Type 2 Diabetes (T2D) is a chronic progressive disease, and its prevalence is on the rise around the world. Despite advances in pharmacotherapy, mitigating the burden of the disease on individuals, societies and the healthcare system remains a challenge. Remission has emerged as a therapeutic target in T2D with wide range of interventions. A plant-based diet seems to be promising to achieve this goal.
The present study is conducted to establish the feasibility of achieving remission of type 2 diabetes with a plant-based diet in a cohort of free-living individuals.
This cohort of patients were referred to our Wellness Clinic for management of various cardiovascular conditions and associated metabolic disorders. They were educated and counseled to adopt a plant-based diet while receiving standard medical treatment. The present study included non-pregnant adults 20 years and older, mostly elderly, with the diagnosis of T2D (HbA1c > 6.5%), with or without on antidiabetic medications. The remission of diabetes is defined as improving HbA1c to < 6.1%, without antidiabetic medications except metformin.
The cohort is composed of 83 patients with mean age 70.1 (SD +/- 9.64) years and 36% were women. The results are reported as disease status at the time of diagnosis (1), disease status immediately prior to adoption of diet (2), and disease status post diet at 3-6 months (3), and disease status post diet after 6 months (4) (Table 1). For comparison, the averages of the two pre-diet parameters and the averages of the two post-diet parameters are given in this summary (Table 2). These are - BMI (kg/m2) 32.93 has changed to 29.85, a decrease of 3.08 (-9.35%) with p < 0.0000, systolic blood pressure (mm of Hg) 133.21 has changed to 131.09, a decrease of 2.12 (-1.59%) with p = 0.1054, diastolic blood pressure (mm of Hg) 74.81 increased to 73.02, a decrease of 1.79 (-2.39%) with p = 0.2592, Hemoglobin A1c 7.3% changed to 5.82%, a decrease of 1.48 points (-20.27%), p < 0.0000, fasting glucose (mg/dl) 137.30 changed to 108.53 mg/dl , a decrease of 28.77 points (-20.95%), p < 0.0000, HDL cholesterol (mg/dl) 44.44 changed to 45.01, an increase of 0.66 points (+1.49%), p 0.4841, LDL cholesterol (mg/dl) 84.08 changed to 74.43, a decrease of 9.65 points (-11.48%), p 0.0011, Triglyceride (mg/dl) 164.48 decreased to 122.47, a decrease of 42.01 points (-25.54%), p 0.0149.
Table 1: Participant characteristics and metabolic outcomes. View Table 1
Table 2: Comparison of parameters before and after plant-based diet. View Table 2
A plant-based diet has been successful in achieving remission of type 2 diabetes in this group of patients, even in their advanced age.
Type 2 diabetes (T2D) remission, Plant-Based diet, Body Mass Index (BMI), HbA1c, Antidiabetic medications
Diabetes is the most prevalent non-communicable disease (NCD) in the world. In the US, from 2001 to 2020 the incidence of diabetes has significantly increased in adults 18 or older. That is 37.3 million people have diabetes which is 11.3% of US population [1]. Moreover, there is an asymptomatic phase (prediabetes phase) which gradually progresses to overt type 2 diabetes (T2D) over time where lifestyle changes will have a profound and positive effect in prevention [2].
The epidemics of diabetes mellitus and its complications poses a major threat to global health. The International Diabetes Federation (IDF) estimated that 1 in 11 adults aged 20-79 years (415 million adults) had diabetes mellitus globally in 2015. This estimate is projected to rise to 642 million by 2040. Over 90% of diabetes mellitus cases are T2D [3]. The Global Burden of Disease (GBD) Study provides a comprehensive picture of the potential impact of suboptimal diet on NCD mortality and morbidity, highlighting the need for improving diet across nations [4]. Foods high in carbohydrates are an important part of healthy diet since they provide the body with glucose to support bodily functions and physical activity. However, the consumption of refined, simple, and low-quality of carbohydrates has direct implication for most of the present chronic diseases [5].
Diabetes is a chronic and progressive disease. It leads to high incidence of complications affecting many organs -cardiovascular disease, retinopathy, nephropathy, neuropathy, peripheral vascular disease, ischemic gangrene, limb amputation, stroke, and causing substantial morbidity and mortality. In addition, it adds to a huge economic burden to the society [6]. Evidence shows that nutrition therapy improves glycemic control and reduces the risks of diabetes and its complications [7].
Despite many advances in the pharmacologic management of T2D, the incidence of diabetes has not abated. Consequently, there is an urgent need to acquire simple solutions, easily obtainable and widely available to counter this trend. In this regard, an appropriately planned, nutritionally rich, whole food plant-based diet has been found to be promising in preventing and reversing T2D [8]. In the present study, we report the success of plant-based diet in a group of free-living patients achieving remission of T2D, even in their advanced age.
