Background: This community-based study was conducted to determine the proportion of individuals in the population that had been infected by the SARS-CoV-2 virus and developed antibodies before the end of the second wave of the pandemic and introduction of COVID-19 vaccines in Nigeria.
Methods: Between December 2020 and March 2021, 2,244 markets sellers and shoppers aged ≤ 70 years across six states [two northern (Kano and Kaduna), two eastern (Ebonyi and Imo), and two western (Oyo and Lagos) regions] were enrolled in the study. Demographic information was collected from the participants as well as whole blood which was separated into plasma and tested for SARS-CoV-2 total antibodies with a validated ELISA kit (WANTAI SARS-CoV-2 Ab ELISA) approved by the U.S. Food and Drug Administration.
Results: Overall, 1, 453 participants tested positive for the antibodies giving a seroprevalence of 66.8%. The antibodies were significantly (P = 0.0001) detected across the six states with the highest rate in Kano (83%) and the lowest rate in Lagos (39%). Participants who were ≤ 19 years and those between 60 and 69 years had the highest (68.42% (104/152) and lowest (56.20%: 68/121) seroprevalence rates respectively. In terms of religion, higher antibody levels were significantly (χ2 =17.4664, P = 0.0001) detected among Christians (75%: 576/766) compared to Muslims (65%: 395/609). There were no significant relationships between antibody positivity rates and gender, education, economic as well as marital status (p > 0.05).
Conclusion: Six out of every ten participants in this study had antibodies against SARS-CoV-2 before the second wave and introduction of COVID-19 vaccines. Increased activities and mobility may be responsible for high levels of SARS-CoV-2 antibodies among young persons while differences in religious practices may account for the low prevalence of SARS-CoV-2 antibodies among Muslims compared to Christians.
The ravaging effect of Coronavirus Disease-2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) cannot be over-emphasized as the ongoing pandemic was declared a public health emergency of international concern in March 2020 (WHO, 2020a). The virus emerged in late December 2019 in Wuhan city, Hubei Province, China [1], since then, over 281 million cases and 5.4 million deaths have been reported to WHO and 8.6 billion vaccine doses have been administered worldwide as of 29th December 2021 (WHO COVID 19 dashboard). About 3.4% of this global statistic was reported in the African continent with around 220,000 deaths recorded (COVID-19 Worldometer).
In Nigeria, 242,877 cases with 3,033 deaths were reported as of 2nd January 2022 (NCDC COVID 19 dashboard). The burden of SARS-CoV-2 cases varies among different states of the country: Lagos (39%), Abuja (11%), Rivers (6%), Kaduna (5%), Kano (2%), Oyo (4%), Ebonyi (1%) and Imo (1%). These cases were diagnosed using molecular-based methods. Several reasons have been suggested for the low prevalence of SARS CoV-2 infection in Africa, one of which is the low testing capacity due to the fragile health system and exiguous molecular laboratories [2-5]. Although studies have shown that over 80% of persons infected with the virus were asymptomatic [6-10], most of the tests conducted in African countries were among people with symptomatic infections [4,7,11-14].
Molecular detection of SARS-CoV-2 using PCR on oropharyngeal swabs and nasopharyngeal swabs has several drawbacks including the need to use of specialized expensive equipment, the need for a high level of technical expertise, and a few false-negative results leading to long turnaround time which translates into low testing capacities [6,11,15-18]. Severe acute respiratory syndrome coronavirus 2 is enveloped, positive sensed RNA viruses belonging to the beta (β) group of coronavirus subgroups (Wang, et al. 2013; Muhammad, et al. 2020) with four structural proteins (spike, envelope, membrane, and nucleocapsid) as well as accessory proteins [19-21]. Several molecular RT-PCR methods have been designed to detect the structural protein genes (E gene, S gene, N gene) [15,22,23]; however, there is still very little information as to the host antibody immune responses to these important proteins. This information is important for containment, mitigation, and promotion of vaccination efforts [21,24].
