Background: Gestational diabetes is one of the most common complications in pregnancy and its prevalence has increased progressively and in parallel with other conditions worldwide.
Objectives: To describe and compare the clinical characteristics and maternal and neonatal outcomes of pregnant women diagnosed with gestational diabetes, considering the trimester of diagnosis.
Methods: Data were collected on pregnant women with singleton pregnancies whose birth occurred at our center between January 2021 and May 2023. The sample was divided into two groups, according to the trimester of diagnosis of gestational diabetes, which were compared with respect to several variables.
Results: A total of 315 pregnant women were included in the study. 54.9% of pregnant women were multiparous; 17.5% had a history of gestational diabetes in previous pregnancies. We found statistically significant differences between the two groups regarding body mass index prior to pregnancy, glycated hemoglobin levels at diagnosis and the occurrence of newborns who were small for gestational age versus large for gestational age.
Conclusion: Understanding the pathophysiology and risk factors associated with gestational diabetes is of relevance given the association with short- and long-term complications, both maternal and offspring.
Gestational diabetes, Pregnancy, Trimester of diagnosis, Fetal and maternal outcomes
BMI: Body Mass Index; DM: Diabetes Mellitus; GA: Gestational Age; GD: Gestational Diabetes; HbA1c: Glycated Hemoglobin; LGA: Large for Gestational Age; NFHRP: Non-Reassuring Fetal Heart Rate Pattern; NICU: Neonatal Intensive Care Unit; PLH: Placental Lactogenic Hormone; SD: Standard Deviation; SGA: Small for Gestational Age
From very early stages of pregnancy, metabolic adaptations occur in the maternal organism, which aim to provide an environment suitable for the normal course of embryogenesis, fetal growth, and maturation [1-3]. Thus, pregnancy is typically characterized by an insulinogenic state, in which a considerable release of insulin is observed when faced with an oral glucose overload.
At an early stage of pregnancy, there is a decrease in maternal fasting glycemia resulting from both greater insulin production and its greater peripheral use. On the other hand, postprandial glycemia levels increase due to increased peripheral insulin resistance, a phenomenon mediated by placental lactogenic hormone (PLH) and, to a lesser extent, by prolactin and cortisol (a phenomenon that manifests itself mainly from the second trimester on [1,2].
The decrease in glucose tolerance that is observed in some pregnant women results not only from the increase in peripheral insulin resistance, but also from the inability of these women's pancreas to adequately respond to the increasing needs for insulin production. It is this inability to adapt that is anomalous during pregnancy and that characterizes gestational diabetes (GD) [1].
GD is one of the most common complications of pregnancy and its prevalence has progressively increased, with an estimated worldwide prevalence of hyperglycemia in diabetes of 16%, 84% of which is GD [4-7]. According to the latest National Diabetes Observatory, the prevalence of this pathology in Portugal in 2018 was 8.8% [4]. This prevalence has increased in parallel with other conditions, such as type 2 Diabetes Mellitus (DM), obesity and decreased oral glucose tolerance [7-9].
Traditionally, GD is defined as a glucose tolerance abnormality diagnosed for the first time during pregnancy [10,11]. Among its main complications are the increased risk of pre-eclampsia, large for gestational age (LGA) newborns and cesarean section births [12,13].
To describe and compare the clinical characteristics and maternal and neonatal outcomes of pregnant women diagnosed with GD, considering the trimester of diagnosis.
This is a retrospective, observational and descriptive study of the clinical characteristics and maternal and neonatal outcomes of pregnant women diagnosed with GD, according to the trimester of diagnosis. Two groups were considered: Group 1, which included pregnant women diagnosed with GD during the 1 st trimester and group 2 with pregnant women whose diagnosis occurred in the 2 nd trimester of pregnancy.
To this end, data was collected on pregnant women with singleton pregnancies whose birth took place in our center between January 2021 and May 2023.
Data were obtained regarding demographics, parity, trimester of GD diagnosis (including the week of pregnancy in which it was made), need for pharmacological therapy and the gestational age (GA) in which the onset occurred, level of glycated hemoglobin (HbA1c) at diagnosis, type of delivery and GA, as well as maternal and neonate complications.