In the cardiovascular wellness clinic, we treat patients with heart disease, hypertension, hyperlipidemia, obesity, and diabetes. The present study is the outcome on patients achieving remission of T2D by adopting a plant-based diet. They all have given consent for the participation and reporting. They are educated on the merits of adopting a plant-based diet to treat, reverse and prevent the major risk factors to avoid the complications associated with diabetes. First off, they are introduced to the AHA’s Simple 7 guidelines to maintain a good health [9]. They are - (1) To avoid all tobacco products, (2) To maintain ideal BMI (body mass index in kg/m2) of less than 25, (3) Regular exercise of minimum 150 minutes per week, (4) A vegetarian diet (Whole Food Plant-Based Diet), (5) To achieve a total cholesterol of less than 200 mg/dl, triglyceride 150 mg/dl, HDL cholesterol greater than 40 mg/dl for men and 50 mg/dl for women, LDL cholesterol less than 100 mg/dl, without medications, (6) A blood pressure of 120/80 mm of Hg, without medications, and (7) Fasting blood glucose of less than 100 mg/dl (HbA1c < 6.0%), without medications.
The first encounter comprises of an hour of consultation. They all receive an intense education on the principles of reversing T2D with a plant-based diet. This consists of vegetables, legumes, whole grains, fruits, nuts, and seeds. On this diet, 75% of calories are derived from complex carbohydrates, 15% from protein (plant), and 10% from fat (Figure 1). Moreover, they are fiber-rich and filled with phytochemicals, polyphenols, antioxidants, vitamins, and minerals. They are to avoid all animal-derived products, processed foods and added oils. A small quantity of egg white and no-fat dairy is allowed for occasional use. A glass of red wine for women and maximum of two glasses for men are allowed for most days of the week. However, if weight loss is the primary goal, use of alcohol is discouraged. They are educated on the importance of consuming high fiber, whole food plant-based diet which leads to weight loss, decrease in visceral fat, improves insulin sensitivity, reduce blood glucose, and improves complications related to diabetes. In addition, they are counseled to achieve ideal body weight where applicable with a calorie-restricted (CR) diet plan of 1200 to 1600 calorie per day, and to participate in regular exercise for at least 150 minutes per week. They are provided with teaching materials in the form of leaflets, brochures, meal plans, and other resources to improve their learning and adoption of this lifestyle. They are particularly impressed upon avoiding all animal-derived products and processed foods which are high in saturated fat, cholesterol and are energy dense. In addition, they are counseled to avoid refined carbohydrate products, salty snacks, and sugar-sweetened beverages. Generally, they return for the second clinic visit in about 6 to 12 weeks with repeat evaluation of blood chemistries which include fasting lipids, blood glucose, HbA1c, renal function, and hepatic function, and in selective cases c-peptide and insulin (free and total) levels. During this clinic visit, their clinical progress is compared to the previous findings and additional counseling is provided on the areas where they have not made satisfactory progress, taking into consideration of the 7 metrics of AHA, as outlined above. There after they return in every 3 to 6 months, depending on their progress, for close follow-up, monitoring and to provide encouragement for compliance.
