Adults with congenital heart disease are a growing population in Colombia and worldwide. Currently, Colombia has a population of more than 51 million inhabitants, with 38.2 million adults, 115,000 of whom live with congenital heart disease of varying complexity. The demographic profile shows that this population with congenital heart disease is mostly young, with ages ranging from 20 to 44 years. Keeping them in optimal health is a challenge, and care involves centralization in special adult congenital heart disease units. This manuscript is a narrative review of the current situation of adults with congenital heart disease living in Colombia. Colombia's current population pyramid is analyzed, and the demographic profile of the adult population with congenital heart disease is described. Finally, the strategies used for developing an adult congenital heart disease unit in Colombia are described, based on the comprehensive model of specialized care for a growing population.
Adult congenital heart disease, Colombia adulthood population, Adult congenital heart disease unit, Specialized care
Congenital heart diseases (CHDs) are the most common congenital anomaly in the world. They are five times more common, overall, than other congenital malformations, and 60% more prevalent than cancer, affecting approximately 0.8% to 1.2% of live births (LBs) worldwide [1]. The prevalence varies around the world and is directly related to the birth rate as well as the quality of records in each country and region, being more prevalent in Asia due to the birth rate and less prevalent in Africa due to underreporting. The meta-analysis by Lui Y, et al. [2] analyzed 260 studies published between 1970-2017, including a total of 130,758,851 LBs, of which 1,161,030 had CHD. They concluded that the mean global prevalence of CHD was 8,224 (7,817-8,641) per thousand. Due to pediatric cardiology's progress in diagnosis and surgical treatment, today many CHD survivors have reached adulthood. This demographic change has been seen most markedly in high-income countries in America, Europe, Asia, and Oceania, where there are more adults than children with CHDs today, showing a prevalence of 6 adults with CHD (ACHDs) for every 1,000 [3]. In middle and low-income countries (MICs and LICs, respectively) in Latin America (LATAM), although the number of children with CHDs continues to be prevalent, the number of ACHDs who currently live there is not negligible and continues to increase 5-6% per year [4].
With this information, it is not surprising that the MICs and LICs in LATAM are concerned about the emerging new ACHD population, which differs from the traditional adult cardiovascular patient. The cardiovascular diseases prevalent in adults, like systemic hypertension, ischemic heart disease, heart failure (HF), and atrial fibrillation, among others, are now being combined with various forms of adult CHDs, with more complex expressions and complications. Concentrating ACHDs in specialized healthcare units is a hugely important point for interdisciplinary care, especially in complex cases, thus improving this population's survival [5,6].
In LATAM, there is an estimated prevalence of 8-13 children with CHDs for every 1,000 LBs, and each year, more than 57,000 children are born with CHDs. Of these, 45% are moderate and high-complexity defects and, due to the severity of the CHDs, up to 25% require urgent surgical or hemodynamic interventions within their first year of life to survive. Without intervention, 14% die within their first month of life, and up to 30% before turning one. Today, it is estimated that only 8% of children with CHDs receive timely and specialized care within the first year of life [7]. Of the rest, close to 50% will develop serious sequelae such as pulmonary arterial hypertension (PAH), HF, Eisenmenger syndrome, and serious arrhythmias, among others. These, coupled with childhood comorbidities (respiratory infections, gastrointestinal infections, malnutrition, parasitosis, tropical diseases), increase childhood mortality from this cause [8]. Prior analyses of CHD mortality in Mexico showed that CHDs accounted for 55% of total deaths from congenital anomalies among children under one-year-old in 2013 [9].
Child mortality is directly related to poverty and the healthcare system's resources, and financial resources are directly related to the economic development of a country or region. According to the most recent 2021 World Bank data [10], the LATAM economies (except Chile) are mostly emerging economies, with most countries classified as MICs and others as LICs. Therefore, it is not surprising that childhood mortality from CHD continues to be high in these regions. Epidemiologically, the six most common lesions (atrial septal defect, pulmonary valve stenosis, aortic valve stenosis, coarctation of the aorta, ventricular septal defect and patent ductus arteriosus) comprise 67% of CHDs at birth. While not all of these lesions are amenable to interventional correction, many subsets are, and may contribute to as many as 30% of all detected CHDs [11]. These CHDs are considered to have a good prognosis when they are diagnosed and treated in time. In LATAM MICs and LICs, with diagnoses still delayed and surgical repair remote for many children, these CHDs end up taking the lives of many children before age one, increasing childhood losses from simple defects. However, even with late repairs, almost 90% of survivors reach adulthood, and many of them have significant CHD sequelae and residuals. As in other parts of the world, this entire population with a history of CHDs now becomes "the new ACHDs" [12], and LATAM is not the exception, since more and more ACHDs are arriving at hospitals like a tide. This whole new population should be managed in specialized ACHD centers [13].
Colombia has problems in the healthcare and coverage of children with CHDs similar to those in other countries in the region. Late diagnosis and delayed repair of many CHDs in infancy is not only expressed in greater child morbidity and mortality, but also in that those who survive childhood procedures and reach adulthood do so with greater morbidity. In other words, the ACHDs present with greater aggressiveness and a less favourable clinical expression.
The clinical phenotype of various CHDs which should have been repaired and not have sequelae is more severe in these adults. Many patients reach adulthood with severe hemodynamic consequences as a result of late repairs (PAH, HF, severe arrhythmias, stroke, valvular regurgitation, and sudden death, among others). As occurs in other LATAM countries, it is not surprising that unrepaired CHDs of varying complexity are frequently diagnosed in adulthood [14]. To further understand the picture, current regional observations and research show that more than 60% of patients who leave pediatric cardiology services are lost to follow up [15]. These significant losses of patients with CHDs of varying complexity will be tomorrow's adults who will return to adult cardiology services in a few years with severe hemodynamic decompensations.
