This literature review investigated the subtle cavovarus foot with a search in Pubmed and Google Scholar using the following keywords: Subtle cavovarus foot, cavovarus foot or cavus foot and one or more of the following: Associations, injuries, ankle sprains, ankle instability, sports, plantar pressure, dynamic pedobarography, Tekscan and footprint, from January 1980 to February 2019.
Subtle cavovarus foot can alter foot and ankle biomechanics but reference values are lacking for dynamic pedobarography assessment. Subtle cavovarus foot is associated with peroneal tendinopathy, metatarsal stress fractures, and recurrent lateral ankle sprains, potentially leading to chronic ankle instability due to altered walking central control patterns. Treatment includes flexible/semi-rigid orthotics to laterally offload the foot, or surgery in rigid cases. Subtle cavovarus foot is associated with chronic foot and ankle pathologies. Unfortunately, diagnosis is often difficult or delayed. Early conservative management, with appropriate foot orthotics, favors a safer return to sports.
Strength of Recommendation Taxonomy (SORT): B
Level of evidence: Level IV clinical review
Subtle cavovarus foot, Chronic ankle instability, Foot and ankle pathologies, Injuries, Plantar pressure
The subtle cavovarus foot, originally known as the underpronator due to its naturally supinated position, is estimated to affect as much as 25% of the population [1-4]. It is a more common and mild, but often undiagnosed, form of the cavovarus foot deformity, which consists of a high medial plantar arch and varus of the hindfoot. These two conditions are the result of hindfoot inversion, forefoot supination, and a plantarflexed first ray; this causes altered foot mechanics during gait, instability, lateral foot pain, an increased risk of injury, and a longer recovery time [5]. Lateral soft-tissue structures of the ankle are stretched out, [4] putting the subject at risk for lateral ankle sprains caused by excessive plantarflexion, inversion, and internal rotation of the ankle [6]. As a result, there is an increased risk of developing chronic ankle instability, and patients will tend to report feeling their ankle "giving way" [2,7,8]. The aim of this report is to review the subtle cavovarus foot, including its clinical evaluation, radiological findings and plantar pressure measurements. Associations between subtle cavovarus foot and other pathologies, such as ankle sprains, chronic ankle instability, peroneal tendon pathologies, and stress fractures will be examined as well.
There are two main etiologies for cavovarus foot deformity: idiopathic and neurogenic. Half of the neurogenic cases are the result of the Charcot-Marie-Tooth disease [9,10]. However, when cavovarus is subtle, it is most commonly idiopathic [3,5,8].
From a biomechanical point of view, hyperactivity of the peroneus longus tendon induces plantarflexion of the first metatarsal, leading to a forefoot-driven cavovarus deformity and a flexible hindfoot with limited eversion. Over time, due to bone remodelling, the bones in the midfoot become more trapezoidal in shape, increasing plantarflexion of the first ray [4]. As a result, the hindfoot cannot evert and has decreased mobility [11]. The foot has increased rigidity [2,3], decreased energy dissipation, and is prone to stress injuries, especially at the fourth and fifth metatarsals [12]. Usually, the subtle deformity is forefoot-driven and even though it is mild, the pressure on the lateral part of the foot is increased, leading to chronic pathologies [2].
The diagnosis of subtle cavovarus foot relies on a physical examination [2]:
1. The peek-a-boo heel [4,13] sign is ascertained from an anterior view of the foot (Figure 1). With normal foot alignment, the heel pad cannot be viewed. This should be followed by a posterior view of the hindfoot for confirmation, although it will only be positive in more severe cavovarus deformities [3,8].
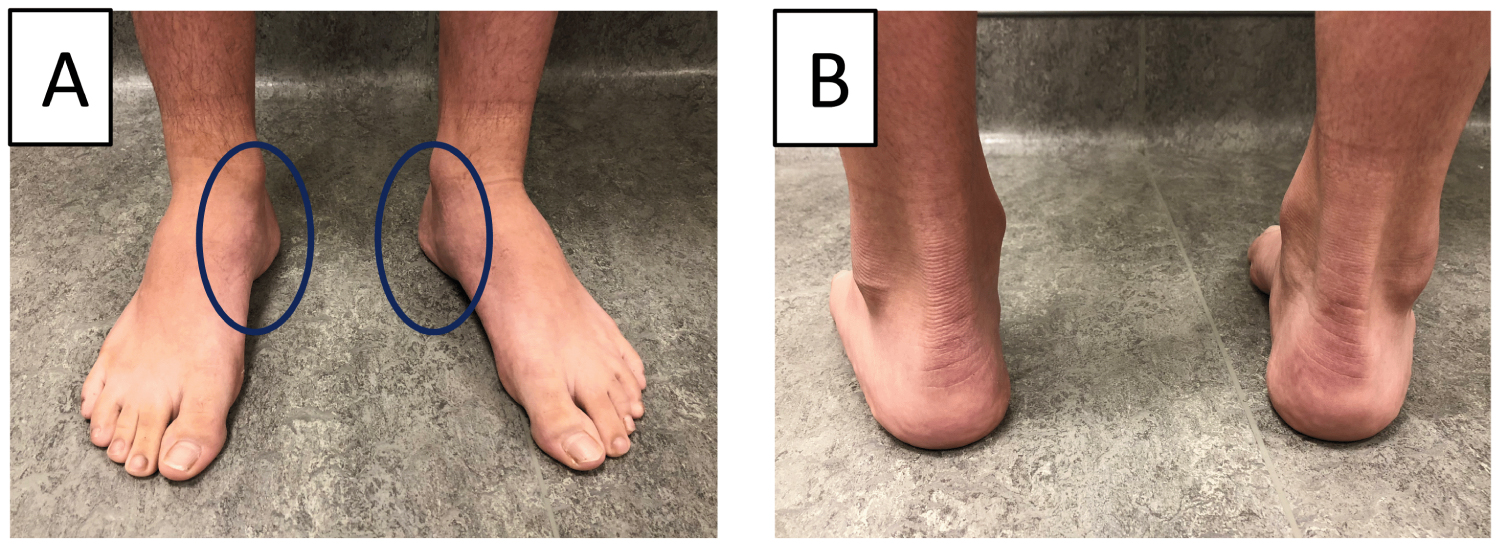 Figure 1: Subtle cavovarus identification on a patient with bilateral cavovarus feet. (A) Clinical evaluation from the front shows prominence of heel pads; (B) The back view reveals varus angulation.
