Background: The blood glucose level in a patient with diabetes is an important prognostic factor for any form of severe illness requiring intensive care hospitalization. We conducted this retrospective study to examine the effect of hyperglycemia on outcomes in patients with diabetes with coronavirus diseases (COVID-19) admitted to the intensive care unit (ICU).
Method: A retrospective analysis of 25 adult patients with diabetes with COVID-19 admitted to the ICU between 1st January to 15th February 2021 was done. Demographics details, past medical history, random blood sugar, medical management, ventilatory requirements, and survival data were obtained from medical record files and computerized patient recording systems. Outcomes such as mortality, need for mechanical ventilation, length of ICU stay, and length of hospital stay were analyzed.
Result: The median age of the patients was 61 years with a male preponderance. Hypertension is the most common co-morbidity associated with diabetes patients. The median blood sugar level was consistently high in the non-survivors although the result was not statistically significant. Clinical management showed that 84% of patients received insulin, 16% (oral hypoglycemic agents) 72% (steroids) and (64%) mechanical ventilation. The median ICU stay was 8(2-72) days, the median hospital stay was 13(6-79) days and overall mortality in patients with diabetes with COVID-19 was 52%.
Conclusion: Hyperglycemia in critically ill COVID-19 patients with preexisting diabetes shows worst outcome in terms of complications, need for mechanical ventilation, and mortality a well-designed prospective study is needed to determine the optimal target for glucose control and its effect on outcomes in patients with diabetes and COVID-19.
COVID-19 retrospective, Diabetes, ICU, Hyperglycemia
Coronavirus diseases (COVID-19) presentation ranges from mild to severe disease, with approximately 5-10% of patients may require intensive care unit (ICU) admission, particularly those with advanced age and multiple comorbidities [1]. India has become the diabetic capital of the world, with a prevalence of 8.7% in the adult population [2]. Multiple studies have been conducted to analyze the factors associated with poor outcomes in COVID-19 patients. Diabetes is often associated with poor outcome in several diseases. In previous SARS and influenza pandemic it was reported that uncontrolled blood sugar value was associated with both the disease severity as well mortality in the infected patients [3,4]. The impact of blood sugar, especially uncontrolled value on the severity of COVID-19 is unknown. An analysis of 11 studies, which evaluated biochemical abnormalities of COVID-19 patients revealed no correlation with blood glucose levels and diseases severity [5].
But few studies on mortality and severity of diabetic patients, reported that patients with poorly controlled hyperglycemia (blood glucose level > 180 mg/dl) have worst outcome in comparison to well controlled in a COVID-19 patients [6]. Further, it is found that age, sex, obesity, comorbidities such as hypertension, chronic kidney disease, pulmonary and liver diseases and laboratory parameters such as d-dimer, lymphopenia, neutropenia, interleukin 6 (IL-6), serum ferritin, and prothrombin time, might predict outcomes in patients with COVID-19 [7-9].
Hyperglycemia is one of the modifiable factors which is associated elevated risk of mortality in COVID-19 patients [10]. Recent evidence suggests that hyperglycemia in COVID-19 patients has a poor outcome and if it is associated with diabetes, it further increases the length of hospital and ICU stays and the risk of mortality [10]. Therefore, our study analyzed the effect of hyperglycemia on outcomes in COVID-19 patients with known diabetes admitted to the intensive care unit in a tertiary care hospital.
The study was conducted in the intensive care unit at a tertiary care hospital, designated as the COVID-19 Centre by the Indian Government. The retrospective data presented in this study were part of a project approved by the Institute Ethics Committee (IEC-291/17.04.2020). Since the study was retrospective, the requirement for informed written consent from individual patients was waived.
