013 and December 31st, 2015 and had a minimum of two clinic visits. We obtained data patient data including: Age, gender, height, weight, and blood pressure at each visit, ART regimen history and CD4 T-lymphocyte (CD4) count history. Other laboratory tests, including serum creatinine, glucose and lipid measurements, were not consistently available at the clinic. These were only present for less than 1% of the cohort, and therefore were excluded from this analysis.
At each clinic visit, a trained nurse performed and recorded blood pressure measurements of seated patients using a calibrated aneroid sphygmomanometer, with small (< 21 cm) and normal (22-32 cm) cuff sizes. Patients were seated in a chair and rested for approximately 10 minutes before BP was measured. Following initial BP measurement, patients with SBP > 140 mmHg and/or DBP > 90 mmHg during this screen underwent two repeat BP measurements one minute after. The average of the two later BPs would then be recorded in the patients clinic review form. Weight and height are measured using a stadiometer attached to a weighing scale. Height was measured to the nearest 0.1 cm after removal of shoes. Weight was measured to the nearest kilogram after removal of shoes and heavy clothing. Data were entered directly into an electronic database (Excel spreadsheet).
The blood pressures of the HIV patients were abstracted from their patient files from the time of initiation to exactly 5 years. The blood pressures were monitored and the time of hypertension recorded for participants who developed hypertension. Participants who did not develop hypertension were censored.
The minimum sample size of 549 participants per group was calculated using Epi info 7. The parameters used are shown in the table below (Table 1).
Table 1: Sample size determination for the retrospective study. View Table 1
All data management and statistical analyses was conducted in Stata 13. Univariate analysis was performed to determine the baseline prevalence and incidence of hypertension. Multivariate Cox proportional hazards models was fitted to assess the association of the time to develop hypertension with demographic, clinical and treatment covariates. The analysis was based on the intention to treat approach. The analysis was based on the intention to treat approach. Coefficients (β) and baseline hazard function [h0(t)] were estimated by Cox regression analysis. For each variable significant on Cox regression analysis, a score was calculated by multiplying β by 100 and rounding to the nearest integer. The total score was the sum of scores for each factor. [h0(t)] will be hypertension-free average survival probability at time t (t = 5 years). The probability (P) of hypertension over 5 years was calculated as follows:
P (Hypertension) = 1 - h0(t)exp(score/100)
The predictive power of the risk-score model was evaluated to identify the risk of developing hypertension in the derivation and validation datasets. The aggregated scores were divided into four ranges, and the observed 5-year cumulative incidence of hypertension was compared with predicted risk by chi-square test for trend. The model's accuracy was assessed by the area under the receiver operating characteristic curve (AUC) based on the sum of scores. The AUC performance of the model was compared with that of Framingham. The optimal cut-off AUC was defined as having the maximum combination of sensitivity and specificity. Goodness of fit was assessed by the Hosmer-Lemeshow test. Statistical significance will be set at p-value < 0.05.
Of the 1640 eligible files reviewed, 344 (21.0%) were hypertensive at baseline. The remaining 1296 subjects were randomly assigned to the derivation cohort (n = 648) and the validation cohort (n = 648). The subjects were then followed up for 5 years and 125 developed hypertension in the derivation cohort compared to 115 in the validation cohort (Figure 2).