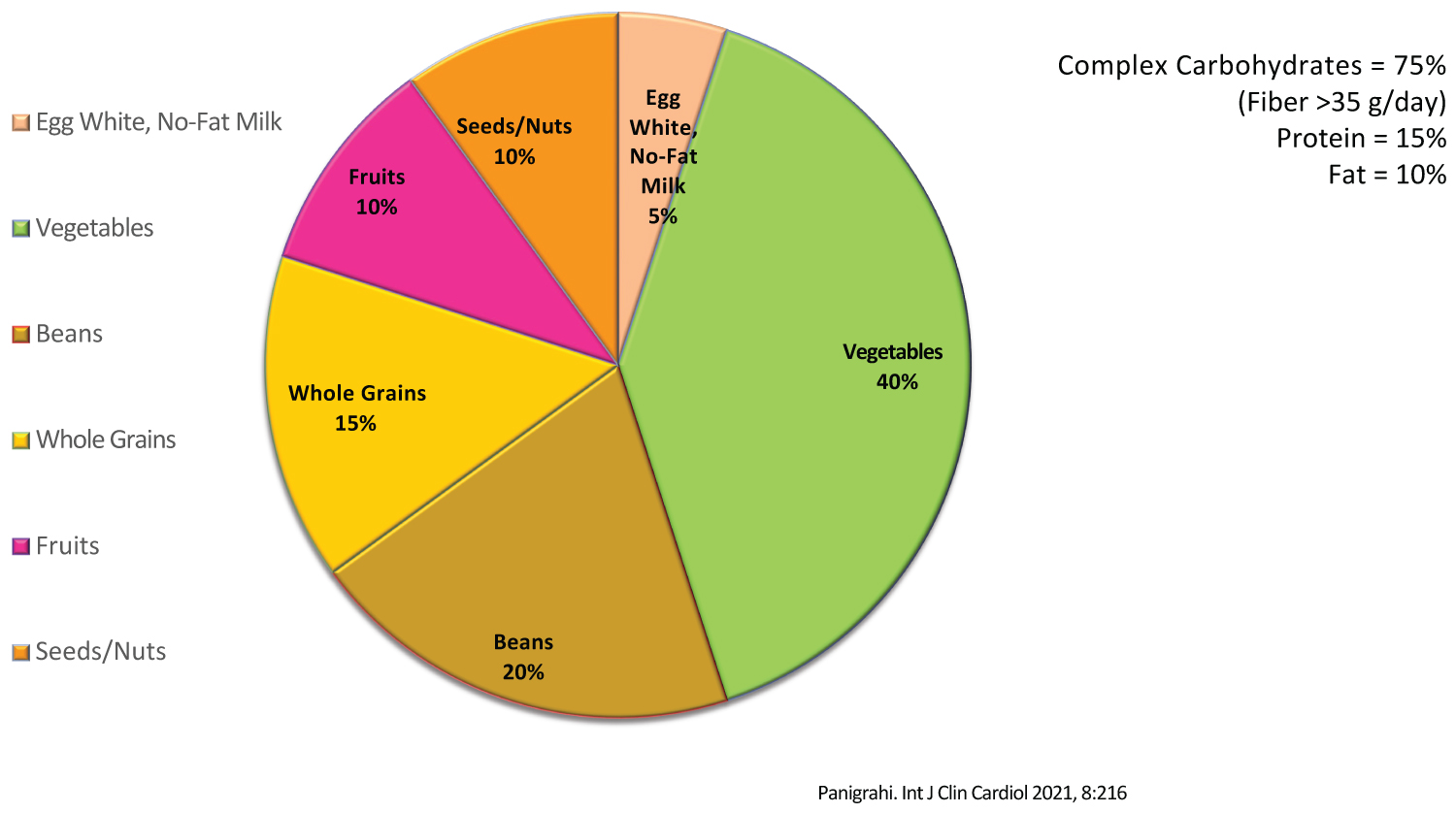 Figure 1: Dietary and nutrient composition of intervention diet.
View Figure 1
Figure 1: Dietary and nutrient composition of intervention diet.
View Figure 1
The standard deviation (STD) and standard error (SE) of mean were calculated utilizing formula in the Microsoft Excel program. The Student’s T-Test was utilized to calculate the p values. The p value < 0.05 is considered statistically significant.
This cohort of comprise of 83 patients with T2D, with an average age of 70.1 years (SD +/- 9.64), and 36% are women. The outcome data are summarized in Table 1. They are, at the time of diagnosis of diabetes.
The average BMI (kg/m2) was 32.83 ( SE +/- 0.7), systolic blood pressure was 135.98 mm of Hg (SE +/- 2.15), diastolic blood pressure was 76.52 mm of Hg (SE+/- 1.22), HbA1c was 7.4% (SE +/- 0.16), fasting blood glucose was 136.59 mg/dl (SE+/- 4.74), HDL cholesterol was 44.93 (SE +/_ 1.39), LDL cholesterol was 88.08 mg/dl (SE +/- 3.46), triglyceride (*patients (n = 2) with triglyceride level > 500 mg/dl are excluded for this analysis) was 151.74 mg/dl (SE +/- 8.23), triglyceride (**participants (n = 2) with triglyceride level > 500 mg/dl are included in this analysis) was 173 mg/dl (SE +/- 22.94). Before adopting the lifestyle of plant-based diet.
The BMI (kg/m2) was 33.02 (SE +/- 0.76), systolic blood pressure was 130.44 mm of Hg (SE +/- 2.04), diastolic blood pressure was 73.10 mm of Hg (SE +/- 1.22), HbA1c was 7.19% (SE +/- 0.12), fasting glucose was 138.01 mg/dl (SE +/- 4.67), HDL cholesterol was 43.94 mg/dl (SE +/- 1.28), LDL cholesterol was 80.09 mg/dl (SE +/- 4.09), triglyceride (*participants (n = 4) with triglyceride level > 500 mg/dl are excluded from this analysis) cholesterol mg/dl was 142.19 mg/dl (SE +/- 9.53), triglyceride (**participants (n = 4) with triglyceride > 500 mg/dl are included in this analysis) was 155.61 mg/dl (SE +/- 13.05).
The BMI (kg/m2) is 30.52 (SE +/- 0.65), systolic blood pressure is 132.44 mm of Hg (SE +/- 2.02), diastolic blood pressure is 75.01 mm of Hg (SE +/- 1.14), HbA1c is 5.79% (SE +/- 0.03), fasting glucose is 106.28 mg/dl (SE +/- 2.0), HDL cholesterol is 44.84 mg/dl (SE +/- 1.38), LDL cholesterol is 75.11 mg/dl (SE +/- 3.21), triglyceride (*) cholesterol is 127.95 mg/dl (SE +/- 6.61), and triglyceride (**) 127.95 mg/dl (SE +/- 6.61) .
The BMI (kg/m2) is 29.19 (SE +/- 0.74), systolic blood pressure is 129.74 mm of Hg (SE +/- 2.12), diastolic blood pressure is 71.02 mm of Hg (SE +/- 1.13), HbA1c is 5.86% (SE +/- 0.05), fasting glucose is 110.78 mg/dl (SE +/- 2.66), HDL cholesterol is 45.36 mg/dl (SE +/- 1.66), LDL cholesterol is 73.74 mg/dl (SE +/- 3.53), and triglyceride (*) cholesterol is 116.98 mg/dl (SE +/- 8.13), and triglyceride (**) was 116.98 mg/dl (SE +/- 8.13).