The study included confirmed COVID-19 patients with diabetes admitted to the COVID ICU between 1st January and 15th February, 2021. Of the 60 patients admitted during the study period, 25 patients met the inclusion criteria. Demographic details (age, sex), past medical history, investigations (random blood Sugar), medical management, ventilatory requirements, patient progress, and survival were obtained from medical records and a computerized patient record system. The pre-breakfast and pre-dinner values were evaluated for 3 successive days. Other parameters such as the severity of COVID-19, septic shock, multiorgan failure, and the need for mechanical ventilation were recorded. Sub-group analysis among survivors and non-survivors was also performed.
Various parameters were either continuous or categorical. Continuous variables are described as mean ± standard deviation or median with an interquartile range, while categorical variables are presented as frequencies and percentages. The independent sample t-test, Mann-Whitney U test, and Durbin-Conover test were used to analyze the random blood sugar values for 3 consecutive days.
Out of the 60 patients screened for possible inclusion in the study, 25 patients with a known case of diabetes mellitus with laboratory-confirmed COVID-19 were included in the final analysis. Patients were further divided into survivor (S) and non-survivor (NS) groups for the analysis. The patient demographics, comorbidities, COVID-19 severity, median blood sugar level, treatment, and outcomes are summarized in Table 1.
Table1: Demographic and clinical characteristics of COVID-19 patients with diabetes. View Table 1
The overall median age of the patients was 61 years (41-85), with a higher median age in non-survivors (62 years) than in survivors (60 years). Approximately 17 (68%) were male and 8 (32%) were female. Hypertension was the most common co-morbidity associated with diabetes patients, accounting for 60% of the cohort. 36% of patients reported kidney dysfunction, of which 88% died. 56% and 52% of patients reported the development of acute respiratory distress syndrome and shock, respectively. As far as COVID severity is concerned, 8% of patients had mild, 40% had moderate and 52% had severe COVID-19.