Although we do not have official records of the exact number of ACHDs in Colombia, specifically, the institutions which are more advanced in CHD cardiovascular care and are developing ACHD services are showing clear growth in this population. In my cardiovascular institution with an ACHD unit we have seen a substantial increase in the adult population seen each day. Thirty to forty percent of the ACHDs being followed at our center are from pediatric cardiology services and the remaining 60% consist of adults with CHDs who were scattered among unspecialized adult cardiology services or were not being followed.
To be more accurate and aligned with the actual number of ACHDs in a given region, you must:
a) Know the current number of inhabitants,
b) Know how many of these are currently adults, with 18 years being the age limit for pediatrics, and
c) Know the survival of the pediatric CHD population.
A detailed observation and analysis of Colombia's population pyramid, specifically for the adult population, shows that the current population is mostly young, that is between the ages of 20 and 44, with the second largest adult population group being those 45-64 years-old and, finally those over 65-years-old. This population analysis is extremely important in relationship to healthcare needs. As has been mentioned, if the number of ACHDs is increasing, the largest group in the population pyramid (20-44 years-old) will logically be the one to require the most care and resources (Figure 1).
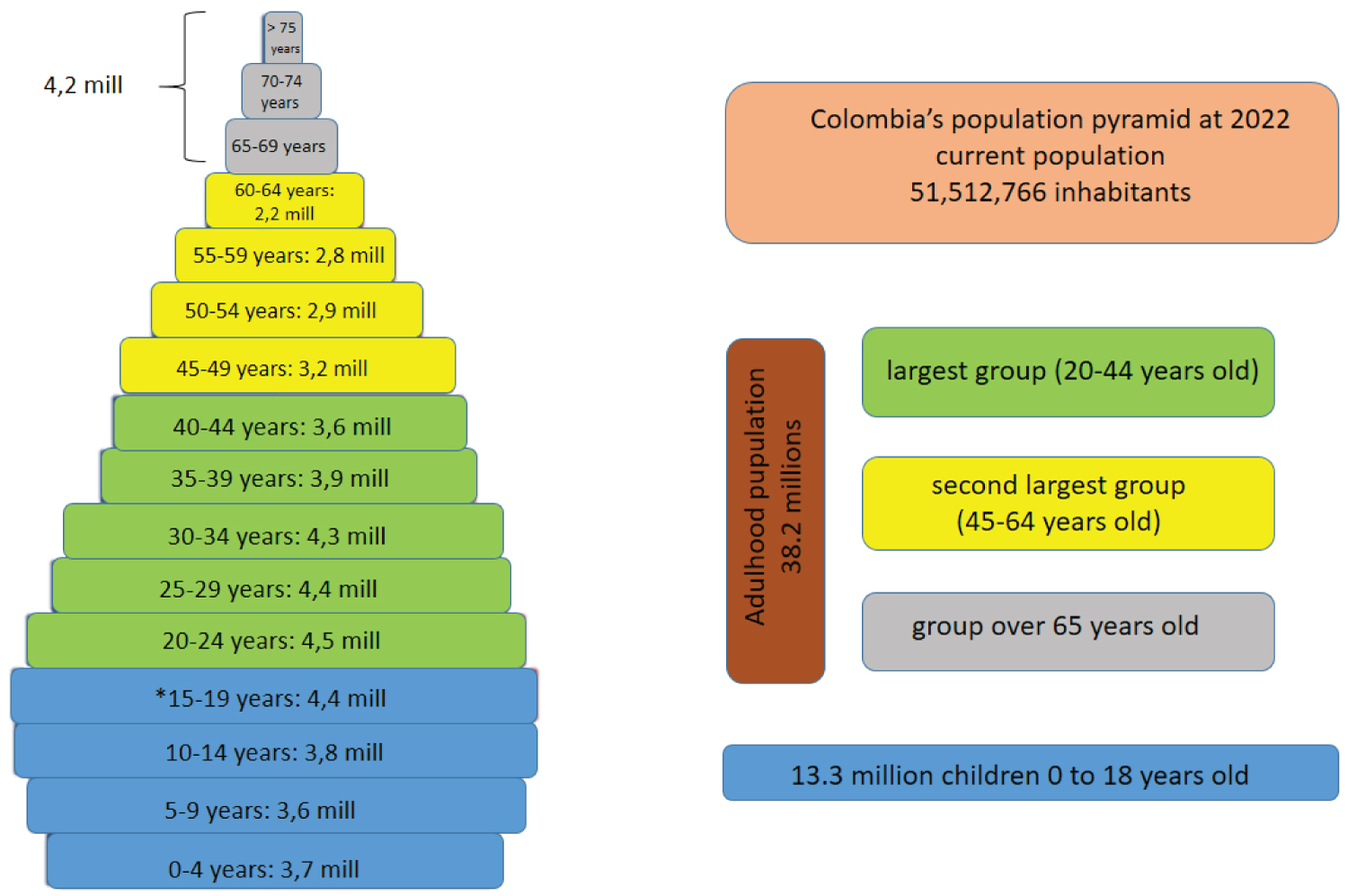 Figure 1: Colombia's adulthood population analisys pyramid at 2022.
Figure 1: Colombia's adulthood population analisys pyramid at 2022.
Green color represents the largest adult population group between the ages of 20 and 44 years, followed by the second largest adult population group being those 45-64 years-old in yellow color, and finally in gray color those over 65-years-old. [modified from Pirámides de población del mundo desde 1950 a 2100. Population Pyramid.net [17]].