The statistical analysis between the periods of observations is summarized in Table 1. Briefly, between the observations of 1 vs. 3, 1 vs. 4, 2 vs. 3, and 2 vs. 4, the BMI, HbA1c, fasting blood glucose, HDL, LDL, and triglyceride parameters are all statistically significant with p value < 0.05. The systolic and diastolic blood pressure, and HDL cholesterol levels are not statistically significant. But again, they all are in the normal range, meaning under good control.
The comparisons of the combined averaged parameters before and after plant-based diet are given in Table 2. They revealed the following: the BMI (kg/m2) has decreased from 32.93 to 29.85, a decrease of 3.08 (-9.35%) with p value < 0.0000, systolic blood pressure has decreased from 133.21 to 131.09 mm of Hg, a decrease of 2.12 mm of Hg (-1.59%) with p value 0.1054, diastolic blood pressure from 74.81 to 73.02 with a decrease of 1.79 mm of Hg (-2.39%) with p value of 0.2592, the HbA1c has decreased from 7.30% to 5.82%, a drop of 1.48% (-20.27%) with the p value of < 0.0000, fasting glucose decreased from 137.30 mg/dl to 108.53 mg/dl, a drop of 28.77 mg/dl (-20.95%) with the p value of < 0.0000, HDL cholesterol of 44.44 mg/dl has increased to 45.10 