Clinical management showed that 84% of patients received insulin, while only 16% were administered oral hypoglycemic agents for hyperglycemia management. Steroids were used in 72% of the patients. Mechanical ventilation was required in 64% of patients. The median ICU stay was 8 (2-72) days, with 8 (6-14) days in survivors and 9 (4.5-11.5) days in non-survivor. The overall median hospital stay was 13 (6-79) days, with 14 (10-19) days in survivors and 12 (9.75-14.5) days in non-survivor. The overall mortality in patients with diabetes with COVID-19 was 52%.
The median blood sugar levels on days 1, day 2, and day 3 are mentioned in Table 1. It shows considerable variation over 3 successive days. The value was consistently high in non-survivor although the result was not statistically significant.
Pair-wise blood sugar comparison showed a statically significant variation between day 1 and day 3 (Table 2 and Figure 1) Patients who have received steroids during treatment have consistently high-median sugar levels, although the result was not statistically significant (Table 3).
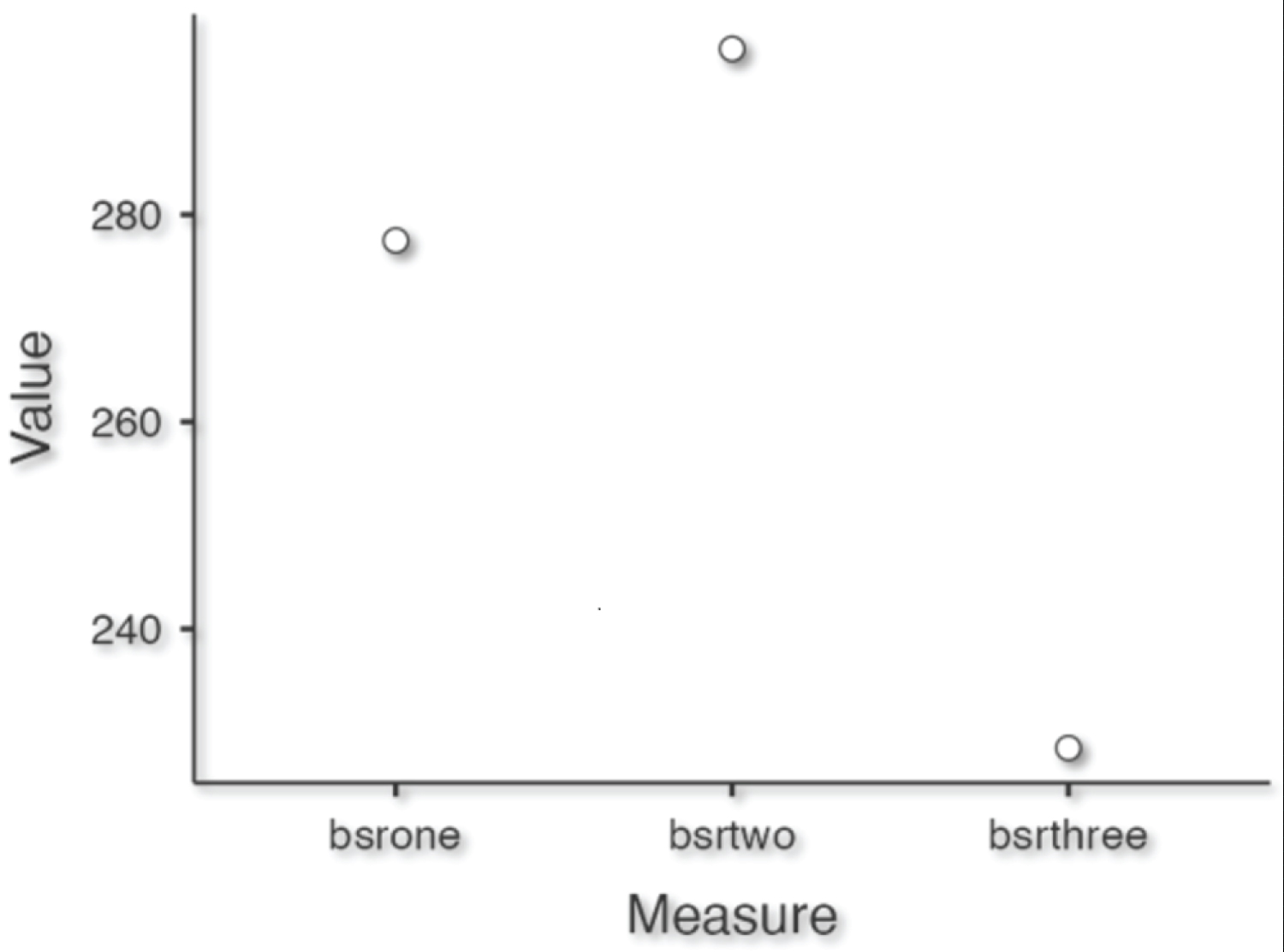 Figure 1: Descriptive plot showing pair-wise median blood sugar level.
View Figure 1
Figure 1: Descriptive plot showing pair-wise median blood sugar level.
View Figure 1
Table 2: Pair-wise comparison of median blood sugar level of first 3 consecutive days. View Table 2
Table 3: Day-wise comparison of median blood sugar levels of the first 3 consecutive days among patients given steroid vs. non-steroid. View Table 3
Our retrospective analysis studied the relationship between hyperglycemia and its outcome in patients with COVID-19. Our study demonstrated that the non-survivor group was associated with high median age (62 years), high blood glucose level (> 282 mg/dl), increase presence of shock, and high number of mechanical ventilated patients (p value- 0.01), which resulted in poor clinical outcome with increased in the mortality (48%). Thus, indirectly hyperglycemia was associated with more shock, higher incidence of mechanical ventilation and mortality, but it has no effect on COVID severity, comorbidity, ICU stay and hospital stay.
