Background: The kinetics of viral shedding of asymptomatic COVID-19 in families is not well understood.
Objective: To study the characteristics of secondary cases in families, after the appearance of a primary asymptomatic case vs. symptomatic.
Methodology: An observational, longitudinal and retrospective study of families, in which there were at least two polymerase chain reaction (PCR) confirmed COVID-19 cases (one primary case or index and at least one secondary case), was conducted from March 15 to December 25, 2020, in a general medicine office in Toledo, Spain.
Results: 39 families with one primary case were included. Of these, 4 were asymptomatic (detected by having been contacts of known cases outside the family) with 8 secondary cases; and 35 were symptomatic, with 62 secondary cases. The asymptomatic primary cases were younger and there were more children than the symptomatic ones. Secondary cases of asymptomatic primary cases vs. secondary cases of symptomatic primary cases differed statistically significantly only because they were more frequently asymptomatic (75% vs. 31%), ethnic minority (75% vs. 27%), and having a smaller family size (12% vs. 60%).
Conclusions: In the context of general medicine in Toledo (Spain), before delta variant became dominant, and the subsequent appearance of omicron, asymptomatic primary cases more frequently give also rise to asymptomatic secondary cases, and preferentially occur in families with a small number of members, which are ethnic minorities. Since asymptomatic cases are infectious, and as they originate new secondary cases that are also asymptomatic, this can make their detection and isolation more difficult, probably contributing to the community spread of SARS-CoV-2.
COVID-19, SARS-CoV-2, Asymptomatic infections, Epidemiological characteristic, Prevalence, Household contact, Family characteristics, Retrospective studies
The coronavirus disease 2019 (COVID-19) due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1], is complex, presents variable clinical symptoms and different severity among patients, although most develop mild symptoms. Several features of SARS-CoV-2 (including high transmissibility, an incubation period with a long-tailed distribution, pre-symptomatic transmission, and the existence of asymptomatic infections, which may also contribute to transmission) make accurate detection during an ongoing epidemic challenging [2-9]. SARS-CoV-2 is transmitted through direct or indirect contact with infected people through infected respiratory droplets or saliva, fomites, or aerosols. Crowded indoor environments with tight and sustained contacts, such as homes, are high-risk environments. In addition, there may be reduced use of personal protective equipment in them compared to other environments [10].
Infected people can transmit the infection whether they are symptomatic or not [11], higher levels of virus can occur in presymptomatic and asymptomatic patients [12,13], and it is recognized that approximately one in three SARS-CoV-2 infections may be asymptomatic [14]. The available data on asymptomatic transmission of SARS-CoV-2 show that the ability of these individuals to transmit the infection is lower than that of the symptomatic and presymptomatic. But, in reality, it is difficult to study transmission from asymptomatic subjects, it is difficult to quantify it, there is little data available on the transmission rate of truly asymptomatic people, and transmission rate of truly asymptomatic people is unknown, as well as its role in the dynamics of COVID-19 [15-18].
Additionally, home transmission of COVID-19 is suspected to have contributed to the increase in cases [19,20]. Analysis of contact tracing data in Hong Kong between January and April 2020 revealed that the majority of transmission pairs infected by an identified contact involved household contacts [21]. Most people with COVID-19 receive care at home, which increases the likelihood of exposure for household members [22]. Thus, the cumulative risk to household contacts of an infected person is likely to be substantial during the peak of viral shedding [23,24], and it is believed that contact within households is responsible for approximately 70% of SARS transmission -CoV-2 when there are generalized community control measures [25].
Homes are ideal settings to assess the transmissibility of a pathogen and the associated determinants of susceptibility and infectivity [26]. However, less attention has been paid to family members and others who care for people with COVID-19 in the community; there has been little research that has evaluated the transmission of COVID-19 at the family level and the characteristics of the primary and secondary cases. In this context, we present a study whose objective was to study the characteristics of secondary cases in families, after the appearance of a primary asymptomatic case vs. symptomatic.
An observational, longitudinal and retrospective study of 39 families and 132 people, in which there was at least two polymerase chain reaction (PCR) confirmed COVID-19 cases -one primary case or index and at least one secondary case-, was conducted from March 15 to December 31, 2020, in a general medicine office in Toledo, Spain. The study was part of a set of studies on COVID-19 in families, and in part the methodology has already been published [27,28] and the present study uses secondary data from the previous one. Secondary cases without infection (with negative PCR and asymptomatic) were excluded in this study.