View Figure 1
Figure 1: Subtle cavovarus identification on a patient with bilateral cavovarus feet. (A) Clinical evaluation from the front shows prominence of heel pads; (B) The back view reveals varus angulation.
View Figure 1
2. The Coleman block test [2,4,6,9] detects if the hindfoot varus is of primary origin or is secondarily caused by the plantarflexion of the first metatarsal [11,13]. The subject's heel and lateral border 'are'? supported by a 1-inch block to unload the first ray (Figure 2). If the hindfoot varus is corrected, the deformity is forefoot driven (caused by the first ray plantiflexion). This test also confirms the flexible nature of the deformity and the potential for a foot orthotic to effectively realign the foot [2,5].
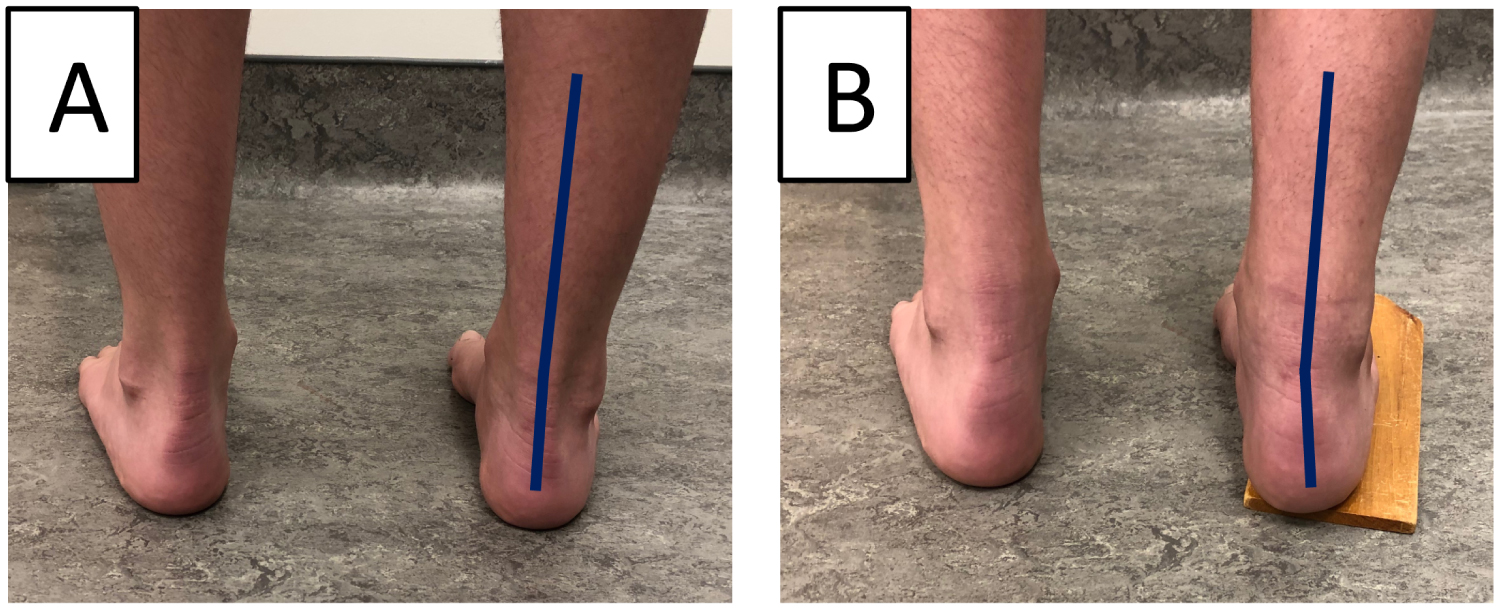 Figure 2: Coleman test. (A) Cavovarus foot without block; (B) Correction with block (positive Coleman test).
View Figure 2
Figure 2: Coleman test. (A) Cavovarus foot without block; (B) Correction with block (positive Coleman test).
View Figure 2
3. The Silfverskiold test [11,13] checks for equinus (limited dorsiflexion) of the ankle, or gastrocnemius tightness [2,3]. Normal dorsiflexion should be 10 and 20 degrees above neutral in passive and active knee flexion, respectively (Figure 3) [2]. If dorsiflexion is limited only when the knee is in extension, this indicates an isolated contracture of the gastrocnemius. However, if dorsiflexion is limited with the knee in flexion and in extension, this indicates a contracture of the Achilles tendon or of the posterior ankle and subtalar joint capsule, or else an anterior impingement of the ankle [2].