The numbers of inhabitants by age groups are expressed in 2 digits for better understanding.
*This age group has a population of pediatric and adult age (over 18 years of age), it is assumed that at least half of this population is already over 18 years of age.
View Figure 1
Colombia has a developing economy, whose productive driving force consists of working-age people (over the age of 18) up to retirement age which, according to current Colombian retirement law is 57 years for women and 62 years for men [16]. This point is key for a country with a growing economy, since this population represents the society's productive column, and it is therefore essential for this group to be in optimal health.
Health care expenses, as well as many other social benefits are financed by tax contributions paid by people who are currently working. If this population is not healthy, the productive machinery will be affected, directly impacting tax contributions to the healthcare system, which will not be able to meet the Colombian population's expenses, much less cover the expenses of the ACHD population. This direct observation is alarming, as an increasing number of CHD survivors, especially those with complex forms of CHD, are reaching adulthood, and many of these continue to have physical limitations which limit their productive capacity (for example, univentricular heart survivors, unrepaired CHDs with HF or PAH sequelae, and Eisenmenger syndrome, among others). This point should be well understood by the cardiologists responsible for this population's healthcare. Professionals practicing in outlying hospitals must know how to promptly refer patients to specialized ACHD care. Those of us who are specialized ACHD cardiologists are aware of this need and should concentrate our efforts on rehabilitating this currently ill population, delivering them to society in an adequate condition to continue being part of the economically productive column.
Colombia's current population is 51,512,766 inhabitants [17]. Analyzing the population distribution by ages, we can conclude that there are slightly more than 13.3 million children 0 to 18-years-old. This figure represents 26% of the Colombian population, and with the estimated prevalence of CHD (8-13 cases per 1,000 LBs), there would currently be 106,000 to 172,000 children living with CHDs, constituting 37-60% of the burden of prevalence of CHD in Colombia.
In turn, the remaining 38.2 million inhabitants consist of adults, representing 74% of the Colombian population. Extrapolating this data, we could infer that there may be more than 115,000 ACHDs currently living in Colombia. This is assumed based on the number of ACHDs/million adults, and would account for 40% of the country's CHD burden (Figure 2).
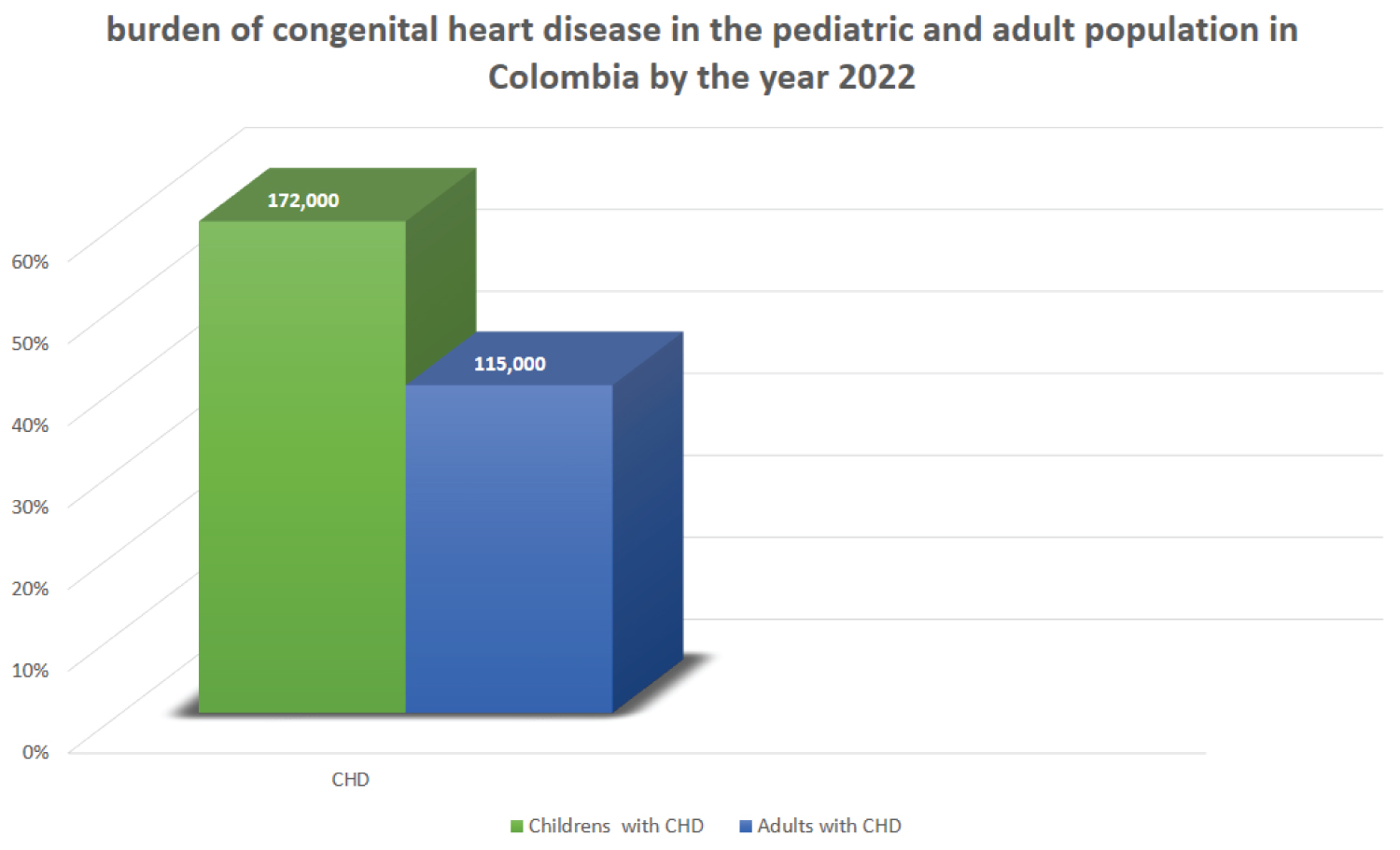 Figure 2: Burden of congenital heart disease in the pediatric and adult population in Colombia by the year 2022.