Symptomatic (primary and secondary) cases: The diagnosis was confirmed with PCR oropharyngeal. Information on COVID-19 patients and their contacts was obtained from the registry systems used by general medical services in the consultation. A confirmed case with active infection was considered to be any person with a clinical picture of sudden onset acute respiratory infection of any severity that occurs, among others, with fever, cough or feeling of shortness of breath; other symptoms such as odynophagia, anosmia, ageusia, muscle pain, diarrhea, chest pain or headache, among others, were also considered symptoms of suspected SARS-CoV-2 infection according to clinical criteria, and a positive PCR test. People with symptoms compatible with COVID-19 who had already had a PCR-confirmed SARS-CoV-2 infection in the previous 90 days were not considered suspect cases again [29].
Asymptomatic primary cases: They were detected by having been contacts of known cases outside the family. These cases had positive CRP and no symptoms throughout the follow-up period.
Asymptomatic secondary cases: They were defined as family members who, after the appearance of the index case, or from contact with a known case of COVID-19 outside the family, had positive PCR without the presence of any symptoms throughout the follow-up period.
Household contacts were defined as people who shared a residence with the COVID-19 index case. We defined family members as those who had lived with primary cases in a house 4 days before and for more than 24 hours after the primary cases developed COVID-19. Families with secondary transmission were defined as those where some or all of the family members become infected within one incubation period (2 weeks) of symptom onset of the primary case.
The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [30] or the date of positive CRP in asymptomatic patients.
It refers to the first case diagnosed or reported in the family. The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [30]. The onset date for an asymptomatic carrier was defined as the date a positive COVID-19 PCR test was obtained [30]. The incubation period of secondary cases was determined from the beginning of the symptoms or the performance of the PCR in asymptomatic patients, and other factors potentially responsible for their infection were ruled out, with respect to the beginning of the symptoms or the positivity of the PCR (in asymptomatic of primary cases). Contacts were quarantined shortly after the index case was diagnosed, thereby reducing the risk of transmission (but, this was a provision not available in all circumstances).
Data on the index case and close contacts were extracted from the medical records of the general medicine practice under study. The following variables were collected: age; sex; symptoms; chronic diseases (defined as "any alteration or deviation from normal that has one or more of the following characteristics: Is permanent, leaves residual impairment, is caused by a non-reversible pathological alteration, requires special training of the patient for rehabilitation, and/or can be expected to require a long period of control, observation or treatment [31]", classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD-10 Version: 2019 [32]; social-occupancy class (according to the Registrar General's classification of occupations and social status code) [33,34]; complex family and low income household based on the genogram and in the experience of the general practitioner for their continuity of care and knowledge of the family (genogram was a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that "complex" genograms present families with psychosocial problems) [35-38]; ethnic minority; family size (number of members); and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths/min., pulse oxygen saturation ≤ 93% with room air at rest, arterial partial pressure of oxygen/oxygen concentration ≤ 300 mmHg) [30]; to simplify comparison, moderate and severe cases were counted together.
A convenience sampling was used. The families participating in the study were chosen because they had their members in the same consultation and all medical information was available.
Secondary attack rate was defined as the number of new cases divided by the number of people exposed to a primary case. The existence of second or third generation cases was not assessed.
The bivariate comparisons were performed using the Chi Square test (X2) with Yates correction or Fisher Exact Test when necessary, (according to the number the expected cell totals) for percentages.
39 families with a primary case were included with a total of 132 cohabitants. There were 70 secondary cases with positive PCR, of which 25 were asymptomatic (25/70 = 36%), and 22 healthy cohabitants (with negative PCR and asymptomatic). Of the 39 primary cases, 4 were asymptomatic (detected because they were contacts of known cases outside the family), and in these families there were 8 secondary cases and 1 healthy partner (PCR negative and asymptomatic, which was not included in the study). The rest of the 39 primary cases, 35 were symptomatic, and in these families there were 62 secondary cases. Figure 1 shows the flowchart of the study.
