Distal tibial metaphyseal fractures (DTMF) are rare fractures among children, and are usually treated by closed methods for 6 to 8 weeks with reported satisfactory outcomes. However, the choice of the surgical procedure if indicated, remains controversial, and many options of osteosynthesis are still considered. This a case of a traumatic progressively displaced DTMF despite cast immobilization in an 11-years-old child, who was treated in our institute by intrafocal pinning and followed for 15 months. We describe in this article the pathophysiology of this type of fractures as well as the technique applied. We compare afterwards our procedure to the other interventions in terms of advantages, disadvantages and final outcome. To best of our knowledge, no cases of intrafocal pinning for DTMF in children were described in literature before.
Tibia fractures are frequent during childhood, ranked as the third most common fractures in children [1], with an incidence of 15%. However, distal metaphyseal or supramalleolar fractures are not very common with an approximate incidence of 0.4% [2,3]. The majority of these fractures are greenstick injuries with a broken cortex posteriorly and a crushed cortex anteriorly [3]. Due to the thickness of the periosteum, a similar lesion would displace the distal fragment generally in a recurvatum and valgus angulation; nevertheless, a deformity by procurvatum and varus can occur [3,4]. Concomitant fibula fracture is a common finding and the pattern of its displacement mirrors the tibial one mentioned before. An intact fibula will lessen the severity of tibial displacement. A fibular fracture, present or absent, will not affect the final outcome no matter what type of care is provided [2].
When the displacement is acceptable, nonoperative treatment by closed reduction and a long leg cast for 6 to 8 weeks is the treatment of choice [5,6]. However, when conservative methods don't offer the optimal reduction and stability, surgical intervention is required to restore the length of the bone and correct its rotational angulation and alignment [5]. Indications for surgical treatment were defined as a recurvatum or a procurvatum of more than 10 degrees, a valgus or a varus of more than 5 degrees, or a misalignment of more than 40% [7]. The poor soft tissue coverage, the poor blood supply, and the distality of the fracture, arise a challenge in discerning what type of surgical intervention should be carried out [7]. Therefore, there isn't a "gold standard" surgical technique, and thus, the choice remains controversial [8]. Plating, elastic stable intramedullary nailing (ESIN), divergent intramedullary nailing (DIN), percutaneous pinning, external fixation and intrafocal pinning, all are debatable choices for surgery and each procedure has its own pros and cons [2,6,9].
An 11-years-old boy, with no medical history, and a BMI of 26.2 kg/m2, presented to the emergency department of our institution with severe pain in his left ankle following trauma. During examination, the pain was located in the supramalleolar region and an important swelling was noted. The patient was unable to bear weight on the affected limb. The neurovascular exam was normal. No accompanying lesions were found.
AP and lateral radiographs revealed a fracture of the distal tibial metaphysis with no significant displacement neither in the frontal nor in the sagittal plane. There was a limited recurvatum of 5 degrees with no varus/valgus deformity comparing to the other limb. There was also a concomitant fibular fracture (Figure 1). No osseous lesions were detected in the joints cranially or caudally to the fracture.
 Figure 1: Comparative AP and lateral radiographs at presentation showing the barely displaced fractures of distal tibia and distal fibula metaphysis.
View Figure 1
Figure 1: Comparative AP and lateral radiographs at presentation showing the barely displaced fractures of distal tibia and distal fibula metaphysis.
View Figure 1
The therapeutic strategy was going toward a conservative treatment with a non-weight bearing long leg cast for 3-4 weeks, then switching to a short leg cast for another 3-4 weeks. So, a long leg cast was done with 20 degrees of knee flexion and a plantar flexion of the foot to avoid secondary displacement. A control radiograph after casting revealed an increase in the recurvatum deformity that reached 9 degrees, still within the tolerable ranges (Figure 2).
 Figure 2: AP and lateral radiographs showing the increased but tolerable fracture displacement after casting.
View Figure 2
Figure 2: AP and lateral radiographs showing the increased but tolerable fracture displacement after casting.
View Figure 2
Follow up radiographs were performed during the first two weeks at day 7 and day 14, and the displacement had clearly increased. We had at day 14 a recurvatum of 19 degrees and a varus of 11 degrees (Figure 3). Therefore, at the present situation, surgical intervention was mandatory to restore the anatomy.
 Figure 3: AP and lateral radiographs showing displacement exaggeration two weeks after casting, (A) at day 7 and (B) at day 14.