The extent of SARS-CoV-2 infection in many African countries including Nigeria remains unclear, underscoring the need for antibody serosurveys to assess the cumulative infection rate of the virus among the populace [23,25]. Serological tests to identify the presence of IgG and IgM antibodies may offer a more valid estimate of the frequency of SARS-CoV-2 past and recent infection in the community since the antibody produced in response to infection is likely to remain in circulation for a longer period after the viral infection has been resolved [6,11,16,26,27]. Serological tests detect SARS-CoV-2 antibodies, indicating prior infection in individuals. By supplementing diagnostic testing for acute infection and informing the public health response to COVID-19, population-based serological testing provides better estimates of the cumulative incidence of infection [27]. Furthermore, as the world advances into vaccination, it is becoming increasingly vital to synthesize seroepidemiology results to follow the transmission of the virus, identify disproportionately afflicted populations, and assess progress toward herd immunity [28-30].
Therefore, this study was designed to determine the prevalence of SARS-CoV-2 total antibodies (IgM and IgG) in three geographical zones of Nigeria before vaccination roll out in the country.
This community-based cross-sectional study was conducted in two northern (Kano and Kaduna), two eastern (Ebonyi and Imo), and two western (Oyo and Lagos) states in Nigeria. These sites were representatives of specific geopolitical zones in the country and the prevalence of SARS-CoV-2 in these places varies significantly. Blood samples were collected from male and female sellers and shoppers in some major open markets in the six states.
Individuals 15 years and above who were in the market for one reason or the other and consented to participate in the study were included, while pregnant women and those under 15 years were excluded.
This study was conducted between December 2020 to March 2021 the availability and introduction of COVID-19 vaccines in the country. This period also coincided with the second wave of the COVID-19 pandemic. Participants were recruited after obtaining their informed consent to participate in the study. Demographic information such as age, gender, occupation, and contact details, as well as other behavioral factors, were collected using an electronic-based questionnaire platform (epicollect). A total of 2,244 blood samples were collected by trained phlebotomists. Five milliliters of whole blood were collected from each participant into EDTA-containing tubes, stored properly in a sealed container using a triple packaging system, and transported to the contact laboratory within the state of collection. Plasma was separated from the samples (after centrifugation at 3500 rpm for 5minutes) and stored immediately at -20 °C until transported under cold chain condition using a triple packaging system to the Department of Virology, University of Ibadan, Oyo State where all samples were stored at -80 °C until analyzed.
Plasma samples were analyzed for total antibody (IgM and IgG) against SARS-CoV-2 using commercially available ELISA kits (WANTAI SARS-CoV-2, Beijing, China). The ELISA kit is approved for use by the U.S. Food and Drug Administration and it is used for identifying persons with adaptive immune responses to COVID-19 infection. The assay was performed on all the 2,244 samples collected under strict biosafety conditions and according to the manufacturer's recommendation. There were no cross-contamination or invalid results during analysis. The assay was previously evaluated in the Department of Virology for specificity by testing samples collected one year before (January – October 2018) the outbreak of SARS-CoV-2 in late 2019.
Ethical approval for this research was obtained from the respective state ministries of health where this research was conducted. All results were delinked from patient identifiers and anonymized.
Statistical analyses were performed using Microsoft Excel and STATA. Categorical variables were compared using Z and chi-square tests while quantitative variables were compared using ANOVA. The test of significance was set at P< 0.05. The number and percentage of positive results were used to summarize data for each assay. The significance level was indicated at a 95% confidence interval (CI) and was reported for each metric.
A total of 2, 244 plasma samples were tested in this study utilizing the serological testing method, with the distribution appropriately depicted below. The overall positivity rate of SARS-CoV-2 antibodies among the study population was 66.8% (Figure 1). As shown in Figure 2, the levels of antibodies detection were significantly (χ2 = 255.2275, df = 5, P = 0.0001) different among the states with the highest in Kano (83%) and lowest in Lagos (39%). The age group of the participants ranged from ≤ 19 to ≥ 70 years with participants ≤ 19 years having the highest seroprevalence (68.42%) while those within the age group 60 to 69 years old had the least proportion (56.20%) as shown in Table 1. Participants who were Christians had significantly (P = 0.0001) higher antibody levels (75%) compared to Muslims (65%) as depicted in Table 2.