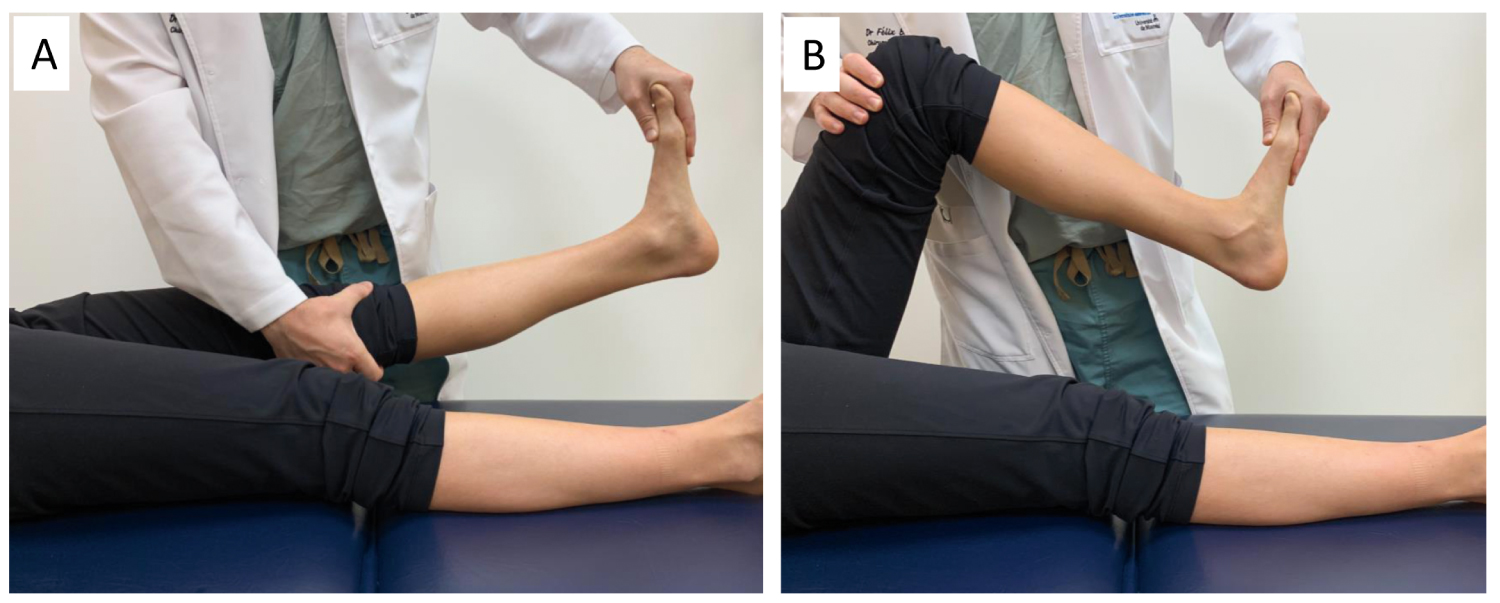 Figure 3: Silfverskiod test assessing passive ankle dorsiflexion in (A) Knee configurations; (B) Knee flexion.
View Figure 3
Figure 3: Silfverskiod test assessing passive ankle dorsiflexion in (A) Knee configurations; (B) Knee flexion.
View Figure 3
The foot and the wear pattern on the shoes should be inspected to detect pressure points, as weight will be concentrated laterally (Figure 4) and perhaps over the first metatarsal head [5,14]. A medial plantar callosity under the first metatarsophalangeal (MTP) joint and lateral border of the foot is common [2].
 Figure 4: Used shoe of a cavovarus left foot, showing wear on the lateral edge of the shoe.
View Figure 4
Figure 4: Used shoe of a cavovarus left foot, showing wear on the lateral edge of the shoe.
View Figure 4
The radiographic evaluation is of secondary importance, because correlation with clinical findings is minimal [2]. The four main radiological findings, namely: Meary's angle [1,6], the calcaneal pitch angle [1,15], Hibb's angle [1,5], and the medial arch height [2], can be seen in a lateral weight-bearing radiograph (Figure 5A and Table 1). The transverse talocalcaneal angle [16] (or Kite's angle [17]) (Figure 5B), the talus rotation [18] and the fibula posterior translation [3,4,19], are seen in standing AP radiographs [3].
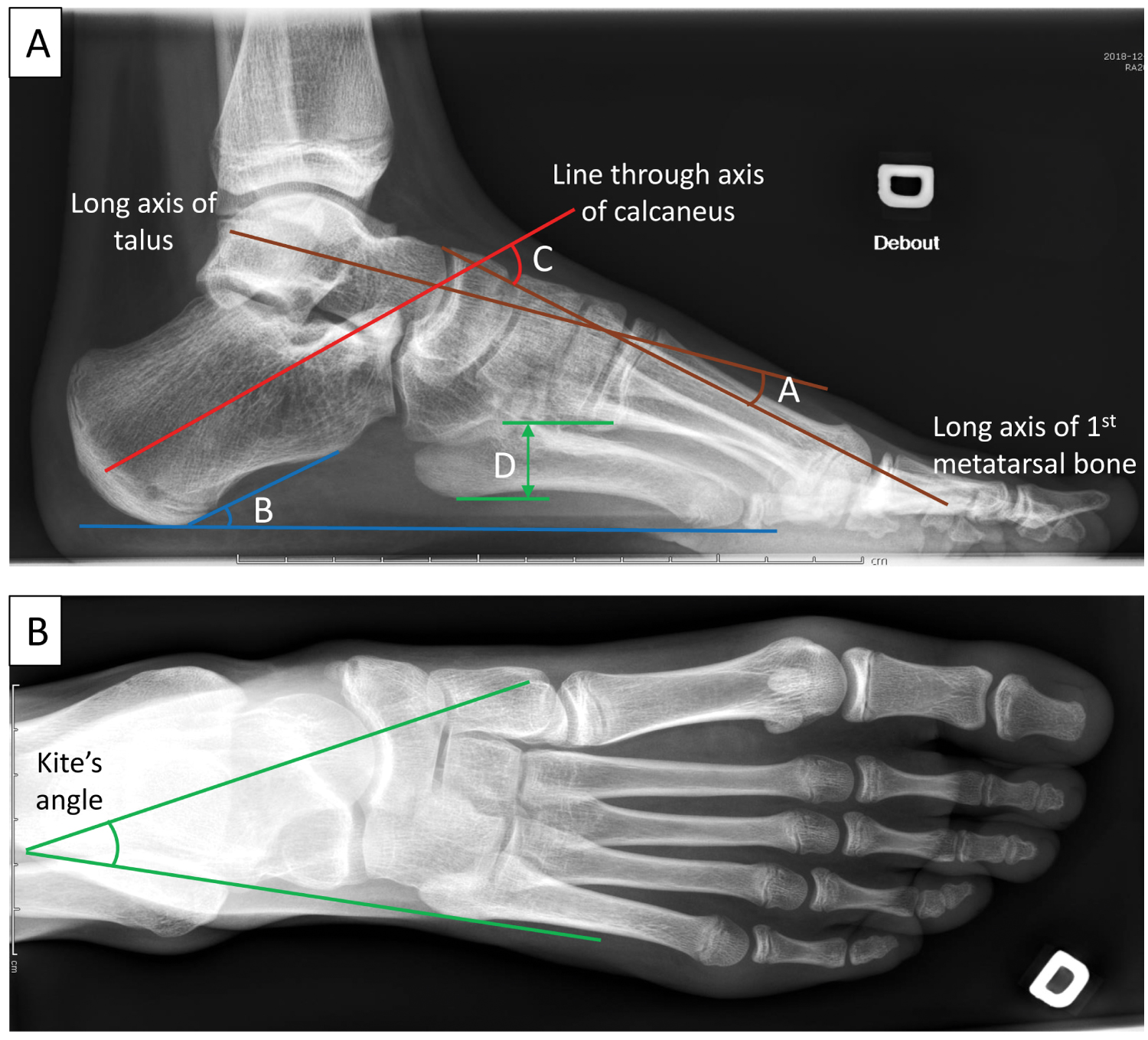 Figure 5: Radiological evaluation and measurements of the right cavovarus foot of a 12-year-old female patient.
