Background: Diabetes mellitus is a rapidly increasing chronic disease associated with complications resulting in long-term damage and failure of various organ systems. In Ethiopia, there is a dearth of evidence on the prevalence of Diabetic complications.
Objective: To assess the prevalence of diabetic complications and associated factors among diabetic patients on follow-up at the diabetic center of Tikur Anbessa Specialized Hospital.
Methods: This was an institutional-based cross-sectional study design conducted from April 14-May 24, 2020. Data were collected by face-to-face interview and medical record review using a pre-tested data collection tool. The collected data was entered into SPSS version 25 and descriptive statistics were performed. The multiple logistic regression model was used to identify the predictors for diabetic complications. A P-value less than 0.05 was considered significant.
Result: A total of 361 participants were included. The majority of the participants were females 186 (51.5%), in the age group of 30-60 years 225 (62.5%), have type 2 diabetes 303 (83.9%), and knew their diabetes and started treatment for 6-10 years 157 (43.5%) and 161 (44.6%) respectively. Most participants had poor glycemic control 279 (77.3%) with HbA1c level ≥ 7. A total of 120 (33.2%) had experienced diabetic complications where neuropathy was the predominant one 57 (47.5%). The odds of developing diabetic complications was more than twice higher in males [AOR 2.6, 95% CI 1.59,4.25; P ≤ 0.01] and patients with A1C ≥ 7% [AOR 2.34, CI 1.4, 6.3; P ≤ 0.01].
Conclusion: The diabetic complications were high among the diabetic patients in TASH. The majority of patients had poor glycemic control. Chronic microvascular complications particularly neuropathy was the most common. The significant factors predicting the occurrence of complications were male gender and HbA1c ≥ 7%.
Diabetes mellitus, Diabetic control, Diabetic complications, Chronic complication, Microvascular complication
BMI: Body Mass Index; CI: Confidence Interval; DM: Diabetes Mellitus; FBS: Fasting Blood Sugar; HbA1c: Glycated Hemoglobin; IDF: International Diabetic Federation; TASH: Tihkur Anbessa Specialized Hospital
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by hyperglycemia and disturbed metabolism of glucose, fat, and protein. It has emerged as a leading global health problem as the prevalence of DM is rapidly increasing at epidemic levels throughout the world [1-3]. In particular, the economy and health care of low- and middle-income countries are being threatened by the rapid progression of DM. In 2019, about 9.3% of the world population were living with diabetes and this prevalence is expected to increase to 10.2% by 2030 and 10.7% by 2045. Besides, DM is the fourth leading cause of death resulting in an estimated 4.2 million deaths globally [4,5].
In Ethiopia, DM is rapidly increasing chronic diseases with a reported prevalence between 2.0-6.5%, the highest prevalence being in Addis Ababa, the capital city [6]. According to the International Diabetes Federation (IDF) report of 2019, the national prevalence of DM in Ethiopia was 3.2% among adults of 20-70 years-old. Besides, Ethiopia stands fourth with DM prevalence in Africa with an estimated 1.7 million people living with DM [5]. Also, a systematic review by Gebreyohannes, et al. reported that an estimated 2.6 million people were living with diabetes in Ethiopia [7].
Although preventable DM complications are major concerns for diabetic patients and the health care system as causes for long-term damage and failure of various organ systems. The major diabetic complications are hypertension, neuropathy, renal diseases, lower extremity amputations, retinopathy, visual disturbances, depression, and cataracts [6-8]. These complications account for increased morbidity, disability, and mortality, and threats for the economies of all countries especially in the middle and low economic countries [9,10]. These complications of DM can be classified as acute or chronic. Acute complications such as diabetic ketoacidosis, hyperglycemic hyperosmolar state, and hypoglycemia account for high morbidity and mortality among diabetic patients and contribute significantly to hospitalization and high costs of diabetes care [9]. Besides, chronic complications of DM are related to damage to small blood vessels (microvascular complications) or large blood vessels (macrovascular complications). Diabetic retinopathy is the most common microvascular complication, followed by diabetic nephropathy and neuropathy. All macrovascular complications arise from the development of atherosclerosis, which gradually causes the narrowing of arterial walls leading to coronary artery disease, stroke, and peripheral vascular disease [9].
