Excessive salt/sodium (Sodium > 2 grams/day, equivalent to 5 g salt/day) and low potassium (less than 3.5 grams/day) intake increases the risk of heart attack and stroke. To fight against cardiovascular diseases, the nutritional strategy is to regulate the dietary intake of salt/sodium and potassium according to set standards.
Objective: This review aimed at documenting salt intake levels and the potential impact of salt reduction initiatives in Africa, based on studies published between January 2012 and April 2022.
Methods: These studies were obtained thanks to PubMed/MEDLINE electronic data, Google Scholar and specialized literature. The PRISMA guidelines were used to conduct the systematic review.
Results: The synthesis produced 583 articles of which 39 studies matched our inclusion criteria. Among these 39 studies, 24 (including 3 systematic reviews and one study) assessed the intake of salt/sodium and potassium from urine tests. Seven studies assessed the salt/sodium content in food and 7 other studies focused on the awareness, attitudes, beliefs and practices of populations with regard to salt intake. One study focused on modelling. Salt intake varied from one country to the other; all countries had an intake level beyond set standards (< 5g/d/p).
In Benin, for instance, the intake level was 4.4 g/24 h of sodium and 1.8 g/24 h of potassium. In Ghana, the estimated salt intake was 8.3 g/day and 6.8 g/day in South Africa. The salt content assessed in food also differed from one country to the other. In Nigeria, for instance, the sodium content was 1.36 g per 100 g of bread while it was 7.63 g (SD 3.12) per 100 g of bread in Tunisia. In Morocco, it was 8 to 9 g of salt for 100g of bread while it was 6 g in South Africa.
The awareness of salt/sodium intake and of food rich in potassium has increased over the last decade. In South Africa, for instance, it has been noticed an evolution of 38 % to 59.5 % (p < 0. 0001) with people having improved upon their awareness further to mass sensitization campaigns. Some studies carried out both in South Africa and Ghana helped notice positive changes further to abiding by the salt-reduction bill, voted in July 2016. Most countries that have either benefited from the WHO (SAGE) support or adopted one of the national strategies in salt reduction like the South Africa’s legislation, notably sensitization in Ghana and Nigeria, results proved to be encouraging.
Conclusion: This study reveals a significant decrease in salt intake in countries having adopted important strategies of salt reduction over this decade. However, these efforts must be maintained by the whole of of countries if we wish to meet worldwide 30% reduction objective in 2025.
Food intake, Sodium, Potassium, Salt, Africa
Non- Communicable Diseases (MNT) are generally chronic ones, with rather slow effects, they take much time to evolve and are generally not communicable from one person to the other [1]. These include essentially cardiovascular diseases, cancer, chronic lung affections and diabetes. They constitute the main mortality cause worldwide [2-4]. A high intake of salt /sodium (Sodium > 2 grams /day, equivalent to 5 g of salt/day) and a low intake of potassium (less than 3.5 grams/day) favour high blood pressure and increase the risk of heart attack and stroke [5-8]. According to the Global Burden of Disease (GBD) study carried out in 2017, a sodium-rich intake is pointed out as the main food risk causing death and years of disability (DALY) [9]. Worldwide, databases on sodium intake in the world show that the required standard is by far exceeded whereas potassium which is highly recommended is less consumed [5]. Indeed, a low intake of salt/sodium and a high intake of potassium results into a combined action in the THA decrease and the prevention of cardiovascular diseases [10-12]. In Africa, some studies on the salt intake among the population determined by the collection of urine in a day have proved that the average salt intake (ET) with African adults varied from 6.8 (2.2) g to 11,3 (5,4) g/day [13]. In Togo, despite the lack of data on sodium and potassium intake, the prevalence of high blood pressure (25-64 years: 19 % in 2014) [14] and the influence of cardiovascular diseases (MCV) on people’s health [15,16] show that an assessment and a survey of salt and food intake and potassium is necessary for the prevention of MCV/MNT.