(A): Lateral weight-bearing radiograph showing A) Meary's angle B) Calcaneal pitch angle C) Hibbs' angle D) Medial arch height.
(B): AP radiograph showing Kite's angle.
View Figure 5
Figure 5: Radiological evaluation and measurements of the right cavovarus foot of a 12-year-old female patient.
(A): Lateral weight-bearing radiograph showing A) Meary's angle B) Calcaneal pitch angle C) Hibbs' angle D) Medial arch height.
(B): AP radiograph showing Kite's angle.
View Figure 5
Table 1: Measurements on lateral radiographs in a standing weight-bearing position. View Table 1
Current literature [15,20,21] suggests that dynamic pedobarography is the ideal method for healthcare professionals (clinicians) to evaluate foot deformities and function, by analyzing plantar pressure values and distribution. More specifically, it is helpful for orthopaedic surgeons in the pre- and post-operative evaluation and classification of mild-to-moderate cavovarus deformities [15,21,22].
A normal, neutral arch has the least possibility of injury because of its even plantar pressure distribution. Any deviation from normal increases overall plantar pressure values in the stance phase of gait [22]. A typical, normal gait cycle has the most pressure located at the heel and forefoot, whereas the medial midfoot has significantly less pressure [23].
There is evidence [1,20] of progression from a flatfoot pattern in normal young children (under 2-years-old) to a curvilinear pattern in older children (over 5-years-old). As age increases, there is an increase in the percentage of maximum force at the heel and medial forefoot, while there is a decrease in maximum force percentage and time spent on the medial midfoot [20]. Consequently, appropriate age-matching should be taken into account when examining pediatric plantar pressure [20].
Subtle cavovarus foot with forefoot-driven cavovarus (positive Coleman block test) [14] presents with increased pressure on the heel, and perhaps the first metatarsal head. In a static standing posture, the subtle cavovarus footprint shows lesser or decreased pressure on the midfoot compared to a normal foot [10,24] (Figure 6). However, during gait, as the condition progresses to involve rotation of the hindfoot and midfoot, there is increased pressure on the lateral aspect of the foot and heel [1,2]. For example, in a study by Shojaedin et al., there was significantly lower peak pressure at the medial midfoot, and greater peak pressure at the heels and toes in badminton players with cavovarus deformity, compared to normal controls [25].
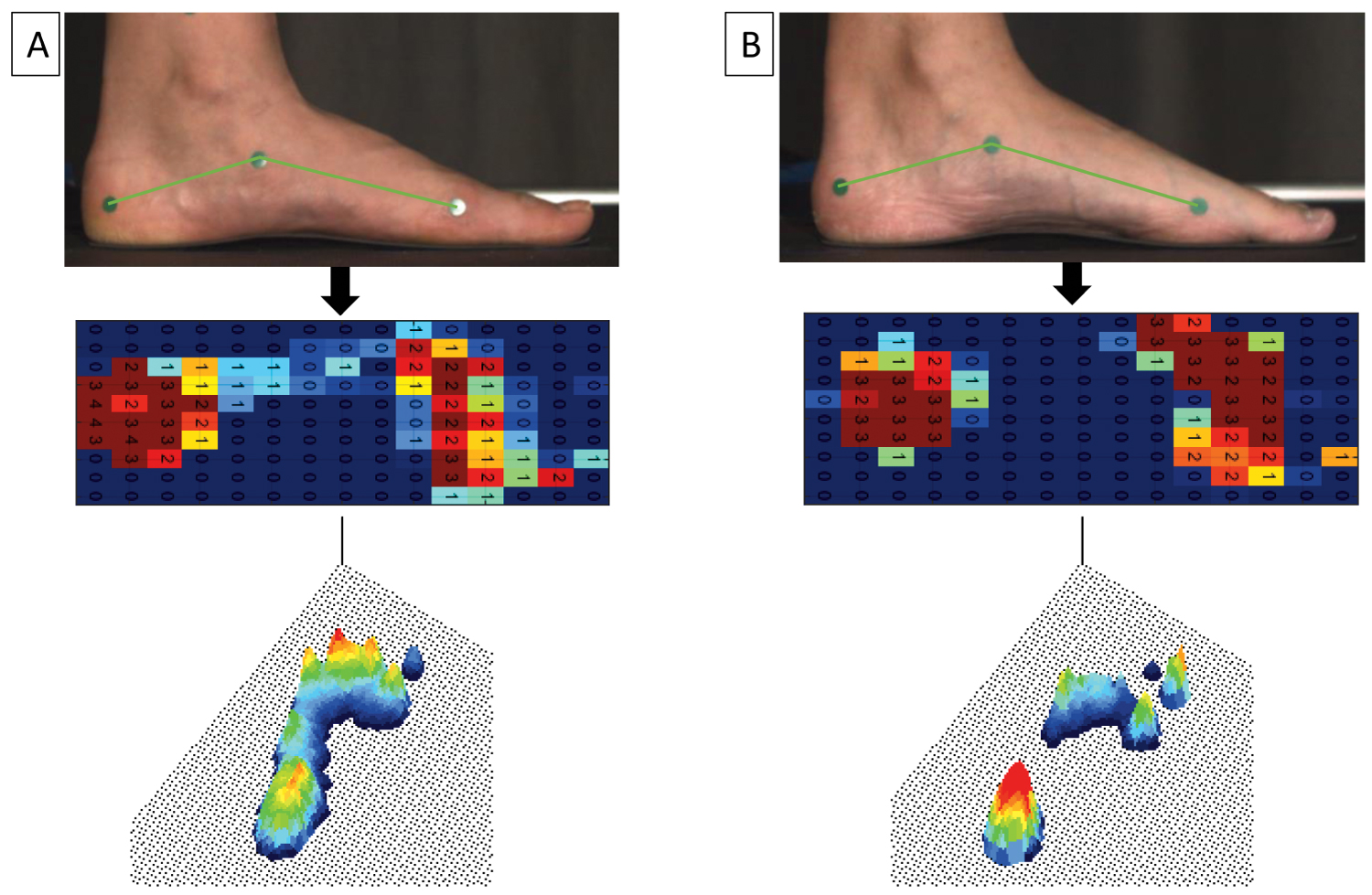 Figure 6: Static standing pedobarography in (A) normal vs. (B) cavus feet.
