The search for possible topographic memory impairment in epileptic patients was carried out with the aim of better understanding the behavior of these patients and optimizing their neuropsychological accompaniment.
The method used is that of named Route Learning Task (RLT). It is a path learning task (topographic memory) that is based solely on learning a route composed of visual but non-verbal cues so that there is no influence of Examiner language or signposts on patient behavior. At a normal walking pace, the subjects had to travel a 10-minute loop in the cocody university hospital. The route (approximately 200 m) included 7 crossings that required an orientation decision. The examiner showed the route a first time and asked the subject to repeat the trip three times in a row, if the first two tests were not successful. For the duration of the task, the examiner noted the errors in orientation and pointed the subject in the right direction by saying "this is where you have to go".
Two (2) of the fifteen (15) healthy control subjects (13.33%) were test deficient (RLT). Four (4) of the ten (10) epileptic patients (40%) were test-deficient (RLT). The statistical analysis indicated a significant correlation between the total number of test errors (RLT) and the frequency of patient seizures (r = 0.65 p < 0.05); between EEG abnormalities and the total number of test errors (RLTs) in epileptic patients. However, no significant correlation was found between antiepileptic drugs and the total number of test errors (RLTs).
This study, in addition to highlighting real memory disorders in patients with generalized epilepsy, supports both the ecological validity of a commonly used clinical memory test.
Topographic memory, Epilepsy generalized, Ecological validity
CHU: Cocody University Hospital; RLT: Route Learning Task
Memory disorders are common in epileptic patients. Indeed, in addition to crises caused by seizures, epileptic patients often complain of memory problems. These deficits of memory often constitute the dominant complaint of this pathology. They are else, rightly, often, they have been marked by the behavior of the interictal period of epilepsy. They manifest to varying degrees through frequent forgetfulness, learning difficulties or problems memorizing a route that can significantly affect daily life. It should be noted that the patient's entourage does not necessarily perceive these difficulties and that the problems can therefore go relatively unnoticed. The identification of these disorders requires the use of standardized psychometric tests whose design is inspired by the theoretical frameworks of the neuropsychological. Thus [1,2] have found a working memory disorder in children with generalized epilepsy, respectively, with absence or a syndrome of Laudau-Klefner, using a countdown span test [3] also observed impaired working memory in adults with juvenile myoclonic epilepsy due to a working memory task. With regard to long-term memory [4] have by means of verbal and visual memory tests, shown memory problems in adults with generalized epilepsy. [5,6] reported verbal memory difficulties in children with epilepsy. [7,8] showed memory-related disorders of a visual nature in children with epilepsy. Although the evaluation of memory deficits by standard neuropsychological test batteries has been the subject of several studies in epileptic patients, on the other hand, the functioning of memory in people with epilepsy has rarely been studied in real-life situations. outside the clinic [9-11]. It is understood that ecological validity is essential for neuropsychology [12,13]. It is for all these reasons that we are proposed to investigate the topographic memory of people with epilepsy in natural environment. The objective of this study is to search for possible topographic memory impairment in epileptic patients was carried out with the aim of better understanding the behavior of these patients and optimizing their neuropsychological accompaniment.
The study described here covered 25 participants in both sexes. They were between 18 and 30-years-old. They were distributed as follows:
• 15 control subjects, with no history of neurological, psychiatric and stroke disorders. They were chosen from the general population.
• 10 patients with generalized epilepsy were recruited in the department of neurology of C.H.U of Cocody-Abidjan (Ivory Coast).
The method used is that of [9,12] named Route Learning Task (RLT). It is a path learning task (topographic memory) that is based solely on learning a route composed of visual but non-verbal cues so that there is no influence of Examiner language or signposts on patient behavior. At a normal walking pace, the subjects had to travel a 10-minute loop in the cocody university hospital. The route (approximately 200 m) included 7 crossings that required an orientation decision. The examiner showed the route a first time and asked the subject to repeat the trip three times in a row, if the first two tests were not successful. For the duration of the task, the examiner noted the errors in orientation and pointed the subject in the right direction by saying "this is where you have to go". The examiner made sure that the crossing of the streets was safe. The path is segmented into a set of segments with orientation decision points and for each decision point the choice is good (0) or erroneous (1).