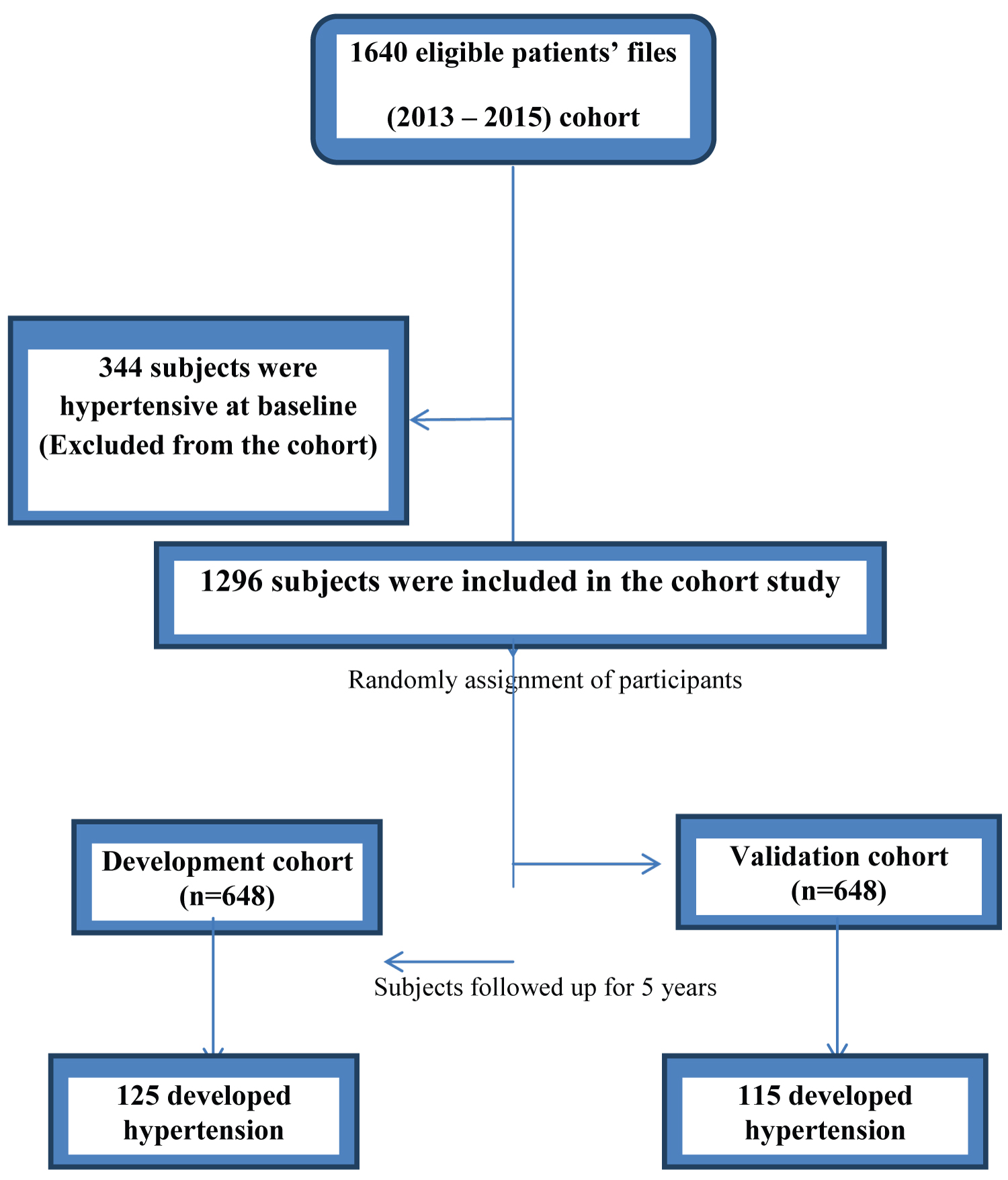 Figure 2: Flow chart of the participants during the retrospective cohort.
View Figure 2
Figure 2: Flow chart of the participants during the retrospective cohort.
View Figure 2
Overall, the incidence density rate of hypertension was estimated at 109.1/1000 person-years:110.6/1000 person-years (n = 125) and 108.9/1000 person-years (n = 115) for the derivation and validation datasets, respectively, with no difference between the datasets (p = 0.522). The baseline characteristics of subjects did not differ between the two datasets (Table 2).
Table 2: Baseline characteristics of subjects in the derivation and validation datasets for developing a model of hypertension among HIV patients on ART in Fako Division. View Table 2
Only baseline BMI, DBP and WHO HIV clinical stage reached statistical significance and were retained in the Cox Proportional regression model with the derivation dataset (Table 3).