Figure 2: Burden of congenital heart disease in the pediatric and adult population in Colombia by the year 2022.
The green color represents the estimated number of pediatric population with CHD living in Colombia by the year 2022, this represents 60% of the CHD burden. The number of adults is represented in blue color and corresponds to 40%.
View Figure 2
Considering the socioeconomic profile of the Colombian population, the largest population group consists of adults from 20-64 years-old, which make up the economically productive driving force, and includes more than 33.2 million people. The rest, over the age of 65, are a minority with just over 5 million, and this population has mostly retired, or does not engage in economically significant work. In fact, they incur healthcare expenses as they are not active and tend to have chronic geriatric illnesses, many of which are disabling.
Our decentralized healthcare system does not allow statistical data from the main hospitals and cardiovascular centers to be unified. This is also complicated by the population's heterogeneity and dispersal throughout the country [18].
Keeping a registry of the number of ACHDs being followed at a given central or outlying hospital will be a requirement for the professionals caring for this population. Sharing this data among institutions will help provide a more accurate knowledge of the number of ACHDs, establish the projected growth of this population and develop healthcare policies aimed at improving care for this population.
The complexity of CHDs demands a high degree of understanding of their pathophysiology and natural progression throughout the lifespan. Knowing how to deal with each particular case and make appropriate decisions is a challenge in each stage of life. In past decades, little was known about the natural progression of CHDs in adulthood, and complex defects were practically nonexistent. Fifty years ago, only 10% of these survived [19]. Throughout the following decades, thanks to the success of timely diagnosis and early surgical repair, the demographic profile of CHD survivors began to change. While ACHDs with simple defects continue to predominate worldwide, the number of ACHDs with complex defects is not insignificant and grows evert year. Europe, with more than 50 years' experience in managing ACHDs, has achieved a life expectancy of 60 years in 40% of ACHDs with complex defects [20].
Globally, in past decades, the vast majority of ACHDs had simple defects, and there was a certain degree of unconcern for this population. Complex CHDs were specific to the pediatric population, so efforts were aimed at developing pediatric cardiology units, especially in developing countries. On the other hand, in developed countries, the prevalence of ACHDs grew rapidly and the situation reversed. Now there are more adults than children with CHDs, and an ever-increasing number of adults with complex defects. Due to the need to provide specialized care for this new population, the adult congenital heart disease specialty was created. In America, this specialty was officially recognized in the United States by the American Board of Medical Specialties in 2012, after a joint petition by the American Board of Pediatrics and the American Board of Internal Medicine [21].
In Colombia, the number of ACHDs has increased rapidly, especially over the last decade, due to greater survival of children with CHDs, who have already reached adulthood. This does not mean that there were no ACHDs before. In fact, they have always existed, but with a different demographic profile, since the ACHDs seen previously by cardiology were adults with unrepaired CHDs (mostly simple defects) who survived to adulthood naturally. So ACHDs care was handled by adult cardiologists. As was previously explained, moderate and high-complexity CHDs were only an issue in the pediatric population, so adult cardiology had no interest in learning about this specific field.
Just as occurred in developed countries, the demographic profile of adults with CHD has changed at an accelerated pace. Thus, the complex forms of CHDs began to increase in adults, and this attracted the attention of some pediatric and adult cardiologists who showed an interest in following this population in Colombia.
Following the international guidelines for ACHD care [22,23], the ACHD specialty has begun to be officially implemented in Colombia over the last few years. The first step was to create the Colombian ACHD chapter in 2017 [24], which sought to integrate specialists who were active in the management and care of ACHDs to work together on academic activities, research, education and professional growth cooperation. Since the creation of the chapter, various academic activities have been conducted nationally and internationally, including congresses, symposia, conferences, and webinars with live streaming in various LATAM countries. This chapter has a website on the Sociedad Colombiana de Cardiología [Colombian Society of Cardiology] web page [25].
Raising the awareness of the country's adult and pediatric cardiologists is helping the ACHD population which is dispersed over several regions to be referred to the cardiovascular centers that currently have ACHD specialists and are able to provide specialized care.
Specialized health care is understood to be a group of care, diagnostic, therapeutic and rehabilitative activities, as well as health promotion, health education and disease prevention activities which, due to their complexity should be conducted at this level of care. And specialized ACHD care is understood to be the set of activities focused or centered on adults with CHD.
In Europe and North America, as child CHD survivors reached adulthood and their number increased exponentially, physicians began to describe a new population of ACHDs requiring super-specialized care, especially those with complex defects who had undergone surgery as children or had never had surgery. These suggestions were made decades ago in Europe by Dr. Jane Somerville (British cardiologist, Imperial College, London) [26].
Expert, consensus and ACHD guideline recommendations [27] recommend that this population be centralized or concentrated in special units, known as "adult congenital heart disease units" (ACHD units), which have the highest care capacity, or Level III complexity in ACHD care.
Following the recommendations for the organization/functioning of ACHD units, one began a few years ago, which is projected to be the most advanced and a model in Colombia. The project is being carried out at a cardiovascular center in north western Colombia, only 45 minutes away from the city of Medellín (the second largest and most important city in Colombia), and only 20 minutes from the international airport. It is connected by a network of high-speed roads to more than 23 municipalities, allowing inhabitants from nearby areas as well as the city of Medellín to access specialized ACHD care.