Cases of diabetes during pregnancy, as well as multiple pregnancies, were excluded from our analysis.
Data were obtained by consulting the users' electronic clinical files and the statistical analysis was carried out using SPSS ® – version 27 for Windows.
A descriptive analysis was carried out, with measures of central tendency and measures of dispersion, considering the variables under study.
In the comparison between the two groups evaluated, T test for independent samples and Kruskal-Wallis test were used. To verify the association between the variables, chi-square test and point-biserial correlation coefficient were used. A significance level of p < 0.05 was considered.
A total of 315 pregnant women were included in the study: 183 (58.1%) belonged to group 1 and 132 (41.9%) to group 2. The prevalence of GD in pregnant women delivering at our center was 148 (14%) in 2021, 139 (12.14%) in 2022 and 28 (6.42%) between January and May 2023. Figure 1 shows the number of GD diagnoses according to the year evaluated, depending on the trimester of diagnosis.
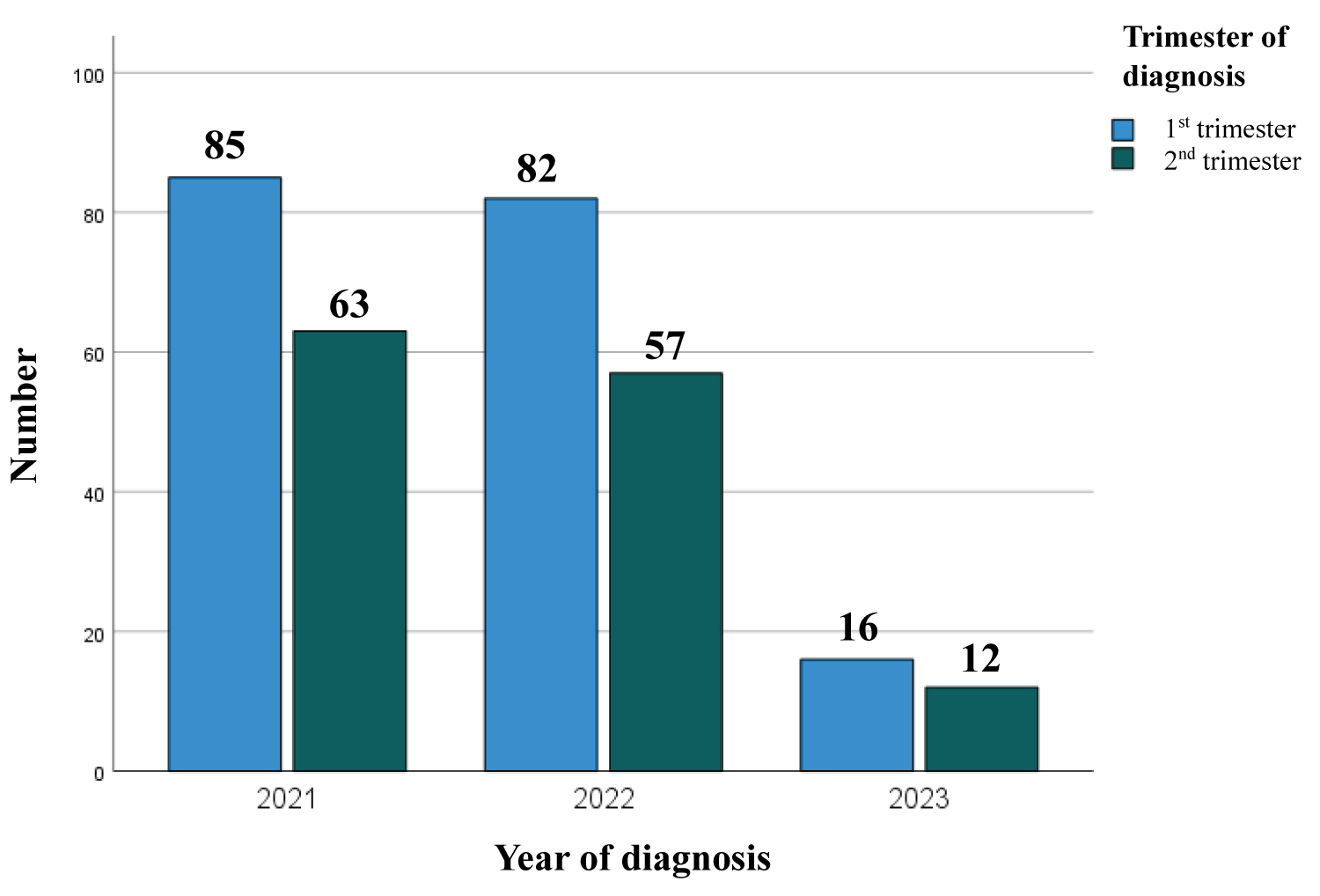 Figure 1: Number of GD diagnoses according to the year of the study evaluated, considering the trimester of diagnosis.