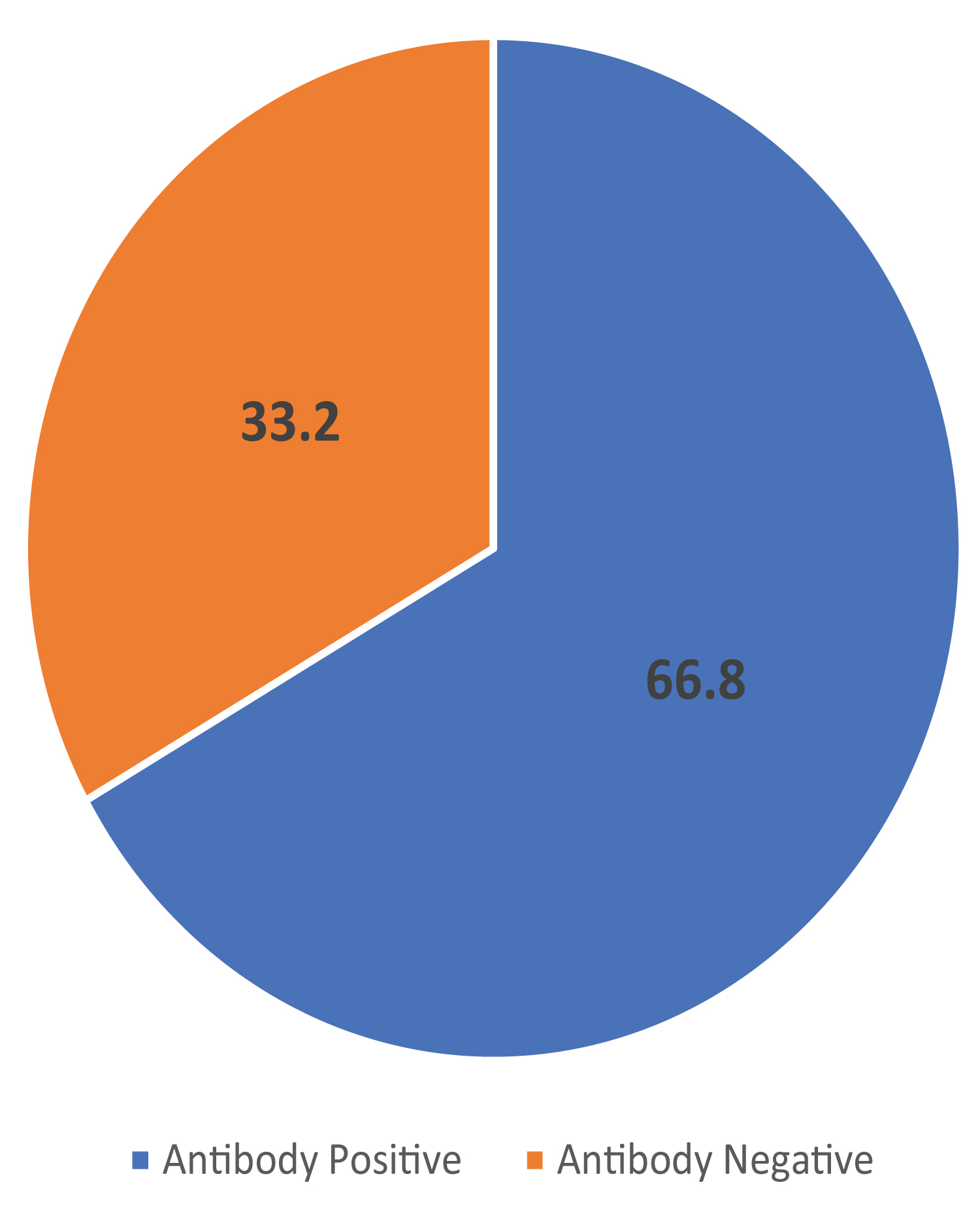 Figure 1: Overall prevalence of SARS-CoV-2 antibodies among study participants. Values are shown in percentages only. The total number of participants is 2244.