View Figure 6
Figure 6: Static standing pedobarography in (A) normal vs. (B) cavus feet.
View Figure 6
Studies of cavovarus feet with severe deformity have shown that only the lateral border bears significant weight when measuring foot pressure distribution [1]. In patients that simulated inverse walking patterns, the center of pressure was situated more laterally [26,27]. Severe varus feet had greater total pressure in the lateral midfoot and lateral forefoot, and decreased pressure in the medial forefoot [15]. They also had decreased and delayed initial peak forces of the hallux [22,26,28] while the first metatarsophalangeal joint displayed higher pressure compared to normal feet [29]. Dynamic pedobarography was able to detect an improvement in peak plantar pressure patterns, pressure-time integrals, and contact area in post-operative surgical correction of cavovarus deformity. It was also able to detect overcorrections of the metatarsals [21].
The pathologies associated with subtle cavovarus foot (Figure 7) include ankle instability [3,4,6,8,13,21,30], peroneal tendon pathologies [2,3,8,13,14], stress fractures [6,13] especially at the 5th metatarsal head [3,4], plantar fasciitis [3,8,10], ankle arthritis [11], forefoot equines [3,6], osteochondral talar lesion [8], mechanical metatarsalgia [8,10,11], hallux sesamoid disorders [3,4,8,14], Morton's neuroma [8,14], hallux valgus [8], and pain on the lateral aspect of the foot [6,10,11,13]. The Achilles tendon, which becomes a secondary inverter, is commonly pathologic as well [8,13,14].
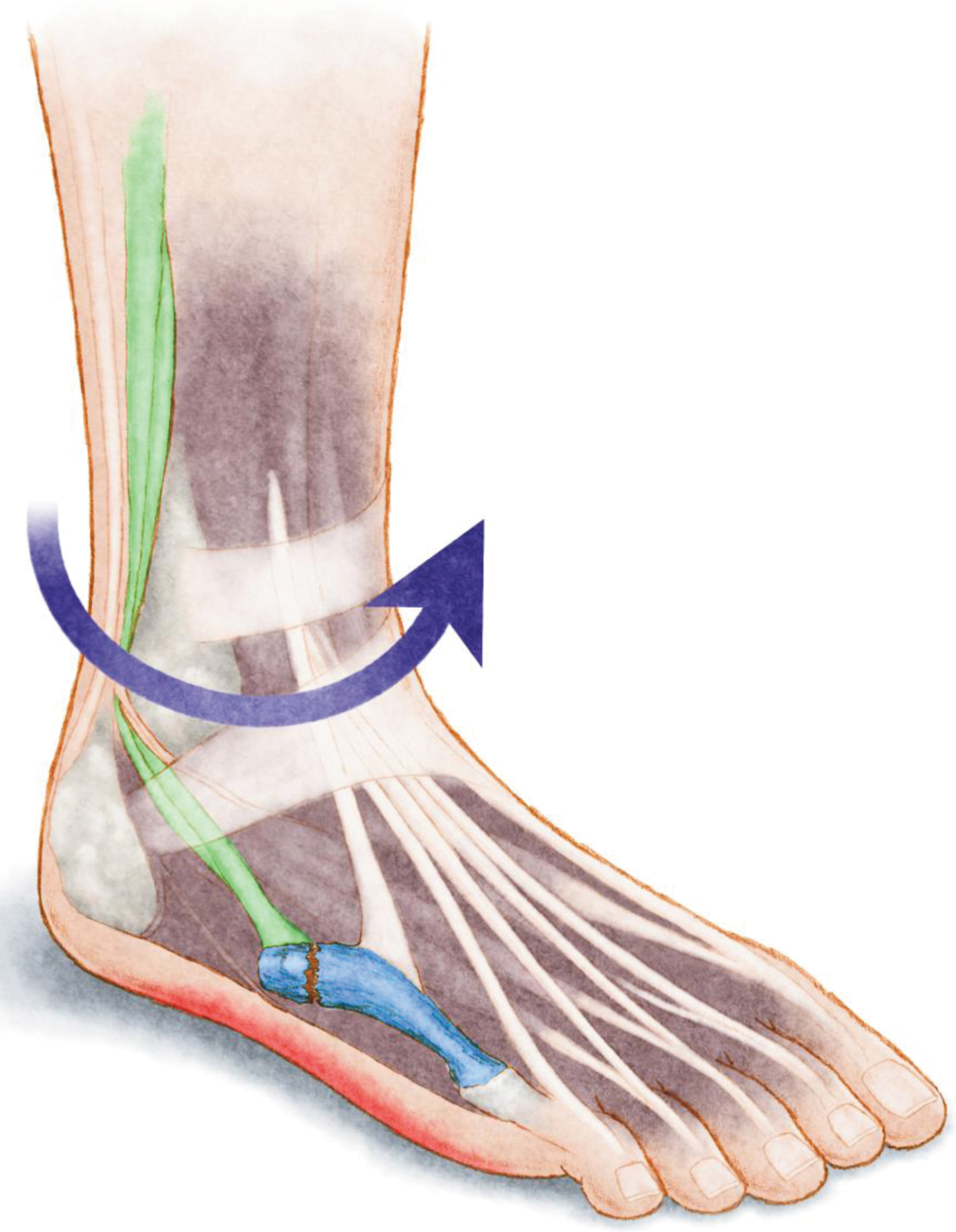 Figure 7: Anatomical illustration showing the most frequent injuries observed in subtle cavovarus feet: Ankle instability (purple arrow), peroneal tendinopathy (green), plantar fasciitis (red), and stress fracture of the 5th metatarsal bone (blue).