View Figure 1
Figure 1: Number of GD diagnoses according to the year of the study evaluated, considering the trimester of diagnosis.
View Figure 1
Average age of all pregnant women included in the sample was 33.25 years (SD = 5.5), varying between 19 and 47 years, with no statistically significant differences between the two groups evaluated ( p = 0.674) – Table 1.
Table 1: Differences between pregnant women diagnosed with GD in the 1st versus 2nd trimester. View Table 1
54.9% of pregnant women were multiparous and only 17.5% had a history of GD in previous pregnancies. Majority of pregnant women included in the sample (69.8%) had a family history of DM.
In group 1, the mean GA at diagnosis was 8 weeks and 4 days (SD = 3.1), while in group 2 it was 25 weeks and 1 day (SD = 1.21).
When comparing pregnant women < 35-years-old versus ≥ 35-years-old, there were also no differences between the groups regarding the average GA at diagnosis [ t (313) = 0.14, p = 0.89].
Regarding the average body mass index (BMI) prior to pregnancy, most pregnant women included in group 1 had a BMI ≥ 30 kg/m 2 (40.5%). On the other hand, pregnant women diagnosed with GD in the 2 nd trimester were generally normal weight (34.1%) – Table 2.
Table 2: Distribution of BMI prior to pregnancy, by category, according to the respective group. View Table 2
Therefore, we found statistically significant differences between the two groups when evaluating this variable, confirming that pregnant women in group 1 had, on average, a higher BMI than group 2: 29.65 Kg/m 2 versus 27.93 Kg/m 2 ( p = 0.026) – Table 1.