Considering the evidence which shows the link between a high intake in salt and cardiovascular diseases and other ones, world leaders committed themselves in 2011 during the UN General Assembly to prevent and control Non-Communicable Diseases (MNT), to reduce people’s exposure to inadequate food intake and to reduce salt-intake of the population as a necessary step to alleviate the world burden due to MNT. In 2013, AMS adopted nine world voluntary objectives for preventing and controlling Non-Communicable Diseases (MNT) which include a relative reduction of 30% of salt intake by the 2025 horizon through world action plan for preventing and controlling Non-Communicable Diseases 2013-2020 [17]. Some studies were carried out on salt intake of the population namely those by the WHO on the world ageing population and the adult (WHO-SAGE).Such mass studies were carried out in six countries (China, Ghana, India, Mexico, Russia and South Africa) in three respective waves: wave 0 (2004), 1 (2007-2010) 2 (2014-2015) 3 (2018-2019) and a few reviews systematically were carried out in Sub-Saharan Africa [13,18,19]. With the recent systematic reviews carried out in Africa, we believe that other studies might have brought along new changes about the new salt intake rates. Hence, we deduce that: “Sodium intakes remain high and potassium intakes low in many African countries. Implementing optimal intake strategies for these nutrients is effective”. To verify this hypothesis, we set as objective to document systematically all the studies concerning salt/ sodium and potassium intake in Africa and aimed at implementing the WHO recommendations about salt intake reduction. This will enable us to adjust strategies in fighting against cardiovascular diseases and to reduce mortality caused by non- communicable diseases [20,21].
We do state that there are no conflicts of interests throughout the procedure of this general excerpt. To this end, the current study was carried out as a systematic review to identify, list, describe and summarize the main studies carried out about salt/sodium and potassium intake to assess the implementation level of recommendations in the fight against MCV/MNT. Our objective was to summarize the existing database on the salt intake levels in Africa. This step will enable us to identify the various strategies to fight against excessive salt/sodium and low potassium intake.
The PRISMA guidelines [22] were used in writing completely the systematic review. A documentary research was carried out in March and April 2022 thanks to PubMed/Medline database, Embase and Google Scholar and was updated in May 2022. It was completed by a specialized literature research using the same terminologies in Google, WHO’s sites and by experts in nutrition and Non-Comunicable Diseases (MNT). These research strategies used for biometric database are considered as supplementary materials. A manual research of references was done based on the excerpts of articles from these very databases.
A study is complete if the following criteria are met: Complete publications available on line, both in English and French between January 2012 and April 2022, concerning the salt intake of the population, the salt levels in food, the awareness, the attitudes, the practices and the people’s behavior. Modelling studies were also included. Duplicate publications, conference minutes and review articles were excluded.
Two examiners carried out the research, excerpted potential articles and deleted duplicate publications. Next, they independently examined the titles and summaries for eligibility. Entire passages were retrieved from all articles deemed to be potentially eligible, and these ones had been independently examined with disagreements which were solved by discussions.
To avoid methodological errors and analysis about collected data which could cause systematic consequences on the quality of this current literature review, distorted facts were highlighted to assess the quality level of the selected studies in compiling this systematic review. This is specifically about the confusion between a bad analysis or a controversial factor which has no link of cause with the study.
Data collection took place by simultaneous documents reading by scholars. The collected data concern on one hand the authors, the years of studies, the publication date, the country of the study, the design of the study, the characteristics of the population and the summary of the results. The data collection was carried out by the leading author and revised by the second author.
A narrative synthesis of the results (descriptive approach) was undertaken due to the hybrid nature of the collected results in the studies.
The Figure 1 shows the chart of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) of our research, which offers 1951 quotatio ones, after removing duplications. Among these ones, 1329 were removed from the database based on filtering of titles, summaries and age targets. The selection of a complete text of 583 articles of the remaining synthesis identified 39 studies that matched our inclusion criteria. Among the 39 studies, 25 (of which 3 systematic reviews and one study) assessed salt /sodium and potassium based on urine tests. Seven studies assessed the salt/sodium content in food and 7 other studies focused on the awareness, the attitudes, the beliefs and the practices of the populations with regard to salt intake. One study focused on modelling. Seven studies assessed the salt/sodium content in food and 7 other studies focused on the awareness, the attitudes, the beliefs and the practices of populations with regard to salt intake. One study focused on modelling (Table 1).