It is a private cardiovascular center which came into being in response to the need for specialized cardiology care, and specifically ACHD care. The Cardiovascular and Special Studies Institute [Instituto Cardiovascular y de Estudios Especiales (Incare)] and Rionegro Medical Society (Somer Clinic) [Sociedad Médica de Rionegro (Clinica Somer)] decided to join forces to create an institution with the logistical and technological capacity to respond to the healthcare needs, with a focus on the comprehensive model of specialized care. This is how Somer Incare emerged in 2004.
The pediatric CHD program had already been functioning unofficially since 2014, and interest in ACHD care began to develop in 2016, with the pediatric and adult CHD program officially inaugurated in 2018. Today, it is a constantly growing and developing program (Figure 3). With more than 200 cardiovascular surgeries per year, it is one of the most solid CHD care institutions in the country.
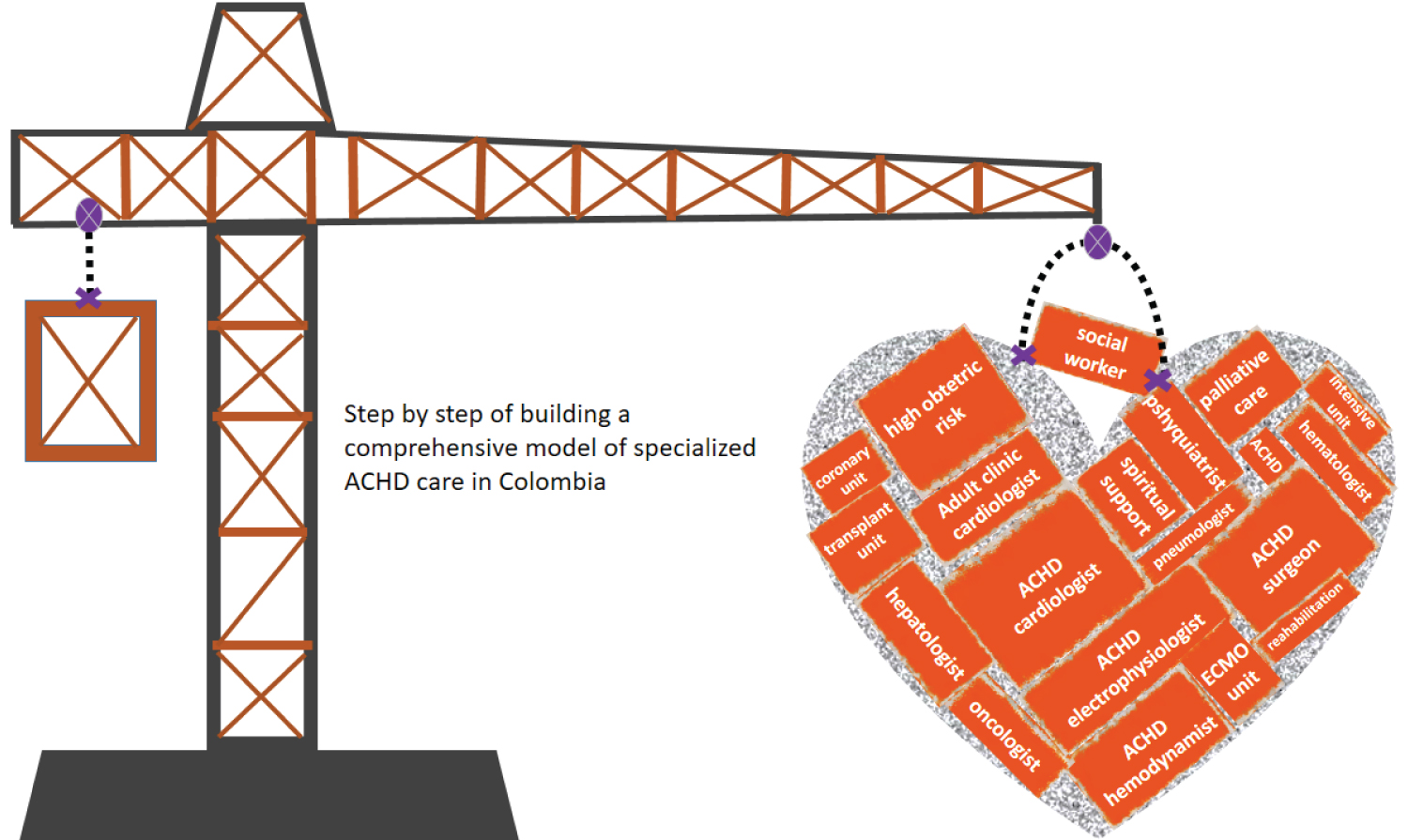 Figure 3: Building a comprehensive program specialized in ACHD in Colombia.
Figure 3: Building a comprehensive program specialized in ACHD in Colombia.
Multiple complementary cardiac and non-cardiac specialties that need ACHDs. Proposal for a comprehensive care model in Colombia.
View Figure 3
The objective of the comprehensive program for specialized CHD care involves the joint implementation of four main programs closely related to CHDs (Figure 4).