Furthermore, we confirmed the existence of a statistically significant association between maternal obesity and the birth of LGA newborns [χ 2 (2) = 10.86, p = 0.004].
Weight gain during pregnancy was identical for both groups: on average, each pregnant woman gained around 10 Kg (Table 1).
By analyzing Figure 2, it is possible to verify that for all BMI classes, weight gain was very similar in both groups evaluated. The exception was the below-normal weight class, in which there was a much greater increase in weight in pregnant women diagnosed with GD in the 1 st trimester compared to those diagnosed in the 2 nd trimester.
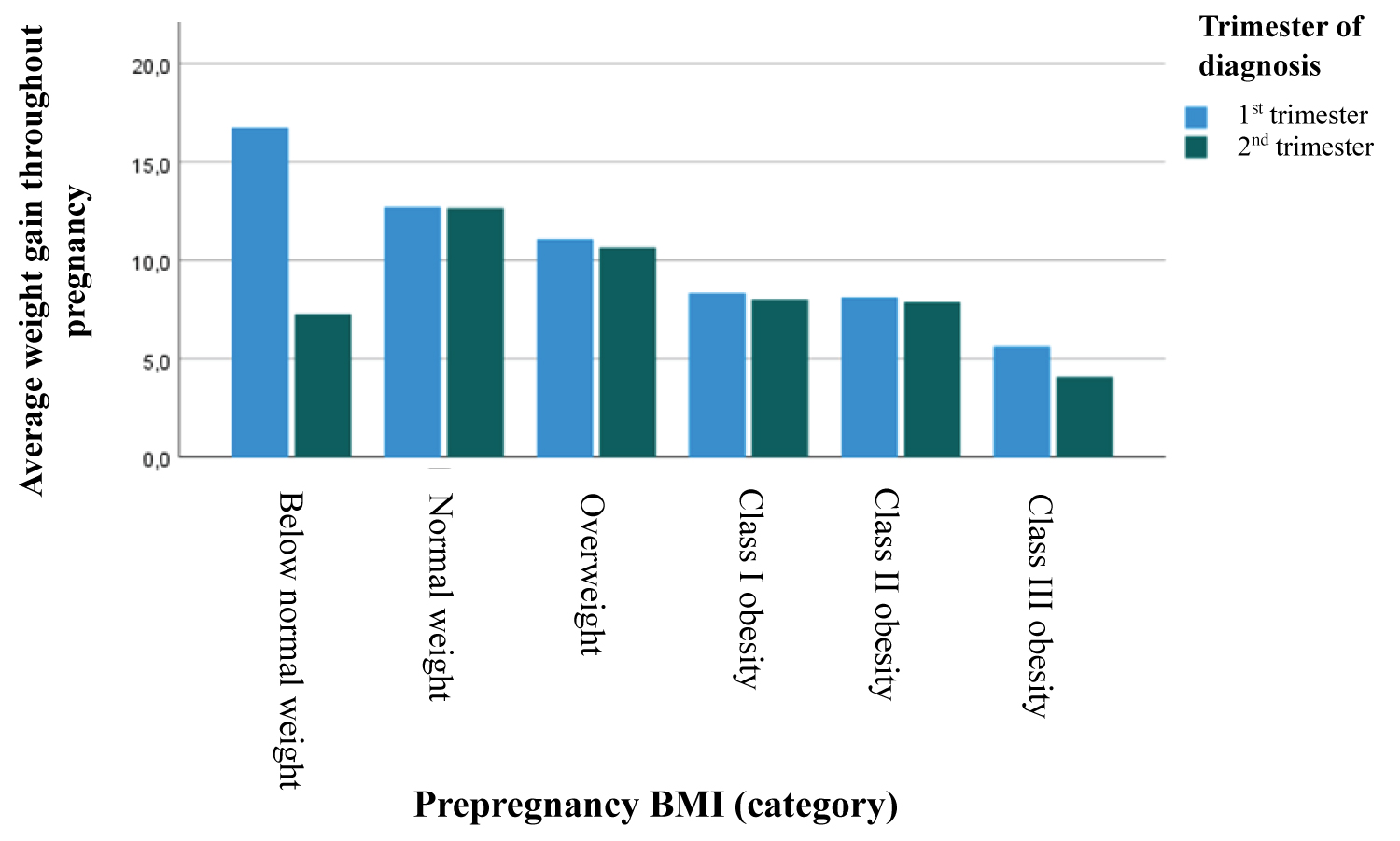 Figure 2: Average weight gain during pregnancy by BMI class, according to the respective trimester of GD diagnosis.
Figure 2: Average weight gain during pregnancy by BMI class, according to the respective trimester of GD diagnosis.
BMI: Body Mass Index.
View Figure 2
In both groups, most GD cases diagnosed did not require the introduction of medical therapy (54.6% in group 1 and 62.9% in group 2). Among medicated cases, a combination of oral antidiabetic therapy and insulin was necessary in most cases – Figure 3 and Table 3. Within these, the average GA at the introduction of therapy was 22 weeks (group 1) and 32 weeks and 3 days (group 2), with statistically significant differences between the groups ( p < 0.001) – Table 1.