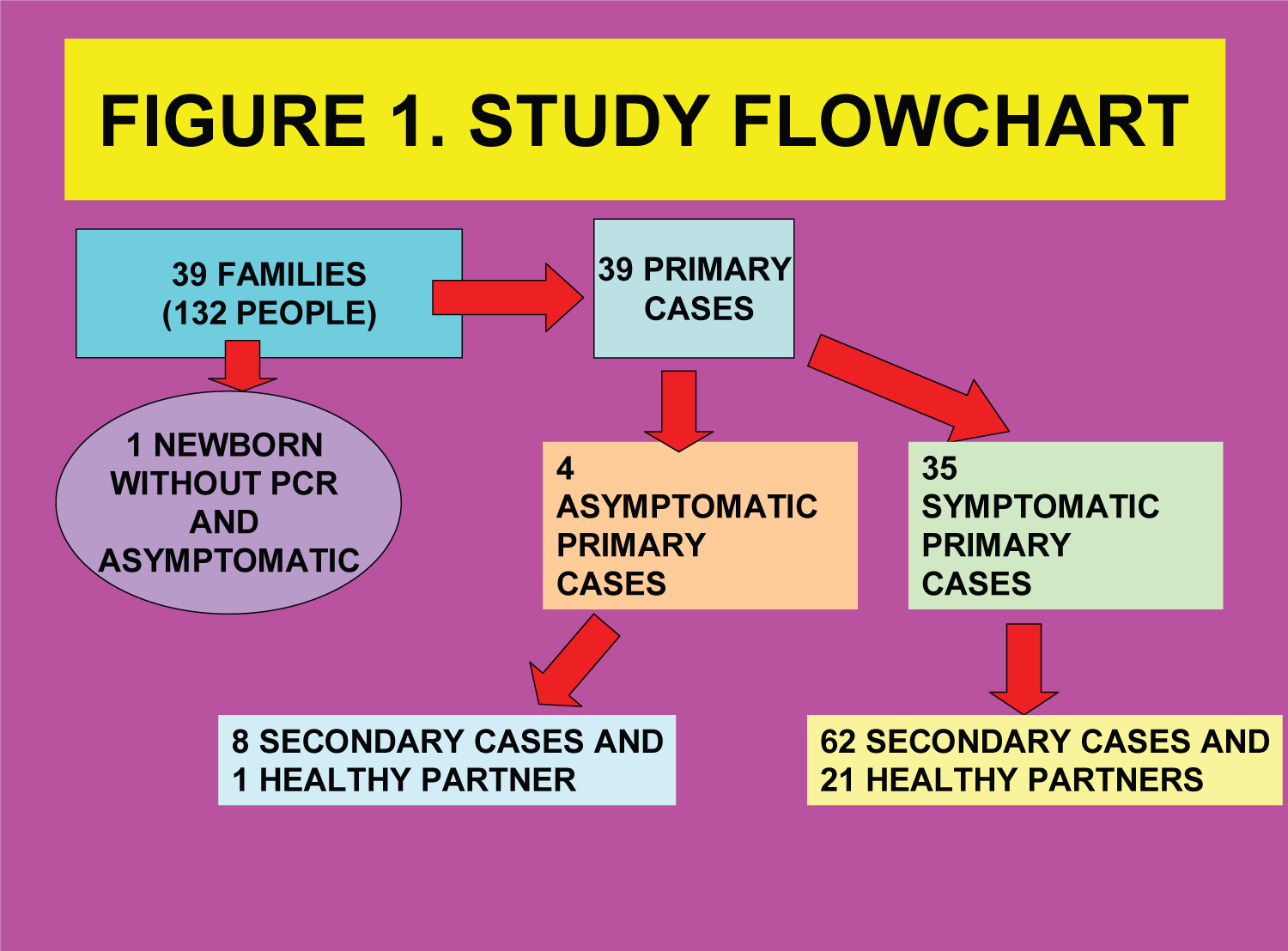 Figure 1: Study Flowchart: Transmission of asymptomatic primary cases in families. View Figure 1
Figure 1: Study Flowchart: Transmission of asymptomatic primary cases in families. View Figure 1
Asymptomatic primary cases were more frequently female vs. symptomatic primary cases: 1/4 (25%) vs. 17/35 (49%), but without statistical significance (Fisher exact test = 0.6094; NS.), younger (the mean age -Arithmetic mean + -Standard deviation- of the asymptomatic primary cases was 29.5 + -19.36 years, vs. 39.97 + -14.86 in symptomatic primary cases; t = -1.29847. P = 0.10108; NS.), and children (< 15 years) were more frequent (There was 1 child -25%- in asymptomatic primary cases vs. 2 children -3%- in the primary symptomatic cases, but the difference was not statistically significant, probably due to the small sample size; Fisher exact test = 0.1735; NS.).
Secondary cases of asymptomatic primary cases vs. secondary cases of symptomatic primary cases differed statistically significantly only because they were more frequently asymptomatic (75% vs. 31%; Fisher exact test = 0.021), being an ethnic minority (75% vs. 27%; Fisher exact test = 0.0128), and having a size of the minor family (12% vs. 60%; Fisher exact test = 0.0198) (Table 1 and Table 2).