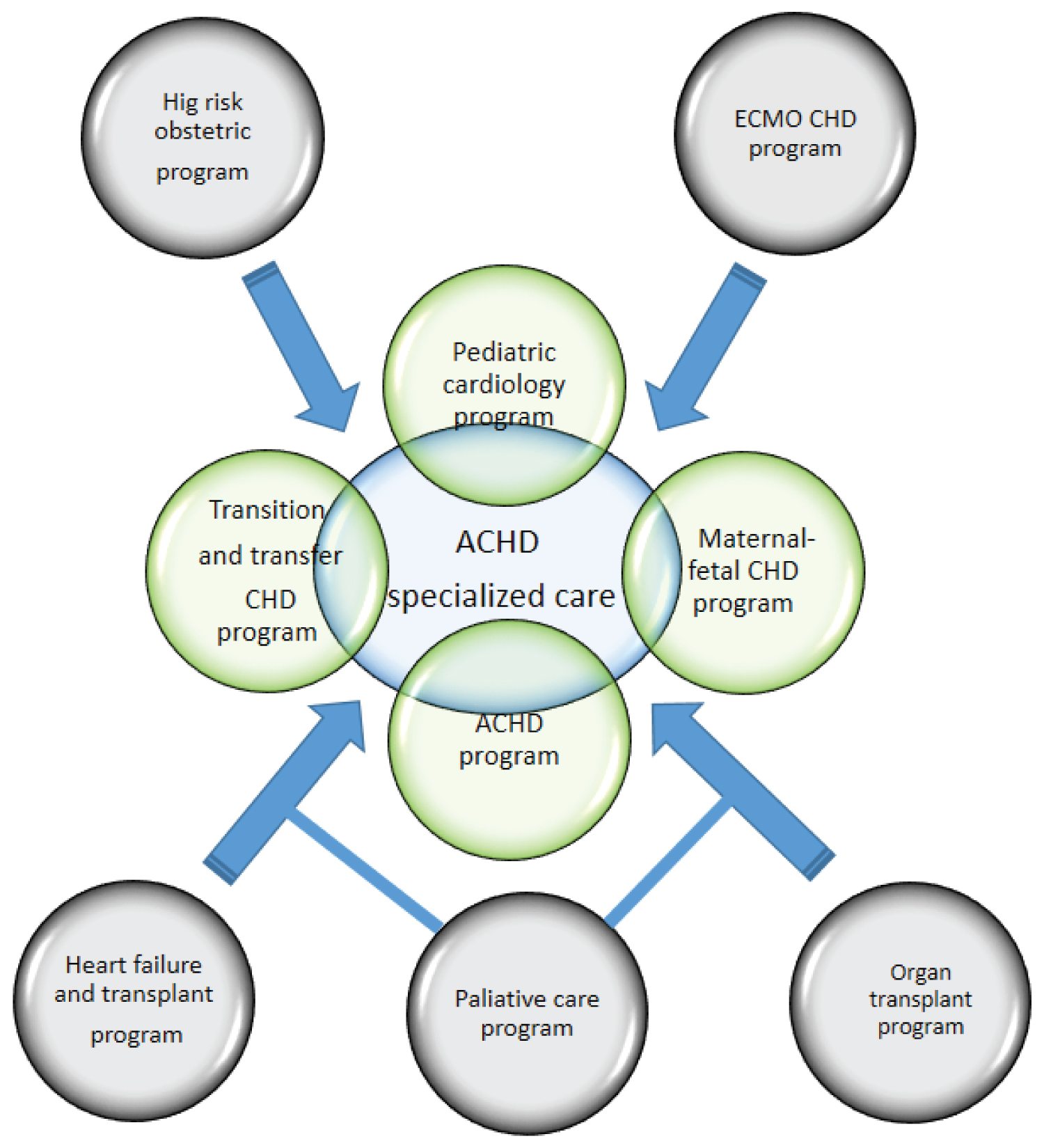 Figure 4: Creation of a comprehensive program for specialized ACHD care in light green color the four main programs that are supported by five complementary and parallel care programs in light gray color.
View Figure 4
Figure 4: Creation of a comprehensive program for specialized ACHD care in light green color the four main programs that are supported by five complementary and parallel care programs in light gray color.
View Figure 4
a) A maternal-fetal medicine program. Made up of specialists in maternal-fetal medicine, perinatology, pediatric cardiology, neonatology and cardiovascular surgery, this program has allowed us to diagnose CHD early and provide a timely response to many children born with CHDs who are repaired either surgically or through hemodynamic procedures at the cardiovascular center.
b) A pediatric cardiology program. With more than 100 surgeries per year, this program has helped solve various CHDs in the pediatric population, which are managed and followed throughout childhood.
c) An adult CHD program. This was one of the first in the country, and the first to have a lead specialist in ACHD with complete and official training in this specialty. With a vision to be a national referral center, we have been able to respond to and solve the problems of adult patients with CHD, and have become a leading and comprehensive program in Colombia.
d) A CHD transition and transfer program. As leaders in CHD care, all the recommendations and concepts of the respective international consensuses on the transition and transfer of pediatric patients to adult CHD care have been applied. A successful program has been developed with more than 90% of the patients seen in pediatric cardiology being followed in the ACHD.