mg/dl to an increase of 0.66 mg/dl (+1.49%) with a p value of 0.4841, LDL cholesterol has decreased from 88.08 to 74.43 mg/dl with drop of 9.65 mg/dl (-11.48%) with a p value of 0.0011, triglyceride (*) decreased from 146.97 mg/dl to 122.47 mg/dl, a drop of 24.50 mg/dl (-16.67%) with p value of 0.0003, and triglyceride (**) decreased from 164.48 mg/dl to 122.47, a drop of 42.01 mg/dl (-25.54%) with the p value of 0.00149.
In other words, BMI, HbA1c, fasting blood glucose, LDL cholesterol, triglyceride cholesterol has significantly improved with plant-based diet. The systolic and diastolic blood pressure, and HDL cholesterol though have improved, but are not statistically significant.
The relationship between BMI and HbA1c is illustrated in Figure 2. This explains how modest weight loss parallels in improving glucose homeostasis. Similarly, the relationship between fasting blood glucose (FBG) and LDL cholesterol level is depicted in Figure 3, achieved with plant-based diet.
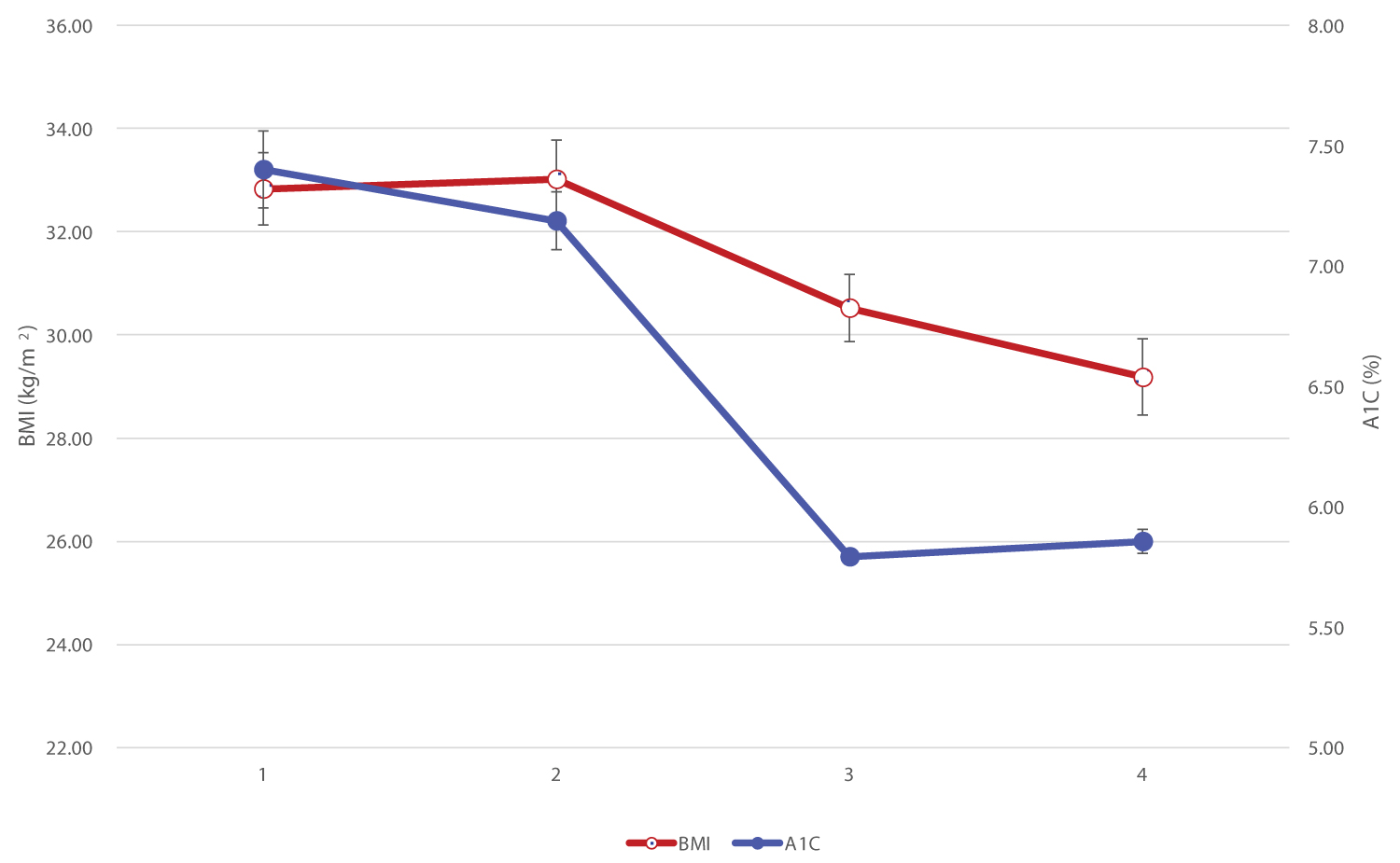 Figure 2: Relationship of BMI vs. HbA1c.
View Figure 2
Figure 2: Relationship of BMI vs. HbA1c.
View Figure 2
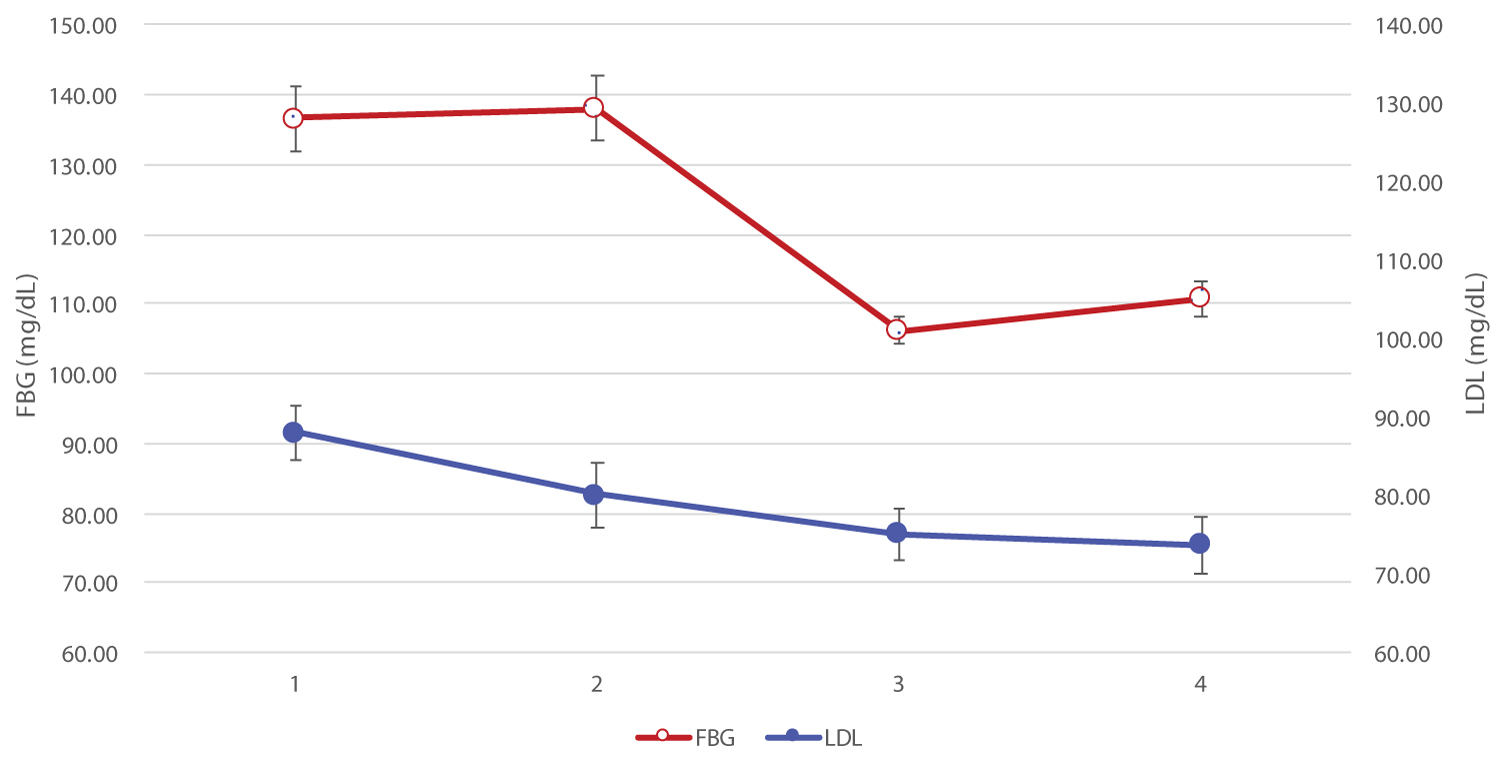 Figure 3: Relationship of FBG vs. LDL Cholesterol.