There is increasing evidence that SARS-CoV-2 has substantial transmission heterogeneity, influenced by biological factors (characteristics possibly related to viral load), behavioral and social factors (certain people have a large number of contacts in relation to the population general), hazardous facilities (for example, confined spaces with poor ventilation) and what are called "opportunistic" situations (large events with many contacts, such as a wedding), or temporary increases in transmissibility (such as occurs when talking or singing out loud) [39-41].
Asymptomatic and presymptomatic carriers can transmit SARS-CoV-2 [8,42]. This presymptomatic transmission has been described in groups of patients with close contact approximately 1 to 3 days before the index patient developed symptoms [42]. Presymptomatic transmission is believed to be a major contributor to the spread of SARS-CoV-2. Model-based studies in China and Singapore estimated the percentage of infections transmitted from a presymptomatic individual to be 48% to 62% [43]. And mathematical modelling studies have suggested that asymptomatic individuals could be the main drivers of the growth of the COVID-19 pandemic [44]. However, little is known about the viral shedding kinetics of asymptomatic COVID-19. At the onset of infection, asymptomatic and symptomatic individuals have similar viral loads regardless of the severity of symptoms, but asymptomatic cases have lower titer at the replication peak, faster viral shedding, and therefore a period shorter infectious disease [15].
The available data on asymptomatic transmission, derived mainly from observational studies, vary in quality and appear to be prone to publication bias [44]. The role of asymptomatic carriers in transmission poses challenges for control of the COVID-19 pandemic. A mathematical framework has been described to assess the effects of asymptomatic transmission on the expected number of secondary cases generated by an average primary case in a completely susceptible population, and the fraction of new secondary cases attributable to cases alone. However, if asymptomatic cases tend to resolve quickly, asymptomatic individuals. If asymptomatic infections are more persistent than symptomatic ones, the mean generation interval for COVID-19 could be longer than estimated from symptomatic then current estimates of may be over-estimates of the underlying strength, and asymptomatic cases may be driving a larger fraction of secondary cases than we would expect without accounting for their differences. The importance of these effects depends on the relative infectiousness of asymptomatic transmission as well as the proportion of incident cases that are asymptomatic [45].
We found that secondary cases of asymptomatic primary cases vs. secondary cases of symptomatic primary cases differed statistically significantly because they were also more frequently asymptomatic (75% vs. 31%; Fisher exact test = 0.021); that is, asymptomatic primary cases generate more asymptomatic secondary cases than symptomatic primary cases.
Overall, a secondary attack rate (the proportion of people exposed to an index or primary case who develop the disease as a result of exposure) in households of 18% has been reported; however, there is significant heterogeneity between the studies with a rate ranging between 4% and 55%, and even higher in the same population of our study. In any case, the secondary attack rate appears to be higher for symptomatic index cases compared to asymptomatic cases (asymptomatic individuals would be much less likely to infect others than symptomatic cases), adults would have a greater susceptibility to infection compared with children, and the spouses of the index case would be more likely to present the disease) [10,26,28,46,47].
In this sense, a meta-analysis that tried to determine the extent of the asymptomatic infection and its transmission potential in the population suggested lower rates of transmission in asymptomatic cases. Transmission rates for asymptomatic cases ranged from 0% to 2% (and from 0.8% to 15% for symptomatic cases) [48,49]. But, in our study, the secondary attack rate (number of secondary cases in relation to the number of family members - exposed population) was higher in households with asymptomatic index case vs. symptomatic index cases (61% vs. 52%), but without statistical significance.
Lower infection rates have been reported in children, which can be attributed to asymptomatic or mild illness, because of a reduced susceptibility by cross-immunity from other coronaviruses. But, although children appear to have a reduced risk of symptomatic disease, it is not yet clear whether they shed the virus similarly to adults [10,50]; it has been reported that children and adolescents are less susceptible to infection, but more infectious a once infected; Although children and adolescents are much less likely to have a serious illness, they may be as likely as adults to develop symptoms [26]. We found that asymptomatic primary and secondary cases were younger than primary and secondary symptomatic cases (Table 1 and Table 2).
Table 1: Comparison between the secondary cases of asymptomatic primary cases and secondary cases of symptomatic primary cases. View Table 1
Table 2: Comparison of symptoms between secondary cases of asymptomatic primary cases and secondary cases of symptomatic primary cases. View Table 2
The absolute risk is influenced by the specific characteristics of the home and the duration of the exposure. In our study, as in most of them, primary cases and contacts were quarantined shortly after diagnosis of the index case, thus reducing the risk of transmission (but, this was a provision that was probably not available in all cases or circumstances and it could be not fully met). Secondary attack rates have been reported to be lower in households with fewer than 3 contacts [10].