View Figure 1
Figure 1: Overall prevalence of SARS-CoV-2 antibodies among study participants. Values are shown in percentages only. The total number of participants is 2244.
View Figure 1
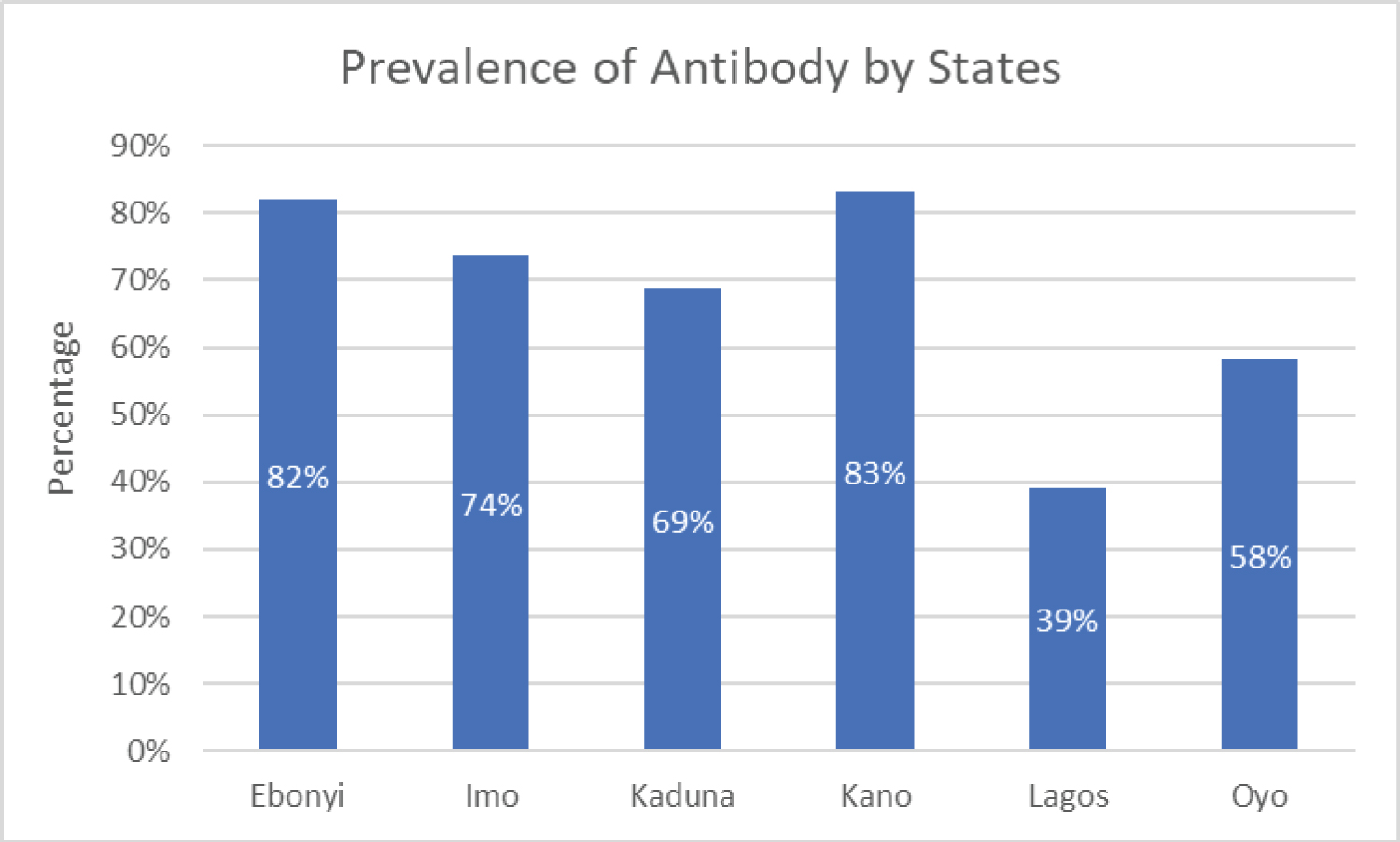 Figure 2: Bar graph showing the rate of SARS-CoV-2 antibody among participants from six states in Nigeria (χ2 = 255.2275, df = 5, P = 0.0001). Kano had the highest seropositivity (83%) while Lagos had the lowest (39%).