View Figure 3
Figure 3: AP and lateral radiographs showing displacement exaggeration two weeks after casting, (A) at day 7 and (B) at day 14.
View Figure 3
Under general anesthesia, pinning was performed using two retrograde K-wires. The first was intrafocal and was used to achieve the reduction. It was introduced anteriorly and ended on the posterior cortex of the proximal fragment. At the same time, it gave the advantage to adjust and to maintain the reduction in the sagittal plane by its buttress effect on the distal fragment, hence limiting the recurvatum. The second K-wire was introduced medially, distal to the fracture, and ended on the lateral cortex of the proximal fragment to avoid posterior displacement (Figure 4). The K-wires were then cut beneath the skin. No stabilization was done on the fibula. The surgery was followed by a below knee non-weight bearing cast.
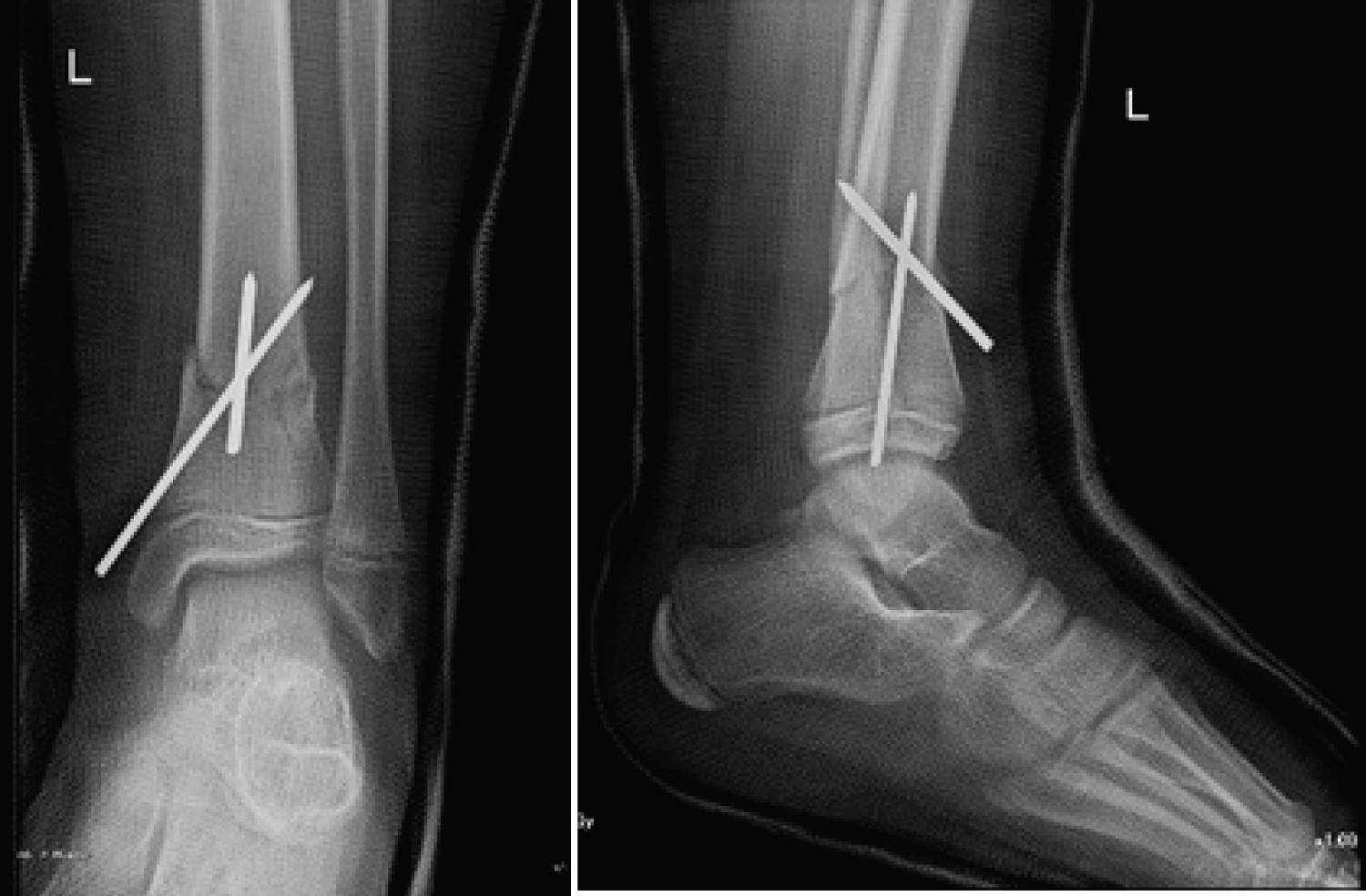 Figure 4: Post-operative radiographs showing the anatomical reduction and conservation by intrafocal pining.