View Figure 7
Figure 7: Anatomical illustration showing the most frequent injuries observed in subtle cavovarus feet: Ankle instability (purple arrow), peroneal tendinopathy (green), plantar fasciitis (red), and stress fracture of the 5th metatarsal bone (blue).
View Figure 7
Lateral ankle sprains are one of the most common sports injuries, especially in soccer, and much research has been done to examine its risk factors [31,32]. Increased supination of the subtalar joint, increased plantarflexion foot positioning (for example, during touchdown in soccer) and delayed reaction time of the peroneal muscles, are critical etiological factors of ankle sprain injuries. Cavovarus feet are more prone to lateral ankle sprains because the foot cannot pronate adequately, secondary to peroneal muscle dysfunction. Following the sprain, anatomic alignment is preserved with the exception of an increased inversion and eversion subtalar range of motion in the injured ankle [33].
Studies report that muscle strength imbalances, such as an elevated eversion-to-inversion strength ratio, greater plantarflexion strength, and a smaller dorsiflexion-to-plantarflexion strength ratio, all had a higher incidence of inversion ankle sprains [33]. Other intrinsic risk factors included the cavovarus deformity or subtle cavovarus foot, a history of previous high-grade ankle sprains (strong evidence but not unanimous), physical activity, increased foot width, reduced ankle dorsiflexion, increased calcaneal eversion, subtalar instability, nerve injury proximal to the lateral ligament of the ankle [32], and impaired proprioception [33,34]. Limb dominance may also be a risk factor, but it is unclear if there is increased risk only for the dominant ankle or if no risk difference exists between ankles [35]. It should be noted that generalized joint laxity, ankle ligament stability, and anatomic alignment (besides subtalar motion) of the foot were not significant risk factors for ankle sprain injury [33,35].
Extrinsic risk factors for acute ankle ligamentous sprain in sports included artificial turf, not stretching before exercising, inferior single leg balance, increased sport intensity (during competitions), and the use of shoes with air cells (but no other shoe types). Obesity, or more specifically, the moment of inertia (square height times weight), is highly predictive of ankle sprains [34,35].
Repetitive ankle sprains have been associated with late sequelae, such as chronic ankle instability, pain, crepitus, swelling, stiffness and arthritis, suggesting the importance of its prevention [36]. Patients that complain about their ankle giving way during movements have either mechanical or functional instability [34,37,38].
Patients with chronic ankle instability tend to have a greater incidence of high foot arches, supination, and cavovarus deformities. Those with chronic ankle instability also have an altered gait pattern compared to normal controls [30,39]. They put a greater load on the midfoot and lateral forefoot, resulting in a lateral shift of their center of pressure and a more lateral gait. As a result, they hesitate when loading their forefoot and toes at the end of the stance phase, as they are unstable in plantarflexion [7,32]. This is significantly different from healthy controls and patients with lateral ankle sprains that have not developed chronic ankle instability. It is thought that either greater rearfoot inversion or decreased eversion (due to decreased peroneal muscle activity) results in greater loading of the lateral rearfoot during gait.
Given the above information, it appears that cavovarus deformity of the foot may predispose subjects to chronic ankle instability. Further research is required to investigate if untreated subtle cavovarus foot is a predictor for chronic ankle instability. Moreover, cavovarus foot is predictive of operative failure when treating chronic ankle instability, if the deformity is not corrected at the time of surgery [40].
The subtle cavovarus foot condition causes lateral soft-tissue structures, such as the anterior talo-fibular ligament and the peroneal tendons, to be stretched during gait. This results in peroneal tendon hyperactivity and is associated with peroneal tendinopathy and tear [2,3,8,14].
The literature has also shown that chronic ankle instability can lead to deficits in peroneal strength, peroneal muscle reaction time, peroneal subluxation, and impaired ankle proprioception [34,36,40].
Walking on the lateral aspect of the foot increases the risk of stress fractures of the fourth and fifth metatarsal and of the cuboid [2,4]. The sesamoid bones, medial malleolus, tibia and fibula also have a higher incidence of stress fractures, because there is significantly more pressure on the lateral aspect of the foot [1-3,12].
An extensive review of treatment is beyond the scope of this review. Therefore, a brief overview will be provided. Identifying athletes' foot type (or an inspection of the deterioration patterns of their footwear) could prevent these overuse injuries by adapting footwear to their feet (Figure 8). Management of pathologies associated to subtle cavovarus foot should target the alignment pathology prior to any lateral ligament/tendon repairs to avoid recurrence of symptoms [8,13]. The majority of cavovarus feet are flexible and conservative management could be indicated. Treatment should include flexible or semirigid [35], neutral insole orthoses to offload the lateral forefoot (Figure 9). Indeed, the only agreed upon protective intervention in the literature was the prescription of semi-rigid orthoses for soccer players with a history of a previous ankle sprain, and all basketball players, likely because it improved proprioception [31,34,35]. Physiotherapy and gastrocnemius stretching exercises should be done as well [4,6]. When the cavus deformity is forefoot-driven, appropriate orthosis should have posting of the lateral forefoot, along with recession under the first ray and lower support under the arch [4]. When it is hindfoot-driven, an orthosis with a lateral wedge at the heel can be prescribed, but might not be helpful because of hindfoot rigidity [12].