View Figure 2
Figure 2: Bar graph showing the rate of SARS-CoV-2 antibody among participants from six states in Nigeria (χ2 = 255.2275, df = 5, P = 0.0001). Kano had the highest seropositivity (83%) while Lagos had the lowest (39%).
View Figure 2
Table 1: Age and gender distribution of seroprevalence of SARS-CoV-2 antibody among study participants View Table 1
Table 2: Seroprevalence of SARS-CoV-2 antibody among participants based on demographic factors View Table 2
Level of education, economic status, gender, and marital status occurred with almost the same frequency and had no significant relationships with antibody positivity rates. Based on ethnicity, individuals who were Igbos had the highest positivity rate of 78% while the Yorubas had the least (58%) as shown in Table 2. Differences in antibody levels within ethnic groups were significant (P = 0.0001). When comparing shoppers and sellers, the antibody positivity rate shows that shoppers had a rate of 72%, whereas sellers had 69% which was not significant (χ2 = 1.6883, df = 5, P = 0.194) Figure 3.
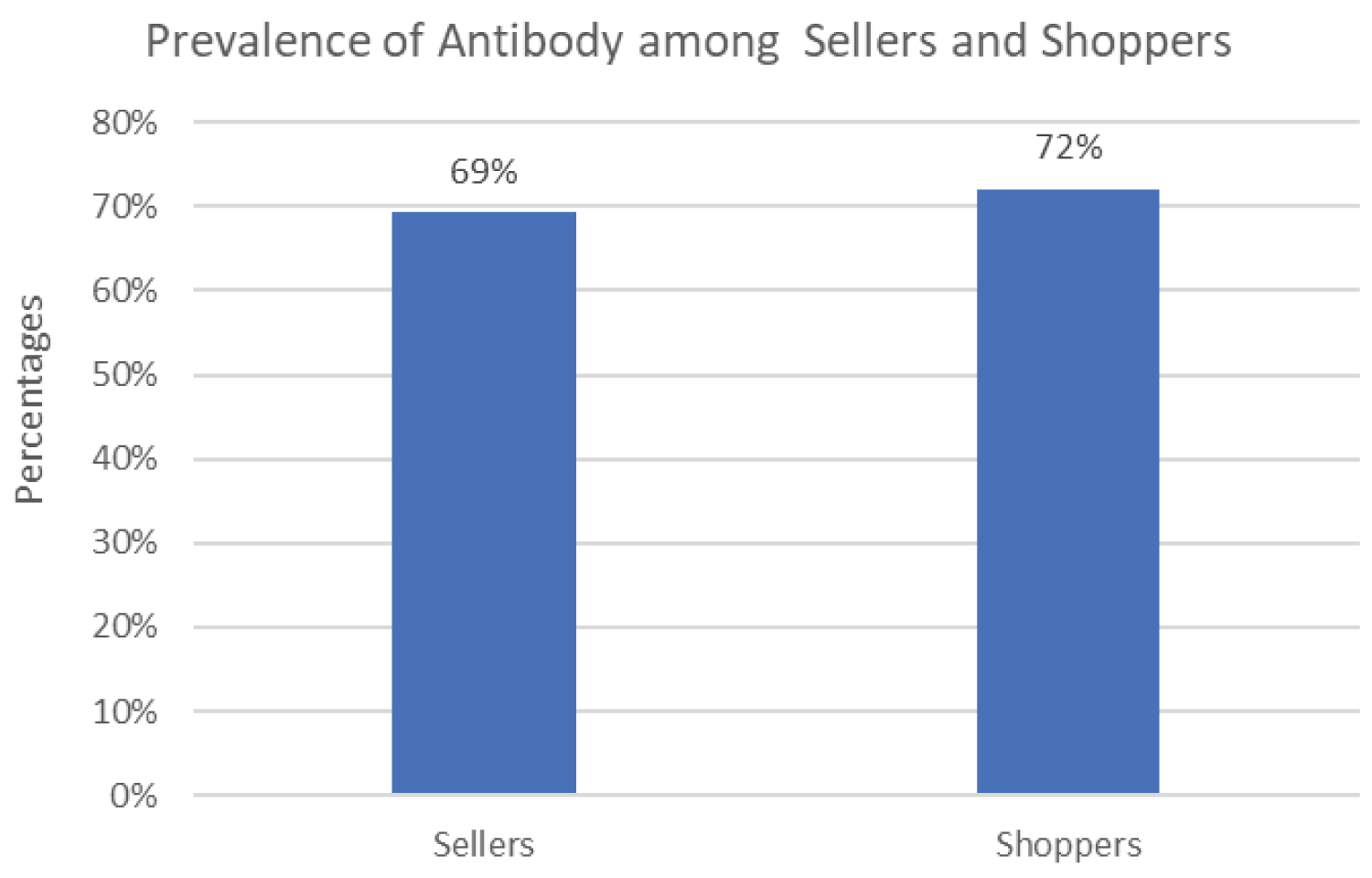 Figure 3: Graph showing the positivity rate of SARS-CoV-2 antibody between shoppers and sellers in the market (χ2 = 1.6883, df = 5, P = 0.194). Shoppers had a higher rate (72%) compared to sellers (69%).
View Figure 3
Figure 3: Graph showing the positivity rate of SARS-CoV-2 antibody between shoppers and sellers in the market (χ2 = 1.6883, df = 5, P = 0.194). Shoppers had a higher rate (72%) compared to sellers (69%).
View Figure 3
To aid the design of broadly protective vaccines, it is necessary to understand the antibody responses to SARS-CoV-2 infection before and after vaccine introduction, also before, during, and after successive waves of the epidemic [27,29,31,32]. While several studies have focused on antibody responses during vaccination rollout, there is very limited data on the baseline prevalence of antibodies to SARS-CoV-2 in African countries including Nigeria [32,33], particularly at the community level, where people may be infected but asymptomatic. This information is critical in filling the gaps in knowledge relating to the duration of antibodies to natural and artificial infection. A proper understanding of the seroprevalence of the infection will also guide the surveillance of the emergence of diverse variants and immune escape strains [18,28].