The occurrence of DM complications is influenced by intrinsic and extrinsic factors. Different studies identified risk factors having predictive value for DM complications. The commonest risk factors for DM complications were age, body mass index, waist-to-hip ratio, blood pressure, fasting plasma glucose, glycated hemoglobin (HgA1c), lipid profiles, albuminuria, smoking and family history of diabetes, gender, type of DM, duration of illness, medication type, negative attitude towards DM, poor adherence to treatment and knowledge about DM and its management [11-16].
Despite the rapidly increasing burden of diabetes in Ethiopia, there is a dearth of evidence showing the prevalence, and associated factors related to DM complications. For the effective management of DM, it is crucial to generate evidence on diabetic complications and associated factors to enhance the therapeutic benefits and patient’s quality of life. Therefore, this study was aimed to assess DM complications and associated factors among diabetes patients on medical follow-up in TiKur Anbessa Specialized Hospital (TASH).
A cross-sectional study was conducted at TASH which is the largest teaching and Specialized public hospital in Ethiopia administered under Addis Ababa University, College of Health Sciences. This study was conducted from 14 April 2020 to 24 May 2020.
The source and the study populations constituted all diabetic patients who had follow-up treatment at the diabetic clinic of TASH and all diabetic patients who had follow-up treatment and fulfilled the inclusion criteria during the study period respectively.
The inclusion criteria for this study were the age of patients 18 and above, voluntary diabetic patients for the interview, and patients who start anti-diabetic drug treatment for at least six months. Pregnant women were excluded from the study.
The dependent variable of the study was the occurrence of diabetes complications whereas the independent variables were demographic factors (age, sex, BMI, educational qualification, monthly income, marital status, occupation, place of residence, social habits, physical activity, source of medication), diagnosis (type 1 and type 2), types of medications, duration of the disease and comorbidity.
The sample size was calculated using the single population proportion formula. The total sample size required for the study was 344 calculated based on the possible patient load to the clinic. By adding 10% contingency, a total of 361 patients were sampled. A systematic random sampling method was used to recruit samples for the study on each day of the data collection process.
After the filled-in forms were checked for completeness of data, cleaned before data entry, and then entered. Data entry and data analysis were carried out using Statistical Package for Social Sciences SPSS version 25. Descriptive statistics such as frequency, percentage, mean and standard deviation (SD) were employed to summarize patients’ characteristics and other related information. Univariable binary logistic regression analysis was performed to relate each variable to complications of diabetes. From the univariable analysis, those variables with p < 0.2 were selected for multivariable binary logistic regression analysis. Multivariable binary logistic regression analysis was used to assess the predictability of the independent variables of complication and to estimate, 95% confidence intervals (CI) and p-values. The association was declared significant at p < 0.05.
In this study, a total of 361 participants were included. The majority of the participants were females 186 (51.5%), in the age group of 30-60 years 225 (62.5%), and urban residents 334 (92.5%). Regarding the clinical characteristics, most participants were having type 2 diabetic patients 303 (83.9%), who knew their DM states and started treatment for 6-10 years 157 (43.5%) and 161 (44.6%) respectively. The glycemic control was not optimal for most participants 279 (77.3%) with HbA1c level ≥ 7 and 292 (80.9%) and a current FBS level of ≥ 126. Table 1 describes the details of socio-demographic and clinical characteristics.
Table 1: Socio-Demographic and clinical characteristics of Diabetic patients at TASH, Ethiopia, 2020. View Table 1
Among the study participants, a total of 120 (33.2%) had experienced diabetic complications. Most of the complications encountered were chronic complications 109 (90.8%) of which neuropathy was the predominant diabetic complication reported 57 (47.5%) followed by nephropathy 26 (21.7%). Figure 1 shows the types of diabetic complications encountered.