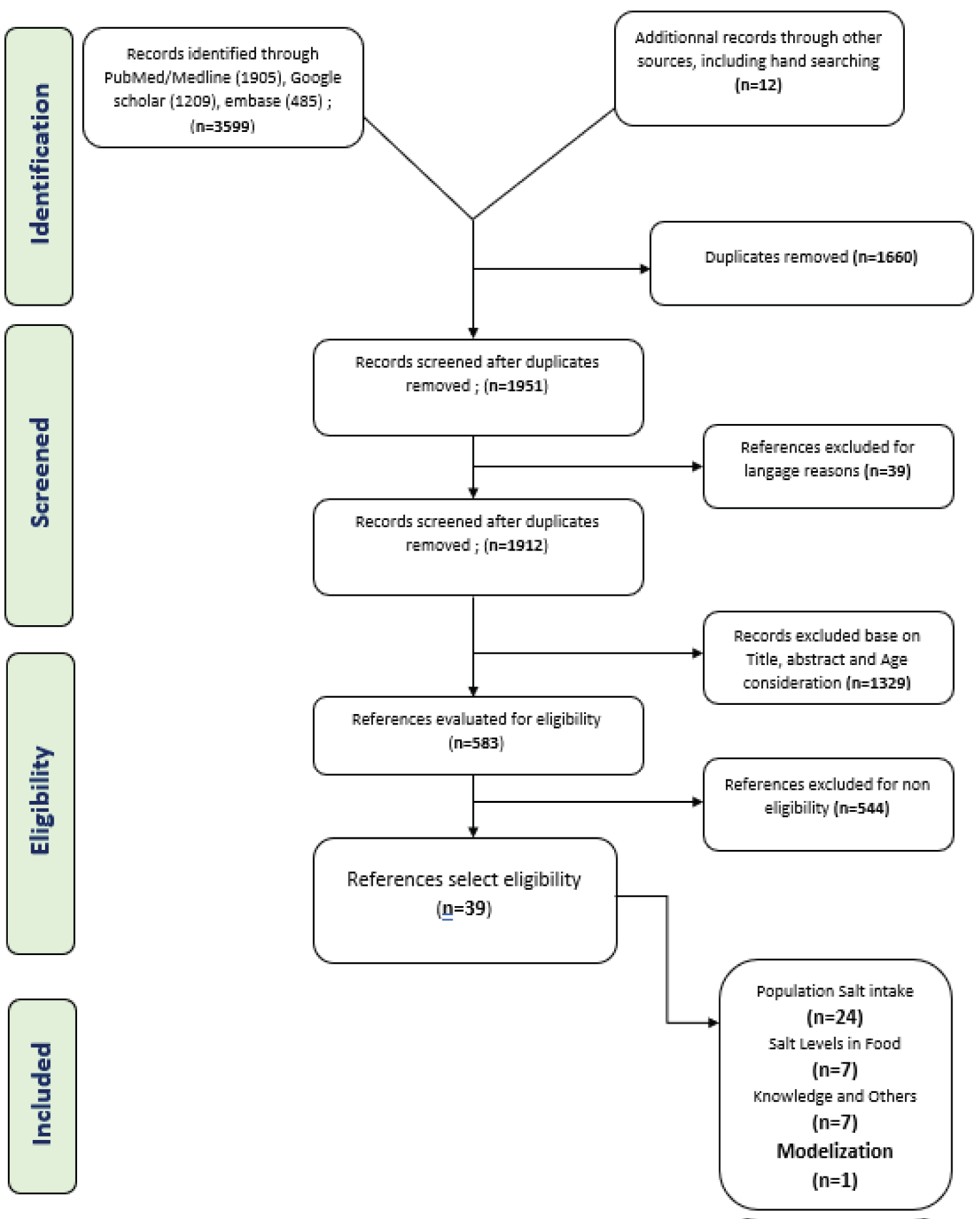 Figure 1: Monitoring and implementation of salt reduction initiatives in Africa: A systematic review.
View Figure 1
Figure 1: Monitoring and implementation of salt reduction initiatives in Africa: A systematic review.
View Figure 1
Table 1: Classification of studies conducted in the 15 Africa contries.View Table 1
Fifteen African countries in all reported on 39 studies on salt and MCV/MTN. The studies included a range of study designs, including 25 cross-sectional studies, 11 case-control studies, 2 mass studies, and 01 modelling study (Table 2).