View Figure 3
Figure 3: Relationship of FBG vs. LDL Cholesterol.
View Figure 3
The above salutary benefits are accompanied with a decrease in the number of antidiabetic medications (Table 3 and Figure 4), which are statistically significant. Importantly, participants are off insulin and the sulfonylurea agents which are known to cause weight gain (and in the long run exacerbate blood glucose control).
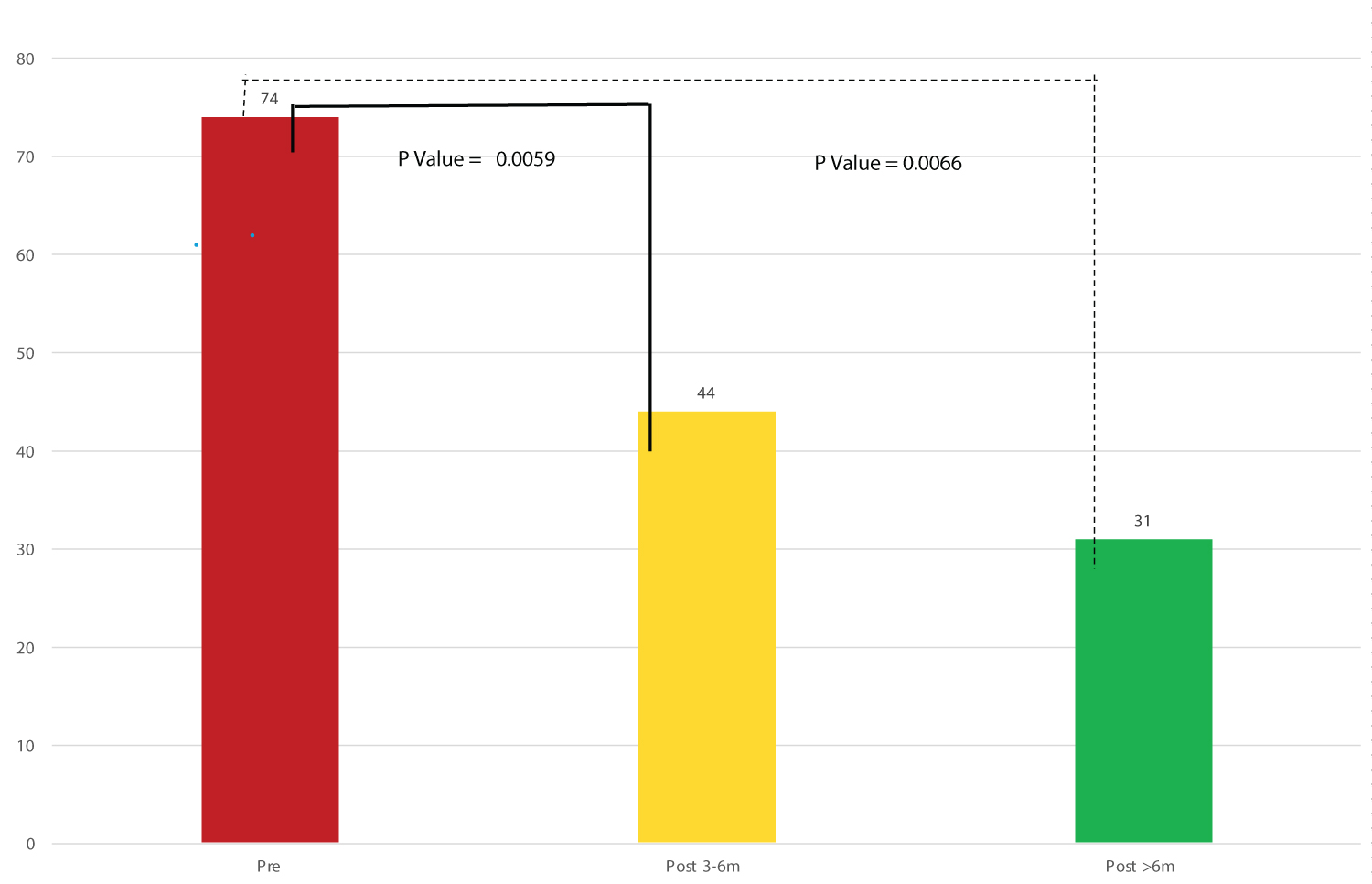 Figure 4: Use of anti-diabetic medication before and after plant-based diet.
View Figure 4
Figure 4: Use of anti-diabetic medication before and after plant-based diet.