In our study there were no statistically significant differences between the number of secondary cases in relation to family size between asymptomatic and symptomatic primary cases. Likewise, we found that secondary cases of asymptomatic index cases occur in households with smaller family size, vs. secondary cases of symptomatic primary index cases.
The spread of SARS-CoV-2 will only decrease if people who test positive for the virus isolate themselves. But waiting for them to do so is problematic. People are not perfect for adhering to the rules of isolation and social distancing, even in their own home. It is almost impossible to fully adhere to social distancing if patient live in crowded or inadequate housing. Furthermore, for millions of people around the world, a positive coronavirus test is not only a financial hit, but also a medical blow. Internal UK government surveys suggest that only 17% of people showing symptoms are undergoing tests, fearing that a positive result and consequent self-isolation will lose them money. Economically marginalized communities generally cannot simply immediately choose to modify their transmission networks through changes in their life or work contexts in the absence of specific support.
COVID-19 is known to have disproportionately affected the poorest in society, often in jobs that cannot be done from home or are unstable [51]. Similarly, people of minority ethnic origin in the UK and the US have been disproportionately affected by COVID-19 compared to white populations. An important factor in these ethnic inequalities may be differences in household structure between ethnic groups [52].
We did not find differences between social class (classified as specialized/non-specialized occupation), nor in the frequency of students, nor in the frequency of low-income households, nor the presence of family problems/complex families among the secondary cases of primary asymptomatic cases vs. secondary cases of symptomatic primary cases. However, there was significantly more ethnic minority in secondary cases of asymptomatic primary cases. Belonging to an ethnic minority (in our context mainly Latin Americans, Arabs and Gypsies) can be understood as an indicator of problematic economic or employment and housing potential. If we take into account that asymptomatic primary cases give rise to more secondary asymptomatic cases, and that the latter are people belonging to ethnic minorities (which indicates they are probably more reluctant to undergo a diagnostic test for fear of its employment and economic implications, and to comply with isolation due to their housing situations) we must conclude that asymptomatic infections pose a problem for the control of COVID-19.
The World Health Organization has reported an approximately uniform distribution of SARS-CoV-2 infections between women and men worldwide, with higher mortality in men [10]. Regarding contacts of primary cases, it has been reported that female contacts were slightly more susceptible than male contacts [26]. In the same sense, in our study there were no statistically significant differences by sex/gender between asymptomatic primary cases vs. symptomatic primary cases (25% vs. 49%), nor among secondary cases of asymptomatic primary cases vs. secondary cases of symptomatic primary cases (75% vs. 73%), where were predominantly women in both groups of secondary cases.
Regarding clinical symptoms, it has been reported that secondary cases were less severe than primary cases, with more asymptomatic cases and fewer severe or critical cases [26]. It is hypothesized that the lack of symptoms that could facilitate transmission (sneezing/coughing) may explain the low transmission rate of asymptomatic cases despite similar viral loads [12]. We did not find differences between the level of severity (they were slight 100% vs. 95%, respectively), nor in the presence of chronic diseases in the secondary cases of asymptomatic primary cases vs. secondary cases of symptomatic primary cases.
Our study has two important limitations that must be taken into account:
1. The sample of included families was not a probabilistic sample; It was a convenience sample (The families participating in the study were chosen because their members were treated in the same consultation and all the medical information was available). However, there are no logical reasons to think that the current research sample was different from the ideal, randomly selected sample (from the entire population), nor that there might be under- or over-represented people in the sample.
2. The small sample size. Some of the differences found in the comparisons, which were not statistically significant, could have been significant in a larger sample.
In the context of general medicine in Toledo (Spain), before delta variant became dominant, and the subsequent appearance of omicron, asymptomatic primary cases more frequently give rise to asymptomatic secondary cases, and preferentially occur in families with a small number of members, which are ethnic minorities. In summary, If we take into account that asymptomatic primary cases give rise to more secondary asymptomatic cases, and that the latter are people belonging to ethnic minorities (which indicates they are probably more reluctant to undergo a diagnostic test for fear of its employment and economic implications, and to comply with isolation due to their housing situations) we must conclude that asymptomatic infections pose a problem for the control of COVID-19. Since asymptomatic cases are infectious, the origin of new secondary cases that are also asymptomatic makes their detection and isolation difficult, probably contributing to the community spread of SARS-CoV-2.