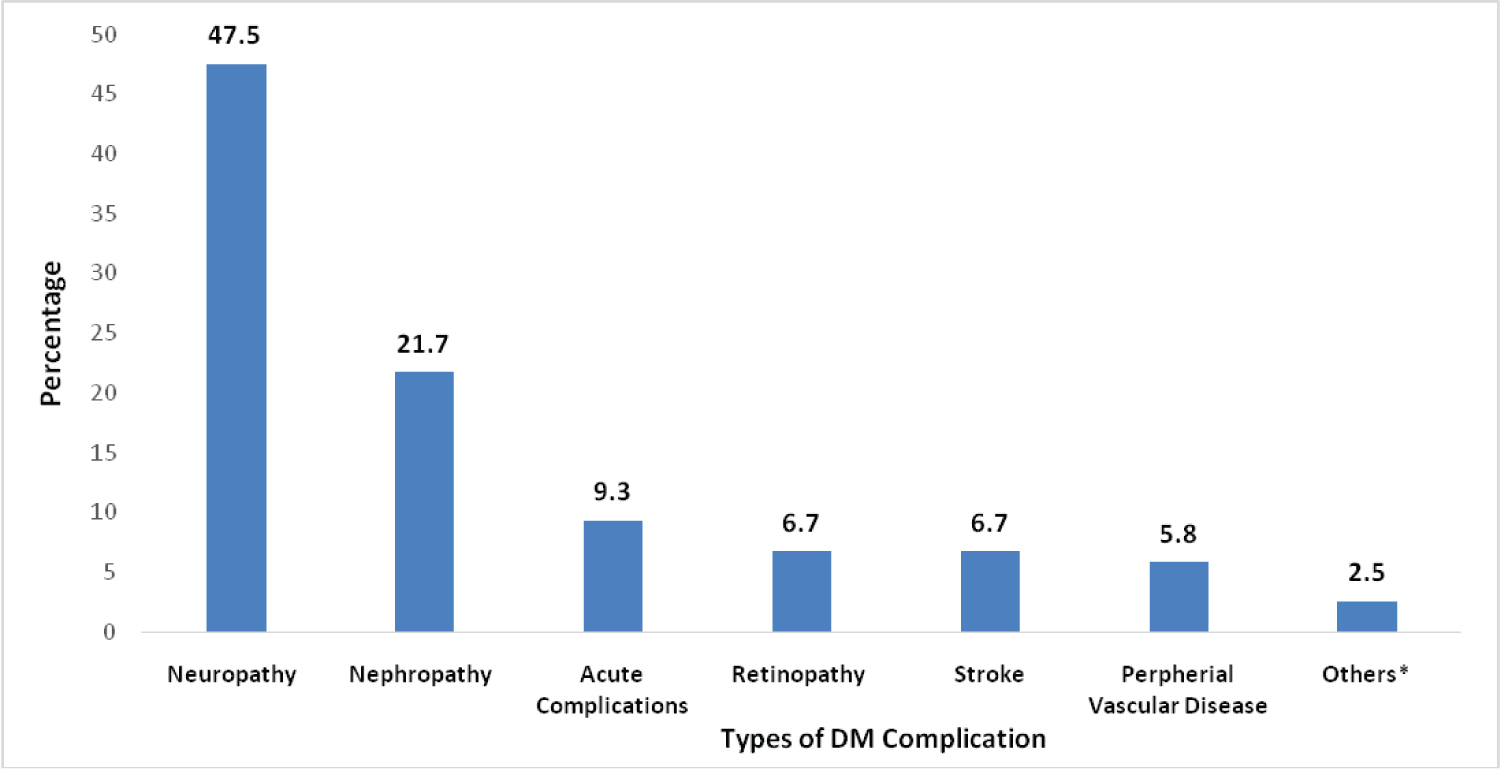 Figure 1: Types of diabetic complications among diabetic patients at TASH, Addis Ababa, Ethiopia (N = 120).
Figure 1: Types of diabetic complications among diabetic patients at TASH, Addis Ababa, Ethiopia (N = 120).
*diabetes foot ulcer, angina, myocardial infarction.
View Figure 1
The multivariate binary logistic regression analysis showed that gender and HbA1c had a statistically significant association with the occurrence of diabetic complications. The independent variables associated with the occurrence of diabetic complications were gender (P ≤ 0.01), age above 60 (P ≤ 0.01), type of DM (p = 0.03). As shown in Table 2, poor diabetic control and male gender were determinants for the occurrence of DM complications. The odds of developing diabetic complications were more than twice higher in participants with A1C ≥ 7% than those with HbA1C with lower than 7% [P ≤ 0.01, AOR 2.34, CI 1.4, 6.3] and male participants [P ≤ 0.01, AOR 2.6, CI 1.59, 4.25].
Table 2: Bivariate and multivariate logistic regression analysis of determinant factors associated with diabetic complications at TASH, Addis Ababa, Ethiopia. View Table 2
Diabetic complications are the major causes of morbidity and mortality, increased hospitalization, and increased health care expenditure for diabetic patients despite they are largely preventable and optimally treated. Hence, identifying the complications among diabetic patients is paramount to improving diabetes management. This study is, therefore aimed to assess the prevalence of diabetic complications and the predictor among diabetic patients attending follow-up at the diabetic clinic of TASH.