Table2 : Summary and characteristics of the studies included in the systematic review.View Table 2
Twenty-four studies carried out in 12 countries reported on salt intake. Of these studies, 24 estimated both potassium and sodium intake; only 29 only estimated sodium intake in order to assess the level of salt intake in relation to blood pressure. Although salt intake varies depending on countries, all had an intake beyond set standards (< 5g/d/p). Therefore, in Benin, for instance, 4.4 g/24 h of sodium and 1.8 g/24 h of potassium was reported [39]. In Ghana, the estimate of salt intake was 8.3 g/day and 6.8 g/day in South Africa [24,40].
Seven studies in 5 countries estimated salt level in food. The most consumed foods were selected for tests, namely the used bread. Salt levels differed according to countries. Therefore, in Nigeria the salt content was 1.36 g/ 100 g of bread while it was 7.63 g (ET 3.12)/ 100 g of bread in Tunisia. In Morocco, it was 8 to 9 g of salt/ 100g of bread while it was 6 g in South Africa.
Similarly, seven studies carried out in 5 countries assessed the behavior of populations in relation to salt. They aimed at improving the populations awareness for a considerable reduction in the intake of food highly in sodium (Na) versus food rich in potassium. Some of these studies were able to assess consumers’awreness after mass sensitization campaigns. In South Africa, for instance, we observed an increase from 38% to 59.5% (p < 0.0001) of people having improved upon their awareness level after a mass sensitization campaign [34]. In Kenya, the STEPS survey showed that 89.5% reports on food intake was highly rich in sodium and foods intake was low in potassium [46].
Three studies conducted in two countries, Ghana and South Africa, were able to assess the effects of salt intake reduction interventions in order to considerably reduce morbidity and mortality due to MCV/MNT. In Ghana, for instance, after a community awareness campaign on salt reduction, urinary sodium excretion increased from 50 mmol/d/person (p < 0.001) to 47.46 mmol (p < 0.001) [44]. In South Africa, in the mass study (Waves 2 and 3) a significant difference of 1.16 g/day/person (p = 0.028) was observed further to the implementation of the legislation voted in June 2016 [28].
This review aimed at identifying studies carried out in Africa in relation to salt/sodium and potassium linked to cardiovascular diseases and/or non- communicable diseases. Considering these results, four types of studies were identified, namely salt assessment studies with total and/or occasional urine test methods or 24-hour recall methods; studies assessing the sodium/potassium levels in the most-consumed food by the population; public perception of the links between sodium/potassium intake and cardiovascular diseases (particularly high blood pressure) and the studies carried out aimed at reducing excessive sodium intake and increasing potassium intake.
Broadly speaking and regardless of the type of study (cross-sectional, case or mass study), it was observed that salt/sodium intake was excessive and low in potassium between 2012 and 2022 despite the commitment of the countries since 2013 [13,19,59,60]. In compliance with the WHO’s guidelines, it is important to quantify current salt intake levels of the population. This is particularly important in sub-Saharan Africa where the epidemiological transition is likely to lead to dietary changes and a high increase in the MNT prevalence.
Furthermore, resources for treating salt-associated diseases may not meet the expectations of the population in such a way that preventive strategies, like salt reductions are important to avoid associated morbidity and mortality [61-63]. To identify populations among which sodium intake is high and to assess progress regarding the WHO’s sodium reduction target, it is necessary to know the sodium intake in Africa. Therefore, thirty-two studies carried out in our document conducted in 12 countries namely South Africa, Benin, Cameroon, Cape Verde, Ethiopia, Ghana, Malawi, Morocco, Mozambique, Nigeria, Uganda and Tunisia reported on the salt intake. Among these studies, 24 assessed both potassium and sodium intake; sodium intake solely from urine tests in twenty-nine. Although salt intake varied from one country to the other, all had an intake beyond set standards (< 5 g/d/p).
In our systematic review, at the beginning of the decade, Benin had an estimate of 4.4 g/24 h of sodium and 1.8 g/24 h of potassium [39]. In Ghana, the salt intake was 8.3 g/day. In South Africa, in a 2013 study, it was 9.5 g/d, 8.5 and 7.8 g/d in white, mixed and black populations respectively [24,40]. All these observations similar to previous studies carried out on the salt intake levels within populations [64,65] showed to which extent it was important to set in place-integrated strategies to reduce salt/sodium intake.