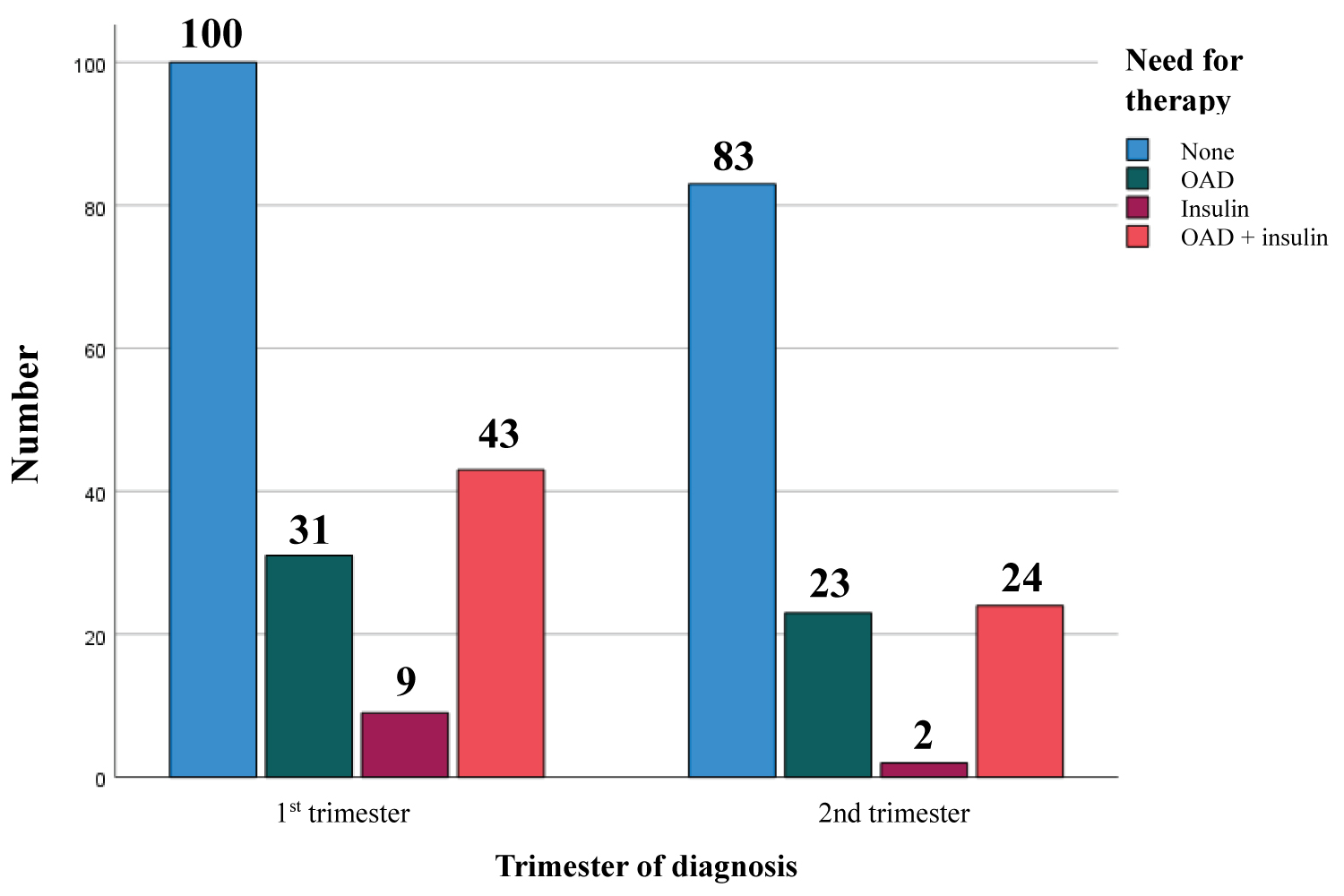 Figure 3: Need for therapy in the treatment of GD, according to the respective trimester of diagnosis.
View Figure 3
Figure 3: Need for therapy in the treatment of GD, according to the respective trimester of diagnosis.
View Figure 3
Table 3: Need for therapy in the treatment of GD, according to the respective group. View Table 3
There was a statistically significant association between the presence of maternal obesity and the need for medical therapy to control GD [χ 2 (2) = 34.45, p < 0.001]. Likewise, we confirmed the existence of a statistically significant association between maternal age and the need for therapy to control GD (r bp = 0.133, p = 0.018).
Pregnant women diagnosed with GD during the 2 nd trimester had, on average, a significantly higher HbA1c at diagnosis than those diagnosed in the 1 st trimester: 5.31% versus 5.2% (Table 1).
The average GA of births was 39 weeks, with most births occurring by cesarean section in both groups, in relation to the current high rate of cesarean sections at our center. The most frequent reason for cesarean section was intrapartum non-reassuring fetal heart rate pattern (NFHRP) – Table 4.
Table 4: Type of birth, according to the respective group. View Table 4
When comparing the two groups regarding the weight of their newborns at birth, we found statistically significant differences (χ 2 = 7.72, p = 0.005), with pregnant women in group 2 tending to have more small for gestational age (SGA) neonates and those in group 1 with more LGA newborns (Table 5).