In this study, about half (50.4%) of the participants had comorbidities related to DM, hypertension being the most common comorbidity found in 37.7%. Our finding is similar to a study by Sheleme, et al. that reported 39.1% comorbid hypertension in Jimma Referral Teaching Hospital [17]. However, this finding is lower than 69.1% hypertension comorbidity by Negash, et al. in Addis Ababa [18]. The development of macrovascular complications and increased cardiovascular death is higher in patients with the coexistence of DM and hypertension.
Poor glycemic control is common among diabetic patients. In our study, the majority of our participants had poor diabetic control as indicated by higher FBG level above 126 mg/dl in 80.9% and A1C level ≥ 7% in 77.3% of study participants. This finding is in line with similar studies that reported poor glycemic control among diabetic patients in 72.1% in Jimma [17], 64.1% in Adama [19], 60.5% in Gondar [20], 64.1% in public hospitals of Western Ethiopia [21], 59.5% in West Ethiopia [22] and 55.3% of patients in Amhara region referral hospitals [23]. Poor glycemic control contributes to the higher prevalence of chronic diabetes complications [24]. Our findings also revealed poor glycemic control was a predictor of the occurrence of DM complications in our study participants.
This study revealed that 33.2% of diabetic patients had experienced at least one complication. This is comparable with findings that at least one complication was reported in 34.5% of type 2 diabetic patients in China [25], 31.3% in Northwest Ethiopia [20], and 38.5% of diabetic patients in Southwest Ethiopia [17]. In contrast, our finding is lower than a study by Agalu, et al. in Dessie, Ethiopia where 59.7% of patients reported at least one diabetic complication [26] and 53.5% major DM complications [27]. The variation in the prevalence of diabetes complications among studies might be differences in the participants' demographic characteristics, the type of diabetic complications assessed, and the difference in glycemic control.
Our study found that 90.8% of diabetic complications encountered were chronic complications of which neuropathy was the predominant 47.5% followed by nephropathy 21.7%. This finding was comparable with other similar studies in Ethiopia that reported microvascular complications as the most common chronic complications of DM [18,21]. In addition, our study finding is also similar to a study in Sri Lanka by Arambewela, et al. where neuropathy was 62.6%, and nephropathy 50.8% were the most common DM complications [28]. A high prevalence of chronic microvascular DM complications was also reported by a systematic review conducted in Northern Africa [24].
According to our study result, poor glycemic control (HbA1C ≥ 7%) and male gender were predictors for the occurrence of DM complications. The odds of developing diabetic complication were more than twice 2.6 times higher in males and 2.34 times higher in participants with A1C ≥ 7%. A study by Fasil, et al. found that poor glycemic control is a predictor of DM complication [20]. In contrast, a study by Gebre and Assefa found that the significant factors associated with diabetic complications were divorced marital status, poor glycemic control, body mass index > 25, and duration of illness [29]. Another study also reported that Age of the patient, family history of DM, duration of illness and medication therapy, and comorbidities were significantly associated [14].
As this study is based on a cross-sectional study design, it is impossible to assess the causality. Participants might express social desirability biases during the interview.
The diabetic complications were high among the patients on diabetic clinic follow-up in TASH. The majority of patients had poor glycemic control and hypertension as a comorbid disease. Most of the complications were chronic microvascular complications. The significant factors predicting the occurrence of complications were male gender and HbA1c ≥ 7%.
The authors acknowledge Addis Ababa University and the diabetic clinic of TASH for allowing the conduct of this study. We also acknowledge all the study participants for their voluntary participation.
CM and MG conceptualized the study and designed the methods, conducted the study, analyzed data and wrote the result. MG and MF supervised the study, transcribed and analyzed the data and prepared manuscript. MF reviewed the manuscript. All authors read and approved the final manuscript.
Ethical approval of the study protocols was granted from the Ethical Review Committee (ERC) of the School of Pharmacy, college of Health sciences, Addis Ababa University. Before data collection, informed verbal consent was obtained from the study participants. The confidentiality of study participants was assured by removing personal identifiers from the questionnaire and keeping the collected data in a secure place. Besides, this study was conducted following the Helsinki declaration.
Consent for publication is not applicable as our manuscript does not contain any personal data.
The authors have no conflicts of interest to declare.
Authors disclose no financial support for this study.
The data supporting the finding of this study will be made available upon request from the corresponding author.