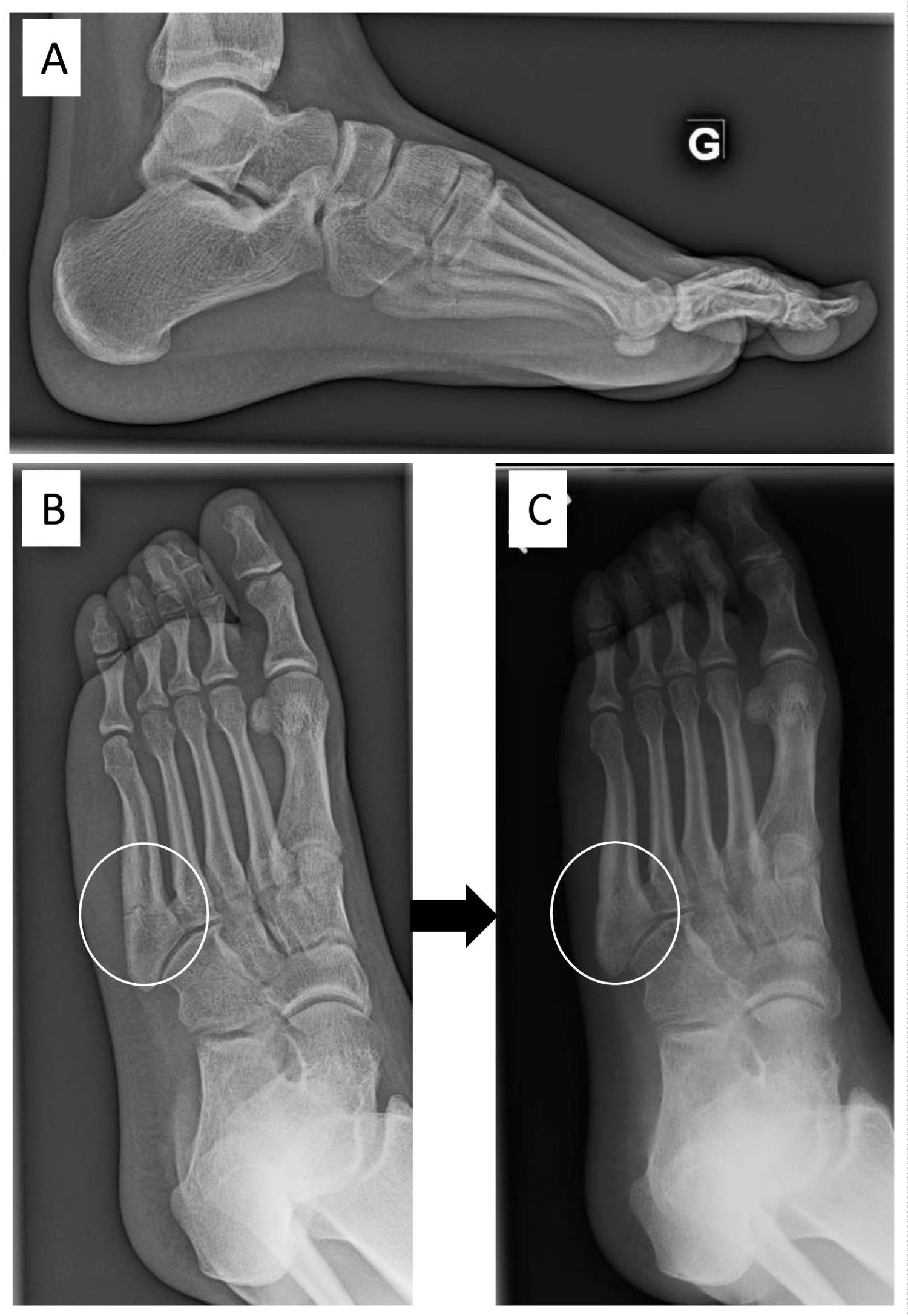 Figure 8: A 16-year-old female soccer player with a fracture of the 5th metatarsal in her left foot. She was treated with a non-weight bearing cast for 2 months, and progressively returned to sport. The same month, she fractured her 5th metatarsal bone (A, B). She wore a cast again and slowly healed. After 3-months, her subtle cavovarus foot was corrected with an insole. (C) After 6 months, she was clinically asymptomatic, returned to soccer with an insole and did not re-fracture.
View Figure 8
Figure 8: A 16-year-old female soccer player with a fracture of the 5th metatarsal in her left foot. She was treated with a non-weight bearing cast for 2 months, and progressively returned to sport. The same month, she fractured her 5th metatarsal bone (A, B). She wore a cast again and slowly healed. After 3-months, her subtle cavovarus foot was corrected with an insole. (C) After 6 months, she was clinically asymptomatic, returned to soccer with an insole and did not re-fracture.
View Figure 8
 Figure 9: Subtle cavovarus correction of a right foot using an orthosis. (A) Varus alignment of a right foot; (B) Plantar orthosis correcting the hyperflexion of the 1st metatarsal through a thinner medial portion highlighted in red and; (C) Foot correction with orthosis showing correct realignment.
View Figure 9
Figure 9: Subtle cavovarus correction of a right foot using an orthosis. (A) Varus alignment of a right foot; (B) Plantar orthosis correcting the hyperflexion of the 1st metatarsal through a thinner medial portion highlighted in red and; (C) Foot correction with orthosis showing correct realignment.