In this study, the overall rate of SARS-CoV-2 antibody among participants was 67%, indicating that many people have been exposed to the virus, most of whom were asymptomatic or probably symptomatic but did not report for test, thus putting other people at risk of contracting the virus. This rate is quite high compared to the rate of approximately 20% found in the Ciheb household survey conducted between September and October 2020. The collection of samples for this study coincided with the second wave of the COVID-19 pandemic in Nigeria. This may explain the difference in the prevalence obtained in the Ciheb study, in addition, antibody detection in this study was done using ELISA which is known to be more sensitive than the rapid test device used in the Ciheb study. Furthermore, the use of a rapid test kit can also explain the low seroprevalence of SARS-CoV-2 antibodies reported in Anambra (17.6%) [34], a south-eastern state of Nigeria compared to the prevalence of 78% found for south-eastern states in this study. Previous studies have highlighted the low-performance characteristics of rapid test kits for screening purposes [35,36].
The high rate of SARS-CoV-2 antibodies may have indicated fairly good herd immunity, however, it is not clear whether these antibodies were neutralizing. The prevalence of SARS-CoV-2 antibody decreased with age with participants of less or equal to 19 years having 68% antibody prevalence compared with participants within 60-69 years with the prevalence of over 56%. Immune senescence [37], thymus regression [38], and reduced B-cell number and activity with increasing age age may have contributed to this difference in antibody prevalence [16] in addition to the probability of more exposure to infection. While the elderly stayed at home during the lockdowns, the younger people were more active and mobile. Frequent events and concerts held by Christians in churches with a lot of singing, dancing, sharing of Holy Communion, and other activities might play a big influence in their high antibodies positive rate when compared to Muslims. The practice of ablution by Muslims as well as the frequency of prayers may explain the lower prevalence of SARS-CoV-2 antibodies among Muslim participants.