View Figure 4
Figure 4: Post-operative radiographs showing the anatomical reduction and conservation by intrafocal pining.
View Figure 4
Two months after surgery, healing was marked on radiographs and the pins were consequently removed through a simple procedure (Figure 5). The patient was then examined. The range of motion in the operated side for both the ankle and the knee were evaluated with no difference compared to the non-operated side. Neither limb length dissimilarity nor malalignment were remarkable. No lameness was notable with full weight bearing. No surgery related complications were encountered during the past two months.
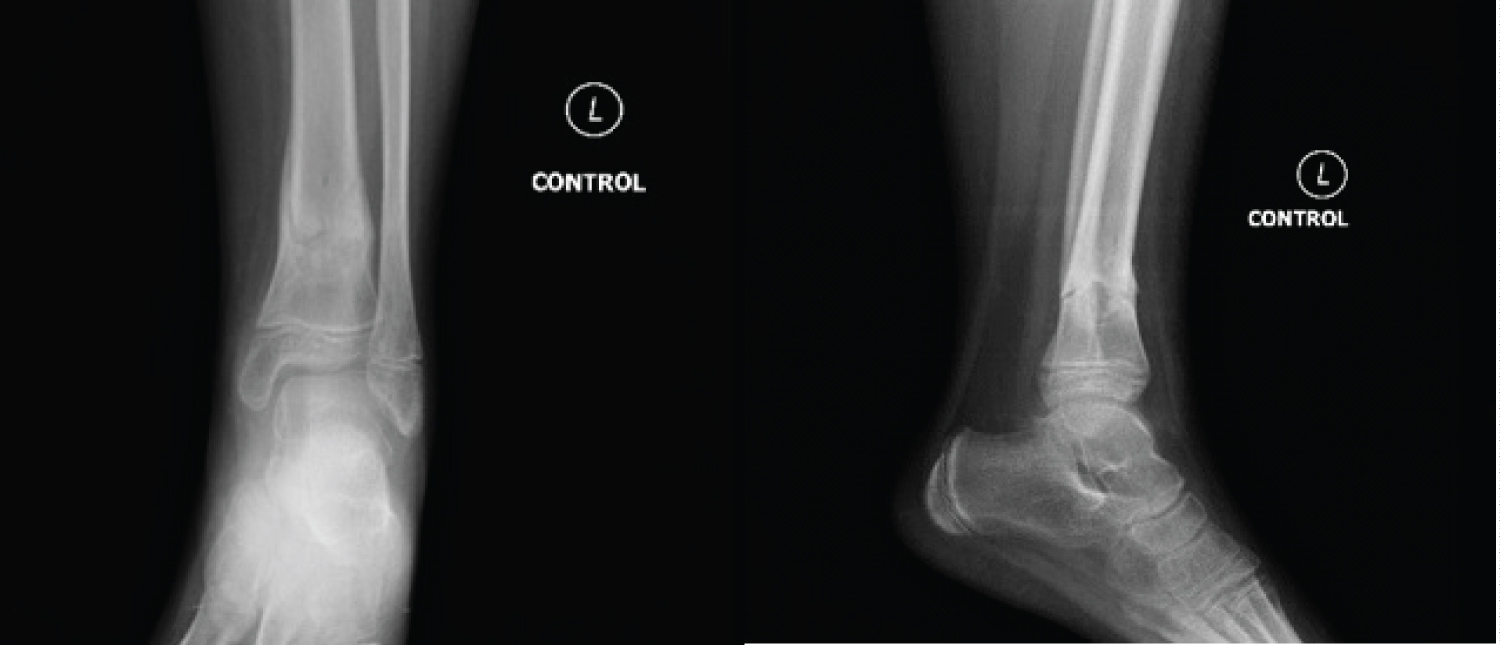 Figure 5: Two months after surgery radiographs showing evidence of fracture healing.
View Figure 5
Figure 5: Two months after surgery radiographs showing evidence of fracture healing.
View Figure 5
The patient was then seen and examined 15 months after surgery. The physical exam was absolutely normal with no eminent changes comparing to the last one. The radiographs have revealed total bone healing with respected length, rotation and alignment comparing to the other limb (Figure 6).
