Burkholderia cepacia complex (BCC) consists of more than 20 distinct gram-negative bacterial species. While commonly associated with cystic fibrosis (CF), BCC infections are not frequently reported in individuals with diabetes mellitus (DM). In this case report a 70-year-old female with multiple comorbidities, including Type 2 Diabetes Mellitus (DM), Chronic Kidney Disease (CKD), and Hypertension (HTN), who presented with a Burkholderia cepacia skin abscess at an insulin injection site on her anterior abdominal wall. The patient's clinical presentation, diagnostic workup, and treatment course are discussed.
Burkholderia cepacia complex (BCC), Skin abscess, Diabetes Mellitus (DM)
The Burkholderia cepacia complex (BCC) encompasses a cluster of widely distributed, aerobic, gram-negative bacilli. This group comprises at least 20 closely related bacterial species, which can be identified through the analysis of recA gene sequences [1]. Burkholderia cenocepacia stands out as the most virulent species within the Burkholderia genus, being linked to higher mortality rates than any other Burkholderia species . Notably, it is a major contributor to recurrent respiratory infections in individuals afflicted with cystic fibrosis (CF) and is also associated with various healthcare-related illnesses [1]. The different species within the Burkholderia cepacia complex (BCC) are not typically the primary pathogens responsible for causing skin and soft tissue infections (SSTIs) [2], especially in diabetic patients who often present with polymicrobial flora-related infections. This case is being reported here due to the rarity of Burkholderia cepacia complex (BCC) infections in patients without cystic fibrosis (CF).
A 70-year-old female with a 10-year history of Type 2 DM, CKD, and HTN presented with pus discharge from an insulin injection site on her anterior abdominal wall and a low-grade fever persisting for 5 days. She also reported symptoms of burning and pinprick sensations in her legs, leg edema, and morning periorbital puffiness. On examination, acanthosis nigricans, skin tags, and an abscess at the insulin injection site were noted. Laboratory findings revealed Hb of 11.6 g/dl, TLC of 7330/µL, Neutrophil count of 53%, and lymphocyte count of 39%. Liver function tests (LFT) showed a bilirubin level of 0.3 mg/dl, AST of 34.0 U/L, ALT of 29.0 U/L, total protein of 7.1 mg/dl, and albumin of 3.7 mg/dl. Kidney function tests (KFT) indicated a serum creatinine level of 1.6 mg/dl and urea level of 52 mg/dl. Arterial blood gas analysis (VBG) revealed a pH of 7.29, bicarbonate level of 19.3 mmol/l, lactate level of 3.4 mmol/l, and pCO 2 of 42. Abdominal wall ultrasound showed subcutaneous stranding over the pus area on the anterior abdominal wall. A culture report confirmed Burkholderia cepacia , which was sensitive to Piperacillin, Ciprofloxacin, and Cefoperazone but resistant to ampicillin + sulbactam and ceftazidime + clavulanic acid (Figure 1A, Figure 1B and Figure 1C).
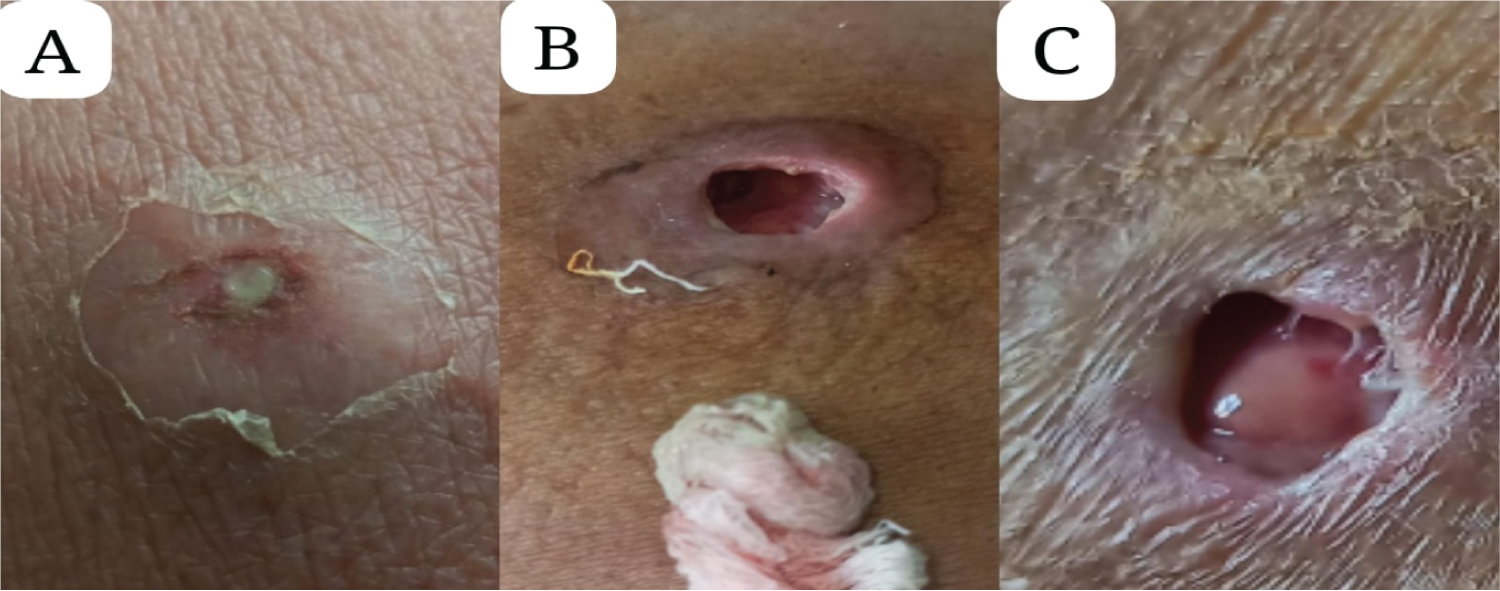 Figure 1: (A) Insulin site abscess; (B) Abscess cavity with drained pus; (C) Healthy granulation tissue indicating good healing.
View Figure 1
Figure 1: (A) Insulin site abscess; (B) Abscess cavity with drained pus; (C) Healthy granulation tissue indicating good healing.
View Figure 1
The patient was treated with Piperacillin-Tazobactam at a dose adjusted for her renal function and received daily antiseptic dressing for the abscess. Her diabetes was managed with insulin, with doses adjusted based on self-monitoring of blood glucose (SMBG). After two weeks of antibiotic therapy, the abscess resolved, and the patient was discharged in a stable condition.
Burkholderia cepacia complex (BCC) infections can vary in severity, ranging from relatively mild infections to potentially life-threatening sepsis, particularly in patients with conditions like cystic fibrosis (CF) or chronic granulomatous disease. However, it's worth noting that some earlier studies have suggested that BCC is not a prevalent pathogen in diabetic patients with skin abscess [3]. This case highlights the importance of considering rare pathogens like Burkholderia cepacia in diabetic patients with skin abscesses.
In conclusion in this case, the management of a Burkholderia cepacia skin abscess in a 70-year-old female with Type 2 DM, CKD, and HTN was successful through a multidisciplinary approach. Early diagnosis and appropriate treatment resulted in the resolution of the abscess and a favorable outcome for the patient.