Diabetes has been incriminated as a risk factor for poor prognosis and mortality in patients with COVID-19. Sand AR, et al. in a multicenter retrospective study in COVID-19 patients demonstrated that hyperglycemia had a significantly higher mortality rate (31.45 vs. 16.6%, p, 0.001), higher ICU length of stay (5.5 vs. 3.5, p < 0.001) and increased use of mechanical ventilation (50.0% vs. 37.2%, p = 0.004) than patients with normoglycemia [1]. Similarly, in another study by Bode, et al., they demonstrated that Covid-19 patients with diabetes or uncontrolled hyperglycemia had a longer length of stay (5.7 vs. 4.3 days, P < 0.001) as compared to patients without diabetes or hyperglycemia [11]. Shang J, et al. in a retrospective cohort study in COVID-19 patients with diabetes from Wuhan reported shorter survival time, high incidence of complications and thus indicating diabetes as an independent risk factor for COVID-19 prognosis (hazard ratio 2.180, P = 0.031) [12].
Further, Zhu L, et al. in their retrospective analysis of 7337 patients with COVID-19 showed that 12.9% of patients had preexisting diabetes and they had increased mortality (7.8% vs. 2.7%, adjusted hazard ratio: 1.49) and intervention rates as compared to patients without diabetes [6]. Kumar A, et al. in their meta-analysis of 16003 COVID-19 patients have also shown that diabetes was associated with 2 times increased risk of mortality and severity compared with patients without diabetes [13]. Kumar B, et al. also reported three times higher mortality rate in preexisting diabetic patients as compared to the those without diabetes [14].
Various studies have shown that higher blood glucose levels on admission were associated with higher mortality, predictive of moderate to severe disease and were strongly correlated with the markers of inflammation. Kumar B, et al. in their study reported patients with plasma glucose of 180 mg/dl or less had better survival [14]. Similarly, Fadini GP, et al. also showed that admission higher fasting plasma glucose was associated with COVID-19 severity, increase in relative risk of 21% (RR 1.21; 95% C.I. 1.11-1.32; P < 0.001) for each 36 mg/dl increase in fasting blood glucose level [15]. Likewise, in our study the overall median blood sugar level for three consecutive days were above 200 mg/dl with high median blood glucose level in the non-survivor than the survivor group, indicating high mortality with high blood sugar values.
The mechanism for increased mortality can be hyperglycemia-induced changes in the immune response and enhanced release of inflammatory cytokines. Various studies have shown that diabetes affects the host's immune response to infection. It affects the different components of immune response like regulation of the production of different cytokines and function of different immune cells [16]. Serum concentrations of both pro-inflammatory and anti-inflammatory cytokines like IL-6, tumor necrosis factor-α, and IL-10, were raised in a significant number of patients with severe disease compared with moderate disease, indicating that cytokine storms might be associated with disease severity [17].
Initial results from the RECOVERY trial showed that the use of dexamethasone was associated with reduced mortality in COVID-19 patients requiring oxygen support or mechanical ventilation [18]. But steroid-induced hyperglycemia is a potentially serious side effect that may result in poor outcomes, and it should be addressed while managing COVID-19 patients [19]. In our study, patients who had received steroids had high-median blood sugar levels compared with the non-steroid group.
This brief report has several limitations. Firstly, the sample size of our study was very small, so to derive any conclusion is not right. Secondly, we could not assess the BMI of the patients, as high BMI is associated with an increased risk of diabetes and poor hyperglycemia control. Thirdly, we could not obtain the glycosylated hemoglobin value, which depicts the past blood sugar control of the patients. Further, the high-glycosylated hemoglobin value will indicate poor sugar control and thus affecting the outcome. Thirdly, this study was retrospective and observational type involving a small sample size with no control group.
Hyperglycemia in critically ill COVID-19 patients with preexisting diabetes shows worst outcome in terms of complications, need for mechanical ventilation, and mortality. However, our study sample size is very small to arrive at any conclusion. Therefore, a well-designed prospective study is needed to determine the effect of hyperglycemia on outcomes in patients with diabetes and COVID-19 and also to know the optimal target for glucose control.