The above programs are supported by five other complementary and parallel care programs in different cardiology and non-cardiology specialties, which involve various specialists needed for providing comprehensive ACHD care.
a) An extracorporeal membrane oxygenation (ECMO) program, the second in the region and sixth in the country. This program has specialized in pediatric and adult CHD support. It also has the only aerial ECMO unit in Colombia, thus providing the opportunity to care for any person in the country who needs it. The multidisciplinary team can travel by air to remote regions of the country, thanks to the strategic location of the center only 20 minutes away from the international airport. This has helped solve various critical situations in children and adults with not only CHD, but also other cardiopulmonary conditions meriting ECMO rescue.
b) A high-risk obstetrics program. This is one of the most solid programs in the region with a group of professionals in the field that, together with ACHD cardiology, has successfully resolved various obstetric problems in this population.
c) A palliative care program. Made up of a group of experts in this field, this program provides professional care in the final stages of life. With ACHDs in mind, the cardiovascular center is able to provide support in terminal situations.
d) A solid organ transplant program. This program was established with ACHDs in mind, especially those with complex cases and advanced anatomic and physiological classification (APC) stages. For ACHDs who need a solid organ (such as liver or kidney) transplant (for example, Fontan), the ACHD unit makes it available within the same institution, without having to be transferred to other institutions or regions of the country.
e) A heart failure and heart transplant program. This program is currently under construction and development. It
All the programs are supported by other inpatient services including intensive care units, a coronary care unit, and an emergency unit, supported by all the medical-surgical specialties (pulmonology, internal medicine, general surgery, orthopedics, clinical neurology, neurosurgery, and psychiatry, among others) of a tertiary care hospital.
Just as many other countries in the region, the tide of ACHDs has taken us by surprise, and currently in Colombian there are fewer than four ACHD care centers, and a much lower number of ACHD specialists. Due to this specialty's recent boom in our setting, some strategies had to be implemented to recruit and centralize ACHDs in our specialized center. In other words, instead of waiting for ACHDs to reach us, we go where they are. The strategies are as follows (Figure 5).
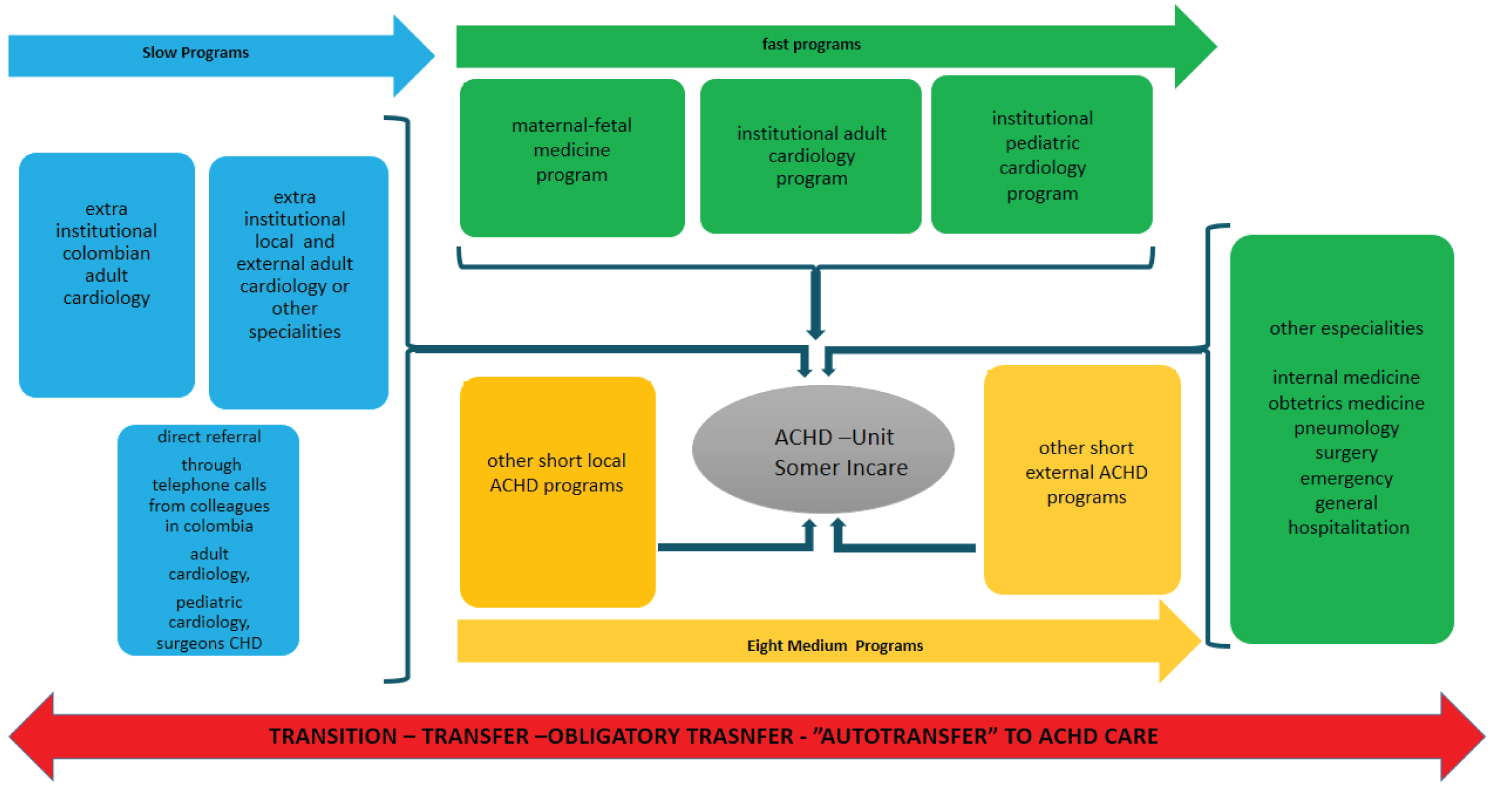 Figure 5: Strategies developed for the recruitment and centralization of ACHD care.
The fast, medium and slow recruitment paths of ACHD are summarized. Green color shows fast recruitment path. In yellow color medium recruitment path, local programs in ACHD are located close (less than 30 kilometers away and less than an hour by ground transportation) to the ACHD-Unit Somer In care, external programs at ACHD are located more than 30 kilometers away and more than an hour from the ACHD-Unit Somer Incare. In blue color slow recruitment path, these are programs in general and pediatric cardiology (external and local programs too). This also includes general cardiology programs from all regions of the country. This recruitment route is completed with cases referred through telephone calls from other colleagues in Colombia.