Table 5: Maternal and perinatal results, according to the respective group. View Table 5
We verified the existence of a statistically significant association between the need for medical therapy to control GD and the occurrence of LGA newborns [χ 2 (1) = 12.97, p < 0.001], thus confirming the acceleration of fetal growth as a potential sign of suboptimal glycemic control, with greater need for medical therapy.
Regarding maternal complications, in both groups, those that occurred most frequently were hypertensive complications, whether gestational hypertension or pre-eclampsia, and preterm birth - Table 5.
Concerning complications related to neonates, similarly, in both groups, the most frequent was hyperbilirubinemia, requiring phototherapy. Furthermore, we confirmed the occurrence of 8 cases of admission to the Neonatal Intensive Care Unit (NICU) in group 1 compared to 5 cases in group 2, both mostly due to situations of prematurity and transient tachypnea of the newborn requiring oxygen therapy alone or associated with other pathologies.
It is worth mentioning the occurrence of a case of fetal death in uterus in a pregnant woman diagnosed with GD during the 1 st trimester, with very poor glycemic control due to frequent therapeutic failures by the pregnant woman.
In most cases, there was no persistence of diabetes in the oral glucose tolerance test carried out postpartum (67.2% in group 1 and 66.7% in group 2). Among women with an altered test, the most common change was a decrease in glucose tolerance (3.83% in group 1 and 4.55% in group 2), with only 2 cases recorded with a diagnosis of DM in this test in group 1.
The increased prevalence of GD has been, at least in part, explained by increasing maternal age and obesity [9-11]. In our sample, most pregnant women were overweight or obese in both groups evaluated (73.8% in group 1; 63.6% in group 2) – Table 2. However, despite this gradual trend of increasing maternal age, in this study most pregnant women analyzed were < 35-years-old (57.8%).
Other important risk factors in the pathophysiology of this condition are a family history of DM, especially in first-degree relatives, and excessive weight gain during pregnancy. In our sample, most pregnant women had a positive family history. Regarding weight gain during pregnancy, when considering the BMI classes with a higher risk of GD (overweight and obesity), the average weight gain was within the limits established by the Institute of Medicine : 6-11 Kg and 5-9 Kg, respectively (Figure 2).
The neonatal morbidity observed in our sample follows what has been described in the literature, in which respiratory and metabolic complications (hyperbilirubinemia, hypoglycemia, hypocalcemia, polycythemia, among others) are among the most frequent [14,15].
Furthermore, we found an increased risk of LGA newborns in obese pregnant women, confirming maternal obesity as one of the major contributing factors to this outcome.
In line with previous data, decreased oral glucose tolerance has become the most prevalent change in the postpartum reclassification test [4].
Thus, in our sample, pregnant women diagnosed with GD in the 1 st trimester tended to have a higher BMI and a greater probability of having a LGA neonate. On the other hand, pregnant women diagnosed during the 2 nd trimester had, on average, higher HbA1c values and a greater tendency to have a SGA newborn. The maternal complications observed, namely hypertensive disease and preterm birth, do not seem to differ depending on the trimester of GD diagnosis [16-19].
Greater limitations of this study are related to its retrospective nature.
Understanding the pathophysiology, risk factors and implications associated with GD becomes of particular relevance given that not only is it associated with short-term complications (such as hypertensive pathology of pregnancy, need for preterm birth due to poor metabolic control or fetal pathology, shoulder dystocia, among others), but also has long-term implications, both for the mother (type 2 DM, metabolic syndrome, cardiovascular risk) and for the offspring (oral glucose tolerance anomaly, obesity, hypertension and metabolic syndrome).
Furthermore, achieving adequate glycemic control is especially important in reducing the frequency and severity of these potential complications. It should be added that nutritional advice and physical exercise are primary tools for achieving adequate control.
The postpartum period is also of particular importance as it is a time when adaptations to a healthy lifestyle previously adopted during pregnancy must be maintained in order to reduce the risk of developing non-communicable diseases.
The authors declare that they have no conflict of interest regarding the publication of this study.