 Figure 6: fifteen months after surgery radiographs showing total and anatomical healing.
View Figure 6
Figure 6: fifteen months after surgery radiographs showing total and anatomical healing.
View Figure 6
This fracture type is considered an unstable fracture, and its secondary displacement is predicted for many reasons. First, in similar fractures with recurvatum, the posterior periosteum is lacerated while the anterior periosteum is intact [3]. Thus, the pull exerted by the anterior cortex with the absence of resistance by the posterior periosteum will augment the risk of displacement., especially with foot dorsiflexion. Second, because of the concomitant fibular fracture, the splint-like effect that is usually provided by the fibula to stabilise the tibial fracture is lost. Moreover, any fracture is prone to secondary displacement with conservative treatment after the subsidence of the edema and the disuse muscle atrophy, which will loosen the cast.
As mentioned above, the majority of distal tibial metaphyseal fractures in children are treated by closed methods when possible. The immobilization of choice is a non-weight bearing long leg cast that will be converted after 3 weeks to a short leg cast to prevent knee stiffness. Ideally, if an important swelling is present, a splint can be applied and then switched to a cast few days later after swelling resolution. However, due to the instability of the fracture, the mild edema in our case and the poor cooperation of the patient, the cast was performed straight away. The fracture was unstable to such a degree that the deformity has increased right after casting as shown on control radiographs (Figure 2). The cast was applied with 20 degrees of knee flexion to avoid the cast from slipping, and with foot plantar flexion to reduce and prevent any further recurvatum. The pattern of the fracture did not require any varus or valgus molding. The parents were than informed about the risk of compartment syndrome and we explained to them about the symptoms, if any appears, and how to monitor at home.
When it comes for surgery, there is no clear consensus concerning the technical choice. An overview of the literature shows that the most used and studied technique is the ESIN, but DIN, plating, percutaneous pinning and external fixation all are arguable techniques [2,6,9].
If we compare intrafocal pinning to ESIN, both are mini-invasive procedures and need to be followed by a short leg cast for 6 weeks. ESIN had proven its efficacy with good functional outcomes in many studies [2,4,5]. But due to the distality of the fracture, its instability and its closeness to the ankle, the challenge in ESIN is the difficulty in controlling the reduction in cancellous bone using elastic nails inserted in the proximal tibia. On the other hand, the superiority of intrafocal pinning are its easy manipulation and simple reduction of the distal fragment. Since the pin itself is used to correct the angulation and to maintain the reduction by its buttress effect, this technique poses no significant difficulties. The operator has to keep in mind using a large pin to avoid its breakage during reduction.
The same arguments are applicable on DIN when compared to intrafocal pinning.
Plating offers a direct and clear exposure to the fracture, and eventually helps to obtain an easy anatomic reduction and stabilization [8,10]. In contrast, plating is an intervention fraught with complications such as the risk of growth plate injury, soft tissue and coverage problems, bleeding, delayed union and infection. Important to mention is the need for a secondary major surgery for hardware removal. All these inconveniences are avoided in our technique.
Treatment with external fixation had leaded to satisfactory outcomes [7]. In addition to the classic post-operative worries with external fixation, in particular pin tract infection, children will be facing difficulty in accepting the presence of the hardware and in tolerating it in their daily activities. The high cost of external fixation should not be neglected also. These problems were prevented in our case. One of the worth to mention advantages of our technique is material lightness and simplicity.
Intrafocal pinning shares the same conveniences with percutaneous pinning in all its three configuration [9]. Nevertheless, the reduction management and maintenance by intrafocal pinning remain easier to achieve.
We would like to add that in our case, contrary to the literature, recurvatum displacement was associated with varus, whereas recurvatum is usually accompanied by valgus and procurvatum is accompanied by varus [3,4]. We think that the secondary displacement that occurred progressively during casting and not at the presentation would be the reason.
As a conclusion, we found that intrafocal pinning is an effective and safe choice for surgical treatment of DTMF in children. It contributes to the restoration of rotation, length and alignment of the bone. The advantages of light weight material, easy manipulation, minimal invasiveness, negligible blood loss, and short operating time make this procedure practical. The absence of reported complications so far and the simplicity of the secondary operation merit emphasis. Future prospective studies on significant samples of patients treated with intrafocal pinning for DTMF, should be regarded in order to confirm our findings, and to search for possible complications or discouraging outcomes.