In all cases, transition and transfer are encouraged, as well as mandatory transfer in specific situations. Finally, the self-transmission strategy is applied as the team leader.
View Figure 5
Figure 5: Strategies developed for the recruitment and centralization of ACHD care.
The fast, medium and slow recruitment paths of ACHD are summarized. Green color shows fast recruitment path. In yellow color medium recruitment path, local programs in ACHD are located close (less than 30 kilometers away and less than an hour by ground transportation) to the ACHD-Unit Somer In care, external programs at ACHD are located more than 30 kilometers away and more than an hour from the ACHD-Unit Somer Incare. In blue color slow recruitment path, these are programs in general and pediatric cardiology (external and local programs too). This also includes general cardiology programs from all regions of the country. This recruitment route is completed with cases referred through telephone calls from other colleagues in Colombia.
In all cases, transition and transfer are encouraged, as well as mandatory transfer in specific situations. Finally, the self-transmission strategy is applied as the team leader.
View Figure 5
With this strategy, we seek to recruit the greatest possible number of ACHDs to be concentrated in ACHD Unit. Three main programs (pediatric cardiology, adult cardiology and maternal-fetal medicine) and other complementary specialized services are the rapid recruitment pathways.
All children with CHD who come of age are transferred to the ACHD unit, after passing through the transition program. Likewise, all ACHDs who are seen in the adult cardiology program are transferred to the ACHD unit. With regard to the maternal-fetal medicine program, while one of the objectives is to capture fetuses with CHDs to be repaired at birth, if required, we also seek out mothers or fathers who are CHD survivors, and direct them to our ACHD unit. In a complementary manner, all the other inpatient areas are sources of ACHD recruitment, as many of these patients are hospitalized for different non-cardiovascular causes, and many of them are even diagnosed with CHD for the first time during those hospitalizations.
There are other local ACHD recruitment programs which we call "medium recruitment" programs, and these are small ACHD care services which are also coordinated by the lead ACHD cardiologist at the cardiovascular center. These are specialized but not complete programs. There are eight programs altogether which have been developed in local and external hospitals, and which are a direct source of ACHD recruitment for the ACHD unit.
Finally, recruitment is complemented by programs not specialized in ACHD (slow recruitment), and these are general clinical cardiology, pediatric cardiology and other specialties which function within local hospitals and in other parts of the Colombian territory and which, for various reasons, care for ACHDs who arrive randomly at these centers. The medical staff working in these institutions are already familiar with our ACDH unit, and thus these ACHDs are referred from these sites for specialized care.
We have previously explained that one of the main problems in our region is losses to follow up, which exceed 60%. Therefore, our program has the goal of reducing these losses and having 100% of the pediatric patients who reach adulthood effectively transferred to the ACHD unit. This goal is being reached, and currently 90% of the patients who leave pediatric cardiology are followed in the ACHD unit.
This particular strategy was developed and mandatorily implemented in our center. Mandatory transfer consists in immediately referring any ACHD found. Thus, adult patients with CHDs who are not being seen in our ACHD unit and who for various reasons consult with echocardiography, cardiac rehabilitation, electrophysiology, clinical cardiology and other specialties, are immediately transferred that same day. This strategy is also applied in cases of incidental first-time CHD diagnoses in adults. This has undoubtedly changed the way of thinking of the various physicians who treat this population incidentally. We have also extended this strategy to the medium and slow recruitment programs, with a very good response and outcome.
Self-transfer is an effective strategy which has reduced losses to follow-up by almost 100%. Basically, as team leader have a double specialty (pediatric cardiology and ACHD specialist), so this potential allow me to manage both programs at the same time, making the transition from one program to the other less traumatic for new ACHDs.
This consists in telephone consults supported by online or video conference communication platforms, after telephone contact with different specialists assessing ACHDs in sites outside of our center. We agree by email to review the new ACHD's medical history, and then agree to conduct a video conference with the patient. Then we send a clinical concept by email and set up a programmed visit to the ACHD unit. We provide the time and space needed to conduct complementary non-invasive or invasive diagnostic tests to establish a deeper assessment and thus reach a more precise diagnosis of the current clinical condition, establishing a treatment plan, whether medical, interventionist or surgical, depending on the condition and APC class found. Finally, we set up a new on-site visit to carry out the agreed plan and return the patient to his/her place of origin in a better condition, to then be followed remotely through video chats.
Given the center's level, I consider it a duty to contribute to the development of the specialty in Colombia and LATAM. Thus, since the founding of the ACHD unit, more than 100 scholarly works have been produced including conferences, webinars, papers, interviews, editorials, and streaming, among others. The center's ACHD unit has been a leader in ACHD research and has participated in different international research projects [28,29]. The center's ACHD unit has a clinical and/or academic/advanced research commitment and participate in teaching on ACHD.
The ACHD population in Colombia has taken us by surprise. With more than 115,000 adults with CHD currently living in Colombia, we are facing big challenges in specialized care. The concentration of this population in ACHD units is a challenge for our region, not only due to few centers having this specialized capacity, but also due to the very limited number of specialists in this field. In Colombia, as in LATAM, we are developing the ACHD specialty simultaneously with ACHD units. This comprehensive model of ACHD specialized care is based on the opportunities and challenges we must face, and through the implementation of strategies using this model we have been able to reduce losses to follow up, and recruit and concentrate ACHDs. We are constantly growing and developing, projecting ourselves as a high-level ACHD unit in the region with clinical and academic commitment, advanced research and teaching on ACHD.