Table 3: Risk factors of incident hypertension in the Derivation Dataset. View Table 3
Significant variables were assigned a score based on the regression coefficient, β (Table 2). The total risk score was calculated as follows:
Risk score = 4 BMI (Kg/m2) + 3DBP (mmHg) + 42 WHO HIV Stage
The predictive risk scores of developing hypertension among adult HIV patients on ART during the 5-years follow-up were calculated and ranged from 259- 562 with a mean of 411.1 (SD = 15.3).
The risk scores of each participant alongside the hypertension status were used to generate a receiver operating characteristic curve (ROC) and the area under the curve (AUC). We equally had a table of sensitivity and 1-specificity data. The sensitivity and specificity scores were summed together for each participant and the sum with the highest score was used to extrapolate the sensitivity, specificity and optimal cut off value for the model [14]. Thus, the Sensitivity, Specificity, Optimal cut-off value for the predictive risk-score model and AUC/c-statistic were 80.0%, 60.0%, 404 and 0.701 (95% CI 0.624-0.784) respectively with the derivation dataset (Figure 3). The larger the ROC curve in the upper left corner, the better the discriminatory power of the curve. The AUC was 0.701 (95% CI 0.624-0.784) and was significantly discriminatory given that the lower limit confident interval was greater than 0.5. Using a contingency table, the positive predictive value (PPV) and negative predictive value (NPV) for the development or derivation model was calculated and were 32.4% and 92.6% respectively. The positive and negative likelihood ratios (how much the odds of a disease changes with a given test) were 2.0 and 0.3 respectively (Table 4).
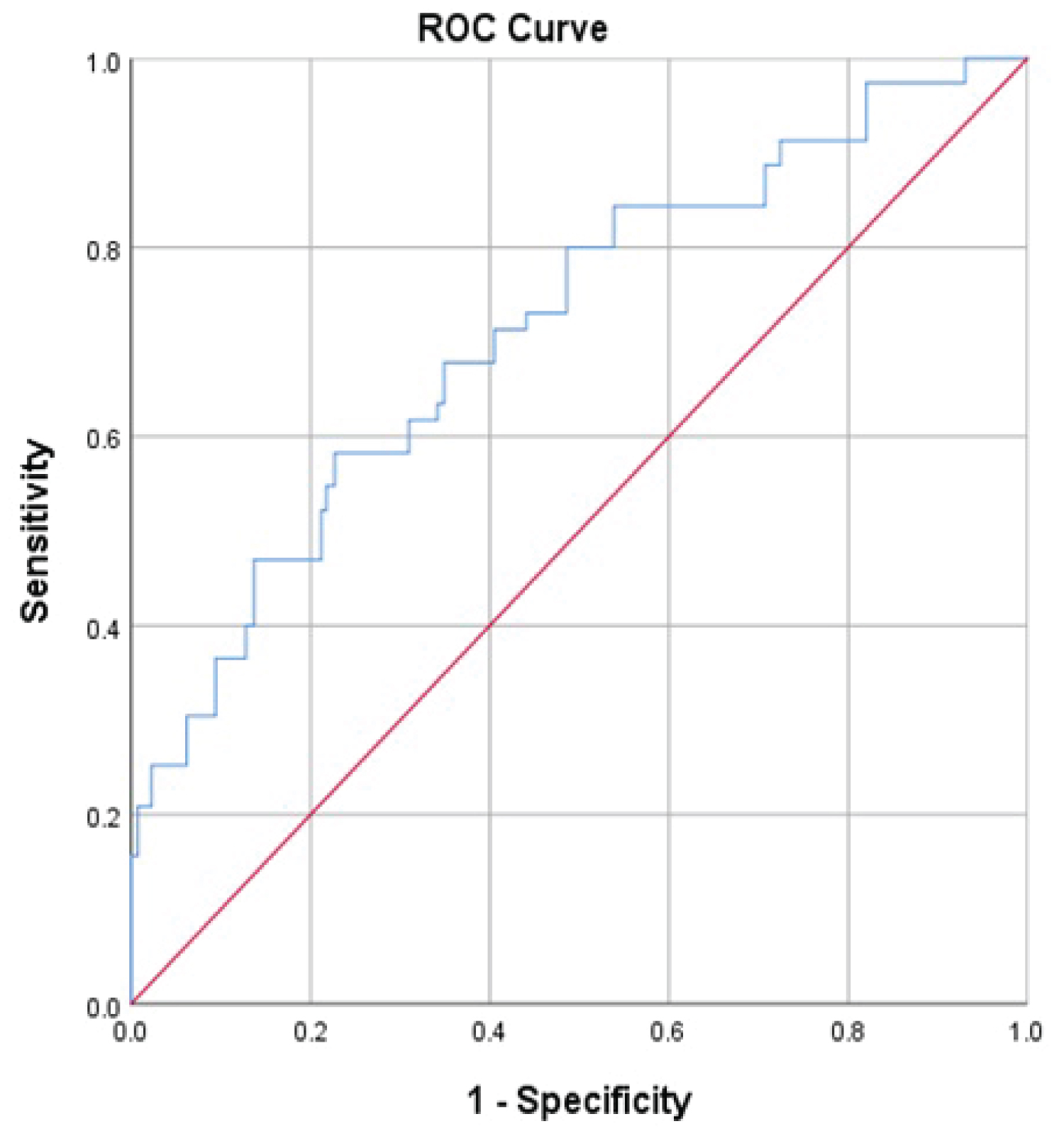 Figure 3: Diagnostic accuracy (AUC or c-statistics) of a risk predictive model for hypertension among HIV patients in Fako Division.
View Figure 3
Figure 3: Diagnostic accuracy (AUC or c-statistics) of a risk predictive model for hypertension among HIV patients in Fako Division.
View Figure 3