View Figure 4
Table 3: Use of anti-diabetic medication before and after plant-based diet. View Table 3
Remission of T2D has emerged as a therapeutic goal in T2D management. The DIRECT study has shown that a low-energy diet of 800-1200 kcal per day achieved T2D remission in 46% of participants. A significant reduction in body weight, especially greater than 15 kg compared to baseline, was highly predictive of remission of T2D [10,11]. Remission of diabetes early after diagnosis appears to reduce the risk of complications. But this is not universal due to a biochemical phenomenon described as "metabolic memory", alternatively known as the "legacy effect" [12]. But aggressive blood glucose control long-term showing promising results in preventing cardiovascular events [13]. Remission of diabetic macular edema by remission of type 2 diabetes with plant-based diet has been achieved [14]. However, maintaining long-term remission requires continuous medical supervision and support from healthcare providers through personalized approach [15]. A nutritional approach to and prevent diabetes has been long recognized by endocrine societies [16,17]. Moreover, consumption of vegetarian diets has been found to be successful in improving glycemic control in T2D [18]. Similarly, a vegetarian diet in the Adventist Health Study 2 found lowest incidence of T2D in vegans (2.9%), compared to non-vegetarians (7.6%) [19].
Modest weight loss (10%) has been associated with impressive glycemic control, improvement in blood pressure and lipids [20]. In a trial with very low-fat (10% of energy) vegetarian diet, fasting blood glucose fell by 24%, serum cholesterol fell over 20%, triglyceride fell by 30%. The weight loss was also significant, over 4 kg over 26 days [21]. In this study, similar results are achieved.
In epidemiologic studies from large perspective observational studies and randomized clinical trials indicate that many cases of T2D could be prevented by maintaining healthy weight with a focus on maintaining energy balance by engaging in regular physical activity and consuming a healthy diet. Dietary practice of consuming naturally occurring dietary fiber in whole grains, vegetables, legumes, and fruits have been successful in reducing blood glucose [22].
A high-fiber diet has multiple health promoting benefits. First, this diet has low calorie density and is rich in nutrients. As a result, it has a profound salutary effect in its digestive, metabolic, antidiabetic, hormonal, anti-inflammatory, and immune enhancing abilities. The beneficial effects of high fiber diets - > 25 g/d in women and > 38 g/d for men, is attributed due to mainly their viscous and/or gel-forming properties of soluble fiber [23]. Chandalia and their group found significant beneficial effects on glucose homeostasis and insulin secretion in diabetic population who increased their dietary fiber intake to 25g soluble and 25g insoluble fiber daily [24]. Furthermore, fiber nutritionally supports the vast intestinal anerobic microbes which by fermentation produce short-chain fatty acids (SCFA), the health promoting compounds. SCFA maintain the health and integrity of the enterocytes, suppresses the growth of disease-causing microbes by maintaining the colonic acidity. A healthy intestinal mucosal barrier prevents "leaky gut syndrome", which in turn prevents endotoxin absorption. Endotoxins are responsible for chronic systemic inflammation, leading to obesity, insulin resistance, metabolic syndrome, and diabetes [25,26].
Grains account for 25% of the energy consumption in the US. Refined grains are stripped off their bran and germ, thereby deplete many biologically active nutrients and constituents, including fiber, antioxidants, minerals, and phytosterols. The high concentration of fiber and indigestible carbohydrates present in whole grains are fermented in the large intestine by endogenous bacteria, thereby producing SCFAs, and they enter the portal circulation. There is evidence that the hepatocytes when exposed to an increased SCFA, increase glucose oxidation, decrease fatty acid release, and increase insulin clearance - an environment conducive to enhanced insulin sensitivity. A whole-grain, high-fiber diet could therefore enhance insulin receptor sensitivity through chronic lowering of the overall dietary glucose load and related need of insulin secretion [27]. In addition, the ingestion of whole grains and legumes are known to reduce postprandial blood glucose, not only at the meal which they were consumed but also at subsequent meals. This is called the "subsequent meal effect" or sometimes "second meal effect"- which has important implication for day-long blood glucose control and prevention of diabetes [28].
The gut-microbiota benefits humans via short-chain-fatty acids (SCFA) production from carbohydrate fermentation, and a deficiency in SCFA production has been found to be associated with T2D. In a randomized clinical study of specifically designed isoenergetic diet, together with shotgun metagenomics to show that a select group of SCFA producing strains was promoted by dietary fibers and most other potential producers were either diminished or unchanged in T2D. When the fiber-promoted SFA producers were present in greater diversity and abundance, participants had better improvement in hemoglobin A1c levels, partly via increased glucagon-like peptide-1 production. Promotion of these positive responders, diminished producers of metabolically detrimental compounds such as indole and hydrogen sulfide. Targeted restoration of these SCFA producers may present a novel ecological approach for managing T2D [29].