In order to assess the RLT learning deficit at the individual level, we represented the total number of errors in the three trials according to the participants. To be in the Test Deficit (RLT) the total error score of the participants must be greater than 2.0 DS compared to the age-appropriate control mean. The subject is therefore deficient in the test (RLT) for the total number of errors greater than 4.
The general and pathological features were compared by a student test (t-test) for numerical values and by a chi-square test for categorical variables.
The matching of subjects to the level of study was based on the bachelor's degree (BAC = 12 years of study). The healthy control group includes two women out of eight men, while the epileptic group includes two women out of 13 men. As shown in (Table 1), both groups (control subjects, epileptic patients) do not differ in demographic characteristics. Indeed, statistical analysis shows that there is no significant difference in age, level of study and gender of participants. This result confirms that the two study groups have a homogeneous profile in terms of demographic characteristics. Only pathological features differ between the two groups.
Table 1: The general and pathological characteristics of the participants. View Table 1
The total number of errors during the three trials of the Road Test Learning Task (RLT), was in high epileptic patients compared to healthy controls. The total average error of healthy controls is M = 1.32; standard deviation = 1.6; the average of the group of epileptic patients M = 4.75; standard deviation = 4.2. To assess the learning deficit at the Learning test Road (RLT) test at the individual level, the total number of errors in the three trials was plotted against the participants (Figure 1). To be deficient in the test (RLT), the total error score of the participants must be greater than 4. Thus, two (2) of the fifteen healthy control subjects were test deficient (RLT). Four (4) of the ten (10) epileptic patients were test-deficient (RLT). The statistical analysis indicated a significant correlation between the total number of test errors (RLT) and the frequency of patient seizures (r = 0.65 p < 0.05); between EEG abnormalities and the total number of test errors (RLTs) in epileptic patients. However, no significant correlation was found between antiepileptic drugs and the total number of test errors (RLTs).
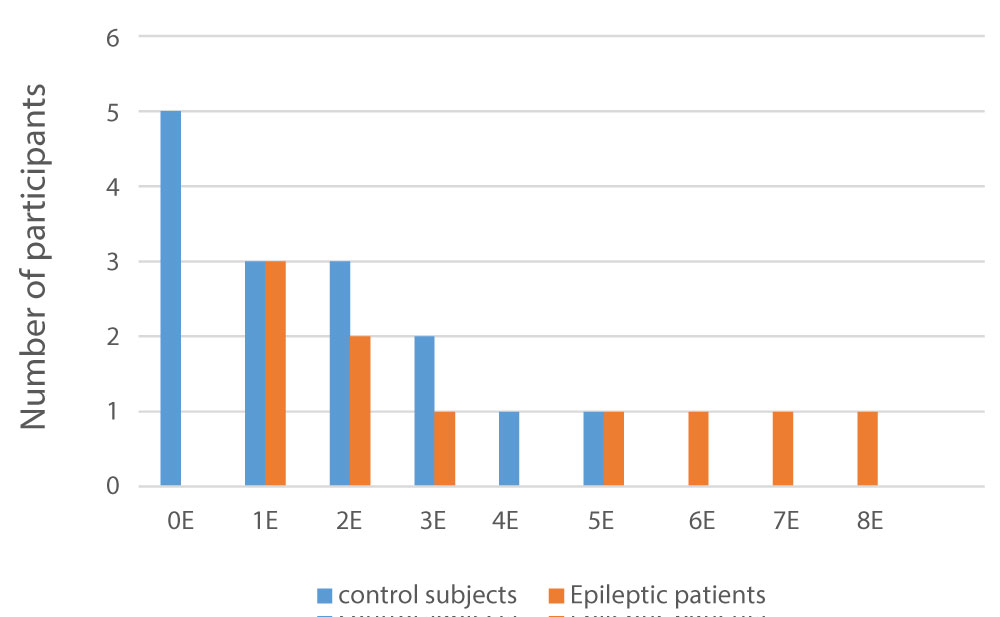 Figure 1: Total number of errors in the three trials by participants.