Studies on dietary salt/sodium and potassium levels are hard to carry out since they require both resources and appropriate technologies. Beside, the dietary issue remains a challenge in a context whereby the choice of food is individual and varies according to the consumers' tastes [65]. Seven studies were able to assess the sodium level in the staple food. The average salt and sodium level in bread in Tunisia (Maghreb) was 7.63 (ET 3.12) and 3.0 (ET 1.23) g/kg while in Nigeria (West Africa) it was 5.0 ° 0.20 mg/100 g bread. These variations could be explained by the differences in food choices and habits of individuals.
Seven studies assessed the awareness, habits and behavior of populations with regard to the salt/sodium intake. Even if the populations are more sensitized about the harmful effects of excessive salt, the rigor in the choice of food low in sodium and high in potassium remains insufficient. Three studies were able to show an improvement of awareness about salt intake. They have demonstrated the need for awareness campaigns as additional strategies in the fight against excessive salt/sodium intake.
The evaluation of the effects of the legislation in South Africa was done in two studies. Another evaluation study focused on the implementation of awareness campaigns in Ghana [28,30,44]. These studies yielded fruits because positive changes were observed thereafter. However, it should be pointed out that efforts are yet to be made if the objective of reducing salt intake in the world by 30% by the year 2025 is still maintained. Still, we were able to notice that the WHO supported only a few African countries notably South Africa and Ghana to carry out large mass studies for the assessment of salt intake level and monitoring over time, particularly the SAGE (Study on Global AGEing and Adult Health). This may explain the low availability of data on the continent because the other countries handicapped by the costs related to these studies were less committed. It is important to encourage all African countries to make data available through operational research studies for a better action.
Therefore, in the light of the results of our research study, only high impact sensitization campaigns such as the adoption and implementation of legislation in South Africa and major mass campaigns yielded minor successes because despite the obtained changes, the results are beyond the set standards intake recommended by the WHO. It is difficult for us to assess salt reduction efforts in other countries since there were no sensitization campaigns or post-sensitization campaigns evaluation. Nevertheless, efforts are to be encouraged as more and more countries are taking measures to reduce salt intake. However, additional measures are essential to reduce the health consequences associated with excessive salt intake, particularly in low- and middle-income countries where the risk of death from high blood pressure is higher, more than double that in high-income countries [66]. Likewise, the WHO encourages the use of tools such as SHAKE to technically assist countries in their fight [67,68]. These tools integrate multidimensional actions extended to other health partners targeting consumers, industry and government in addition to an efficient leadership and political commitment [69].
The strengths of this systematic review lie in the almost exhaustive search of studies carried out throughout the African continent. They were identified both in Sub-Saharan Africa and in the Maghreb countries. This study was able to appreciate the trends observed at the beginning and at the end of the decade (2012-2022) with regard to the levels of salt/sodium and potassium intake and this through the different methods which were the assessment of urinary sodium/potassium through spots and/or total urine, dietary sodium/potassium level and the awareness, attitudes, beliefs and practices of food consumers. Some also appreciated the perception of taste based on the variability of salt in food. Two reviewers reviewed the study extraction methodology. This confers more certainty to the various studies carried out. Unfortunately, this review was unable to obtain enough intervention studies to conduct the meta-analysis. No single strategy can be dependent on the reduction results observed in these studies. It will therefore be important to be cautious in the different conclusions made in these studies.
This review highlights the value of updating and monitoring studies on the assessment of salt/sodium and potassium intake levels in each country in order to assess the level of achievement of the global goals by 2025. Reducing salt intake is underway but remains a challenge for all countries in the African region due to the nutritional shift that the continent is initiating. In addition, the disease burden associated with high salt intake is also increasing in Africa and might strain public health systems that are not strong enough. The sensitization campaigns supported by the WHO, although limited in scope, are to be encouraged in other countries in order to optimize salt reduction efforts and to encourage the intake of foods rich in potassium, protective factors against cardiovascular diseases/non-communicable diseases.
Nothing to report.
No conflict of interest to declare.