View Figure 9
Procedures for cavovarus foot are personalized and may include a lateral displacement calcaneal osteotomy [11,41], plantar fascia release [42,43], dorsiflexion osteotomy of the first metatarsal [44], peroneal longus to brevis tendon transfer [11,41], peroneal tendon surgery (Figure 10), Achilles tendon lengthening and arthrodesis, if it is severe [3,6,9,11]. In a high-level athlete that needs to return to play, or in refractory cases, surgery is indicated and often involves a first ray osteotomy [12], which has a very high success rate [5,45]. Post-operatively, the athlete will be in a splint for two weeks with no weight-bearing before progressing to a removable walker boot, and a return to athletics within 12 weeks [12].
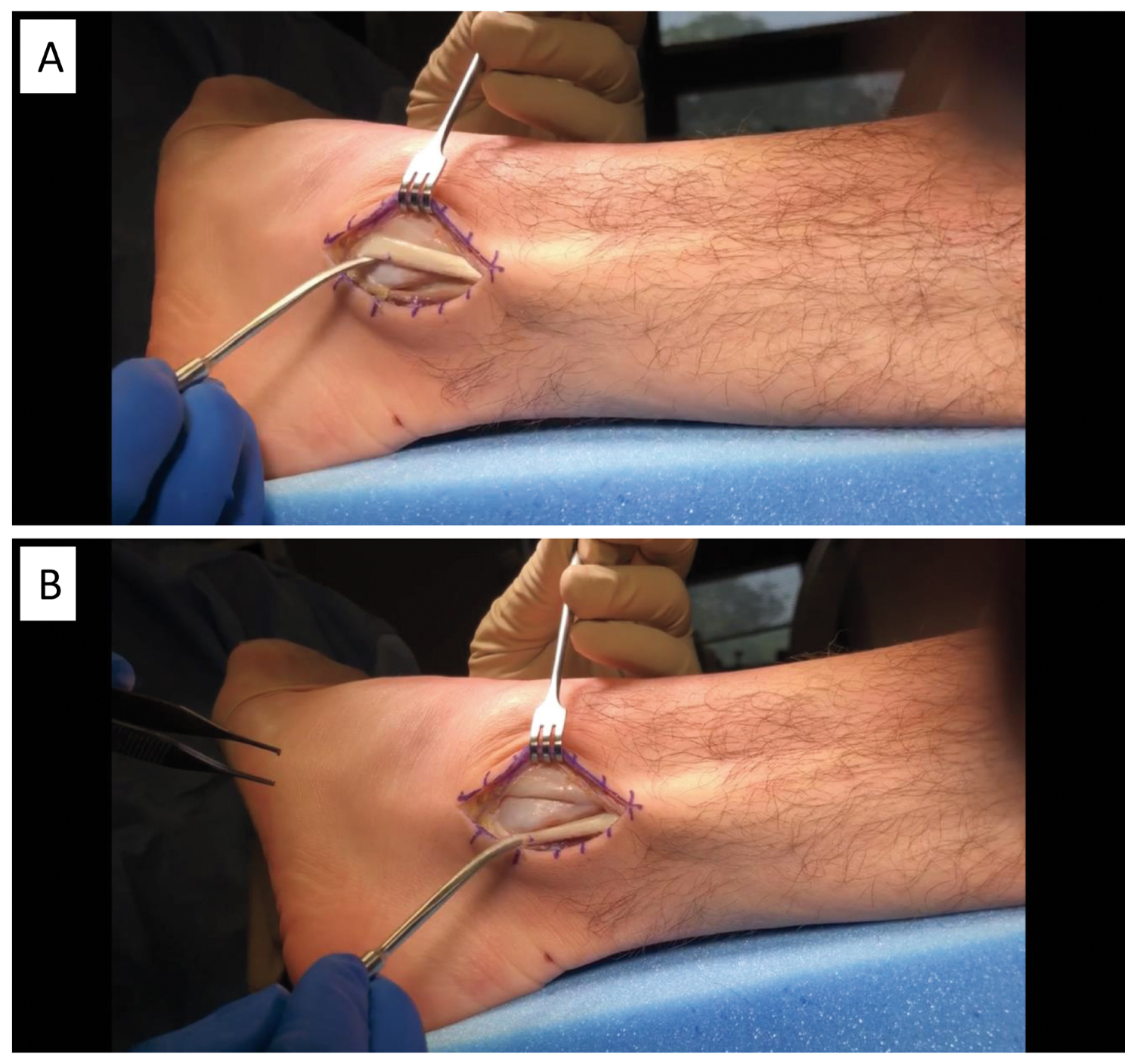 Figure 10: Surgery of peroneal tendons for chronic instability of a left foot with subtle cavovarus. (A) Peroneal tendons dislocated from behind the lateral malleolus; (B) Peroneal tendons in anatomical position behind the lateral malleolus.
View Figure 10
Figure 10: Surgery of peroneal tendons for chronic instability of a left foot with subtle cavovarus. (A) Peroneal tendons dislocated from behind the lateral malleolus; (B) Peroneal tendons in anatomical position behind the lateral malleolus.
View Figure 10
Subtle cavovarus foot places an athlete at greater risk for various foot and ankle pathologies. The diagnosis should be based on physical examination, standing feet radiographs and, if available, dynamic pedobarography. Subtle cavovarus foot alignment should be looked for in any case of chronic lateral foot and ankle pathologies, to help treatment and prevent recurrence after return to sport. Early identification and intervention with conservative treatments, such as semirigid foot orthoses, could eventually become an injury prevention measure for athletes in sports at greater risk.
Stéphane Leduc is a consultant for Stryker. The institution (HSCM) has received funding for research and educational purposes from: Arthrex, Conmed, Depuy, Linvatec, Smith & Nephew, Stryker, Synthes, Tornier, Wright, Zimmer Biomet. For the remaining authors, none declared.
This research was conducted as part of TransMedTech Institute's activities and thanks, in part, to funding from the Canada First Research Excellence Fund.
The authors would like to thank Kathleen Beaumont for editing and revising the manuscript.