Table 4: Sensitivity, Specificity, likelihood ratios and Predictive values of the model. View Table 4
To validate the model, we applied this scoring method to the validation dataset. The aggregated scores were divided into 3 ranges i.e. low, moderate and high risk of hypertension (Table 4). For scores of < 359, 359-459 and > 459, the cumulative incidence of incident hypertension was 9.6%, 16.6% and 32.4%, respectively, in the derivation dataset and 6.7%, 13.4% and 34.2%, respectively, in the validation dataset. The observed incidence increased with increasing risk score or estimated probability or incidence in the 2 data sets (both Ptrend < 0.001) (Table 5).
Table 5: Estimated probability and observed incidence of hypertension in the derivation and validation datasets. View Table 5
We developed and internally validated a simple prediction model for incident hypertension in two different cohorts of adults HIV patients in similar settings in line with the general recommendation that before being applied in clinical practice, prediction models should be internally or externally validated [15]. The c-statistic of the model in the original cohort (0.69 (95% CI 0.65 to 0.72)) was only slightly increased to (0.72 (95% CI: 0.65 to 0.77)) after external validation, consistent with findings from other studies from the Netherlands where the c-statistics of a prediction model for identifying nulliparous women who developed hypertension before 36 weeks of gestation using systolic BP, diastolic BP and weight increased from 0.75 (95% CI 0.68 to 0.81) to 0.78 (95% CI 0.75 to 0.82) after external validation [16]. The small increase in c-statistic in our study implies that the model predicts well based on initiation data routinely collected in HTCs and can be applied to the HIV patients in the study setting. The current risk prediction model for hypertension among HIV patients used BMI, baseline diastolic blood pressure and WHO clinical stage of HIV. These factors have been proven to be associated to incident hypertension in the general population and HIV patients.