Gut peptides, exemplified by glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are secreted in a nutrient-dependent manner and stimulate glucose-dependent insulin secretion. Both GIP and GLP-1 also promote beta cell proliferation and inhibit apoptosis, leading to expansion of beta cell mass. GLP-1 controls glycemia via additional actions on glucose sensors, inhibition of gastric emptying, food intake, and glucagon secretion. Furthermore, GLP-1 potently stimulates insulin secretion and reduces blood glucose in human subjects with T2D [30,31].
The dietary fiber in addition provides phytosterols and stanols which prevent absorption of intestinal cholesterol. They are derived from the plant source of whole grains, legumes, vegetables, fruits, seeds, and nuts. The National Cholesterol Education Program (NCEP) recommends 2 grams of phytosterol and stanols a day to lower blood level of LDL cholesterol. At high intestinal plant stanol concentrations, cholesterol loses its micellar solubility possibly by its replacement of free fraction in the micellar phase by hydrolyzed plant stanols, and this leads to a decreased intestinal absorption of cholesterol [32]. In a dose escalation trial, the LDL-cholesterol lowering effect of plant sterols and stanols across different range continued to increase up to intakes approximately 3 g/d to an average effect of 12% [33].
Nutritional recommendations emphasize fruits and vegetables consumption. This is related to health-benefits associated with bioactive nutrient molecules (vitamins, minerals, fiber, etc.) as well as non-nutritive phytochemicals (phenolic compounds, flavonoids, and other bioactive peptides) content of this group of foods. They have pleotropic health-benefits - anti-inflammatory, immune enhancing, improving blood pressure, reducing heart disease, enhancing brain function, and in reducing cancer cell growth. So, incorporating these diets daily are beneficial [34].
The currently available information suggests that CR reduces the risk of developing T2D and atherosclerosis [35]. In addition, it extends to other beneficial effects in reducing obesity, hypertension, and late complications of heart disease, stroke, and neurodegenerative disorders [36]. Furthermore, intermittent fasting or time restricted feeding leads to many health benefits by reducing the demand on insulin production and release [37]. Also, intermittent fasting confers resilience via activation of NRF2 (nuclear factor-erythroid 2 p45-related factor 2), AMPK (adenosine 5’ monophosphate-activated protein kinase), PGC1-a (peroxisome proliferator-activated receptor-gamma coactivator -1 alpha) and FOXO (Fork head box O) pathways, but also time-restricted feeding, enhances circadian regulation of gut microbiome and down regulation of mTOR pathway, which is useful in many disease states, including diabetes, obesity, autoimmunity, cancer, and neurodegeneration [38,39].
In the observational and cohort studies in type 1 and type 2 diabetes, intensive medical management has reduced microvascular complications, but the outcome benefits for macrovascular complications are conflicting [12,13]. This is attributed due to glycemic "metabolic memory "or the "legacy effect". However, the Veterans Administration Diabetes Treatment (VADT) study showed intensive medical treatment for 5.6 years resulted in 1.5% drop in HbA1c (from 8.4% to 6.9%) and 17% decrease in cardiovascular events, compared to the standard medical treatment group, which was statistically significant. After the intensive medical treatment was stopped, the HbA1c rose and in 3 years it reached the same level as the standard treatment group of about 8.0%. At this point of 15-years of follow-up, there was no difference in cardiovascular events between these two groups. This indicated there is no permanent legacy effect, rather the withdrawal of intensive treatment in 3 years led to concomitant rise in HbA1c and so also the increased cardiovascular events. This suggested just the preceding 3 years contributed to the increased cardiovascular events. However, the intensive medical treatment was associated with higher incidence of hypoglycemia and increased weight gain, a common side effect of most used of antidiabetic medications (for example: insulin and sulfonylurea) [40]. This poses a limitation to accrue long-term cardiovascular benefit with intensive medical treatment. In the present study, plant-based diet has contributed simultaneously to the decrease in weight and HbA1c with reduction in the use of medications (off insulin and sulfonylurea). So, to counter the legacy effect of diabetes (hyperglycemia) does not seem to be altogether hopeless. On the other hand, if plant-based diet can be adopted early and followed long-term, in these vulnerable groups of patients, there will be an expected reduction in cardiovascular morbidity and mortality. This has been the experience from the dietary practices of the population in Okinawa centenarians [41]. But a longitudinal study on remission of T2D based on a plant-based diet as a primary intervention remains unknown [42].
A plant-based diet resulting in weight loss, decreased fasting blood glucose and HbA1c to a level achieving remission of T2D without most of the antidiabetic medications. Secondly, dietary cholesterol found only in animal foods (and no fiber), while fiber only inplant-based foods (and no cholesterol) decreased LDL and triglyceride cholesterol levels and reduced blood pressure, ultimately reducing cardiovascular risks. Thirdly, with a hopeful note, the legacy effect of diabetes may not be a permanent condition, and a plant-based diet is poised to confer immediate and long-term benefits with reduction of microvascular and macrovascular complications.
Not applicable.
A part of this study has been contributed to the research project of the American College of Lifestyle Medicine titled - "Remission of Type 2 Diabetes with Plant-Based Diet".
The author thanks Stephen G. Manga, MS and Sally M. Goodwin for their assistance in preparation of this manuscript.