Increased activities and mobility might explain the high prevalence of SARS CoV-2 antibodies among students and unemployed participants compared to employed or married participants. Most students in the country are taught in crowded spaces and classrooms and they are also known not to comply with prevention protocols. These factors may also have contributed to the high prevalence among students. We found no gender differences in the prevalence of anti-SARS-CoV-2 among participants in this study. This finding needs further investigation because previous studies found that men had higher SARS-CoV-2 infectivity rates compared to women [39-42], and male participants with underlying conditions, including diabetes, hypertension, and cardiovascular diseases developed a severe form of the infection, with increased mortality rate [43,44]. Many factors such as hormone-specific reaction and activity of X-linked genes, which modulate the innate and adaptive immune response to virus infection were suggested [41,42,45-48]. As possible reasons for these observations.
We found in this study that at least 67% of the participants had circulating anti-SARS-CoV-2 antibodies which vary with the region of the country, age, occupation, and religion of the participants. This has implications for vaccine efficacy and attainment of herd immunity [29,31,49,50]. Diagnosis of COVID-19 based on the molecular detection of the viral RNA using RT-PCR sometimes produces false-negative results due to low viral load in the nasal and pharyngeal swabs [7]. Therefore, a huge number of symptomatic subjects might not be detected, contributing to further spread of the virus in the population. Detection of COVID-19 specific antibody among asymptomatic individuals will give an indication of true burden sub-clinical infection and the possibility of herd immunity. Evidence of antibody responses to SARS-CoV-2 infection was reported [33,50,51] and people who recovered from the infection have antibodies to the virus [27]. However, the presence of SARS-CoV-2 antibodies in the asymptomatic but exposed population is critical for understanding the extent of risk factors associated with SARS-COV-2 infection. The present study provided data on the percentage of people with detectable anti-SARS-CoV-2 which are relevant to the population at risk, plasma therapy, and herd immunity [18,28,29].
In patients with SARS-CoV-2 infection, B cell concomitantly with T follicular helper cell responses starts from 1 week after symptom onset against the nucleocapsid (N) protein. Within 4-8 days after symptom onset, antibody responses to S protein were reported. Neutralizing antibody responses to S protein begins by week 2, and most patients develop neutralizing antibodies by week 3 [52-56]. However, a subset of patients may not develop long-lasting antibodies to SARS-COV- 2 [11] but it remains unknown whether these patients are susceptible to re-infection [12]. Antibodies to SARS-CoV-2 were detected in 82%, 83%, and 39% of participants from the South-eastern, Northern, and South-western parts of Nigeria respectively. This might be related to higher exposure to SARS CoV-2 probably because of none- or late compliance to COVID-19 prevention strategies by participants from Northern and Eastern regions of Nigeria.
The presence of SARS-CoV-2 antibodies has immunological implications. The IgM type of CoV antibody was reported to promote early inflammation through activation of the Complement pathway [11], leading to severe form of COVID-19 through antibody-mediated immune enhancement (ADE), initiating upregulation of pro-inflammatory cytokines, and downregulating anti-inflammatory cytokines [57-61]. However, neutralizing IgG antibodies provides protective immunity by binding the receptor-binding domain (RBD) of the viral spike protein to prevent the virus from attaching to the ACE 2 receptor for SARS-COV-2. It was however reported that the concentration of each antibody class is crucial in its function as either protective or pathogenic which is important to vaccine design and immunization delivery [62-64]. Moreover, having both anti-Cov-2 IgG and -IgM antibodies might be an indication of active antibody production to an ongoing SARS-COV-2 infection. However, the absence of detectable anti-Cov IgG/IgM antibodies might be due to lack or low levels of these antibodies but does not necessarily mean the absence of active infection. Thus, there will be a need to determine the class-typing of SARS-CoV-2 antibodies.
In conclusion, the results of this study provided baseline information on SARS-CoV-2 seroprevalence in areas of low and high transmission of the virus in Nigeria. The high seroprevalence of SARS-CoV-2 total antibody by the second wave of COVID-19 and preceding commencement of vaccination in Nigeria may be due to the earlier exposure to COVID-19 and might enhance the achievement of herd immunity in the country. However, it is not clear if these circulating antibodies are neutralizing.