Most prediction models for incident hypertension have focused on preeclampsia and eclampsia in pregnancy which is severer forms of the disorder [17]. However, incident hypertension in HIV patients is also associated with a reduced quality of life and poor health outcomes. Given that hypertension can be managed to prevent progression to severer forms and complications, a model that identifies women at risk is useful.
A limitation of our study was the application of clinical and physiological characteristics only, excluding biomarkers in our prediction model. This is because of the non-mandatory and non-routine use of these parameters during ART initiation in the Cameroonian setting. Both approaches are expensive and the equipment for analyzing these biomarkers is generally not available in many low-resource settings. However, future research could assess the added value of these biomarkers on incident hypertension among adult HIV patients.
There exist no risk prediction model for incident hypertension among HIV patients and the difficulty of predicting hypertension using only initiation parameters has been pointed out; however, the feasibility of applying these models in low-resource settings currently remains limited due to constraints in the availability of diagnostic equipment and the high cost of the tests which are beyond the means of most people who require them. Thus despite the increased predictive value of adding biomarkers to the predictive model; the need to derive reasonably accurate prediction models that use variables, which are routinely easy to obtain for low-resource settings is important.
In the development or derivation cohort, 119 participants were classified as being at high risk of developing hypertension. Fifty seven (32.4%) of them eventually developed hypertension giving a PPV of 32.4% and NPV of 92.4%. In the validation cohort, 121 participants were classified as being at high risk of incident hypertension and 63 of them developed the condition. Classifying HIV patients on ART into different risk categories allows for closer monitoring of clients at high risk. This will include more frequent refill visits or referral for specialist care.
Given that the addition of biomarkers in the screening of HIV patients could enhance the identification of those at high risk of incident hypertension, future research should explore the added value of biomarkers in the early identification of adult HIV patients at increased risk of hypertension in LMICs. Such studies should be accompanied by comparative cost-effectiveness of the routine data only predictive models and the models that combine routine data and biomarkers to provide essential health technology assessment information for future decision-making. In the interim however, despite the fact that the modest PPV in the development and validation cohorts show the limitation and difficulty of predicting hypertension using only anthropometric and clinical characteristics the model has the potential of identifying HIV patients at increased risk of incident hypertension for subsequent care and monitoring. Its further and external validation and use is worth serious consideration in low-resource settings.
We developed and validated a risk score prediction model for incident hypertension among adults HIV patients on ART. This model showed adequate performance (good sensitivity, specificity and diagnostic accuracy). This model could be useful in HTCs to identify patients with a high risk of developing hypertension. This will contribute to efforts in providing clinical decision-making that will improve on the clients' health and quality of life.
This model shows adequate performance and may be useful in Fako Division to promote the identification of adult HIV patients on ART at high risk of developing hypertension based on simple and non-invasive initiation parameters.
The study was based on secondary data whose quality and completeness is usually inadequate. Our limited sample was partly due to the fact that many file record were excluded for lack of complete follow-up data.
The strength of this study was that it made use of a retrospective cohort design which has a stronger potential of establishing causality than the cross-sectional design. The strength of the risk predictive model is its use of a few anthropometric and clinical variables already routinely obtained by healthcare providers during ART initiation. Such a simple predictive model to aid frontline providers estimate the probability of incident hypertension among adult HIV patients on ART and take relevant precautions is potentially lifesaving.
We would recommend that our risk prediction model be validated externally in other low-income settings as well as implementation research to inform implementation, monitoring and evaluation at scale in Cameroon.
This study was self-funded.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
TAY, ALN, NFP and EOG designed the study. TAY, NEN, NSA and KEN did the fieldwork. TAY and TN did the analysis. TAY wrote the first draft, and all authors approved the final version.
The authors declare that they have no competing interests.
This manuscript does not contain any individual's data. Consent for publication was obtained from the PhD thesis supervisors.
This study was approved by the Faculty of Health Sciences of the Institutional Review Board at University of Buea (No 5231/FHSIRB_UB/02/2020).