View Figure 1
Figure 1: Total number of errors in the three trials by participants.
View Figure 1
The evaluation of memory in patients with real-life epilepsy in a natural environment has been the subject of little study. As part of this study we tested the ability of epileptic patients and healthy control subjects to learn a route through the Cocody University Hospital Center. The topographic learning curves of the participants indicated that the average percentages of errors were significantly different from those of the healthy control subjects. In addition, the average percentages of epileptic patients' errors were high and remained almost identical during the three trials included in the trial. This result reflects a real difficulty for the epileptic group to learn and memorize a route. It confirms the studies of [11,14]. The first author in a similar study had a total mean error (M = 5.8 ± 4.1) for the group of epileptic patients versus (M = 1.7 ± 1.6) for controls. For the second author, epileptic patients were very poorly tested (RLT) compared to control subjects. In both studies, epileptic patients had temporal lobe epilepsy. This result is also to be compared with the study by [12,15]. who had a memory deficit of a route in brain-injured patients compared to controls. In order to assess the RLT learning deficit at the individual level, we represented the total number of errors in the three trials according to the participants. Thus, two (2) of the fifteen (15) healthy control subjects (13.33%) were test deficient (RLT). This result is comparable to that of [14] who obtained or (1) of (32) control subjects who were test deficient (RLT). As for epileptic patients, four (4) of the ten (10) epileptic patients were test deficient (RLT). It is close to the work of [12]. who reported (100%) of patients who were test deficient (RLT). This deficit was most regularly related to occipital mesial temporal and/or mesial lesion: Bilateral. Our results are also closer to the study by [14] of which (8) out of (19) or were test-deficient (RLT) patients, all of these patients had temporal lobe epilepsy. The statistical analysis indicated a significant correlation between the total number of test errors (RLTs) and patients' epileptic seizures. Indeed, the patients who had a high frequency of crisis, were deficient in the test (RLT). This result is close to the work of [16] which demonstrated the significant deleterious effect of status epilepticus, combined with generalized seizures on memory. It also showed that there was a significant correlation between EEG abnormalities and the total number of test errors (RLTs). Thus, patients with EEG abnormalities performed less well on the test (RLT). Our study is the first to highlight this correlation. These data are similar to those of [17] who observed a significant decrease in the scores of the test involving working memory in patients with epilepsy with rolandic paroxysms. The electroencephalogram of these patients showed very abundant abnormalities associated with a persistent slow focus. Finally, no significant correlation was found between antiepileptic drugs and the total number of test errors (RLTs). This result could be similar to the work of [18] who noted a lack of adverse effect of antiepileptics on short-term memory learning curves in epileptic patients.
While it is well established that patients with focal epilepsies generally have greater memory impairment than individuals with generalized epilepsies, they still have memory problems. These memory deficits have generally been evaluated by conventional standard neuropsychological tests on tables. In this study we assessed the memory of patients with generalized epilepsy and healthy control subjects in real-life situations (real world) using the route learning task (RLT). Patients with generalized epilepsy were at this test (RLT) compared to control subjects. Patients with generalized epilepsy were at this test (RLT) compared to control subjects. The study showed a significant correlation between the total number of test errors (RLT) and epileptic seizures of patients; between the EEG anomalies and the total number of test errors (RLT). Finally this study, in addition to highlighting real memory disorders in patients with generalized epilepsy, supports both the ecological validity of a commonly used clinical memory test.