Subtalar arthrodesis is the mainstay surgical treatment for subtalar arthritis, instability and malalignment. The purpose of this study is to synthesize the state of knowledge of outcomes after in situ subtalar arthrodesis.
A systematic literature review of three major medical databases (PubMed, Scopus, and Embase) was performed following Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. The literature was searched for studies in which subtalar arthrodesis was used to treat subtalar pathology from inception to December 1, 2020. The quality of research was assessed using a modified Coleman Methodology Score.
Twenty-six studies were included and reported on 815 patients and 839 feet. The average modified Coleman Methodology Score was 49.8 (range: 28-76, SD: 11.3). The most common complication was symptomatic hardware leading to hardware removal, reported in 11.4% of feet, followed by a 4.6% nonunion rate. Deep infection requiring surgery occurred in 1.3% of feet. American Orthopaedic Foot and Ankle Society scores were used in 37.7% of feet and improved from an average of 49.6 (range 33.0-61.7; SD: 9.6) to an average of 79.4 (69.0-88.0; SD: 5.5). Visual Analogue Scale pain scores were reported postoperatively in 18.4% of feet and improved from an average of 6.0 (range: 4.4-7.6; SD: 1.1) to an average of 1.6 (range: 0.9-2.9; SD: 0.7).
In situ subtalar arthrodesis has a union rate of 95.4%, reduces preoperative pain by more than half, and carries a roughly 17% rate of return to the operating room, primarily for hardware removal.
Level 2.
Subtalar arthritis, Calcaneus fracture, Posttraumatic arthritis
Subtalar arthritis, instability, and malalignment are common conditions causing hindfoot pain and disability. For patients who have failed nonoperative management, subtalar arthrodesis (STA) is the mainstay surgical treatment and leads to improved pain and outcome scores [1,2].
An array of STA surgical techniques exists, including open and arthroscopic approaches, in situ and distraction arthrodesis, with fixation strategies ranging from screws, staples, talocalcaneal nails, to pins. This systematic review focuses on the most commonly employed technique of in situ fusion with screw fixation via open or arthroscopic approaches.
Within the extant literature regarding STA, there is variability in the quality of research as well as the consistency of reported surgical variables. Therefore, we sought to assemble a group of studies that would meet stringent exclusion criteria and then 1) Describe the characteristics of this literature and 2) Describe surgical characteristics including indications, techniques, complications, and outcomes, as well as 3) Quantify union rates after STA.
A systematic literature review was performed following Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [3]. Three major medical databases (PubMed, MedLine, and Embase) were evaluated from inception through December 1, 2020, with the following search strategy: (subtalar OR subastragalus) AND (fusion OR arthrodesis). The bibliographies of articles of interest and reviews were additionally reviewed. Bidirectional citation searching was also used including backward and forward citation search methods [4]. There were no limitations on type of journal or publication date of the article. Only publications in English were included.
Inclusion criteria consisted of studies reporting on 1) Patients undergoing a primary isolated STA using screw fixation with 2) Reporting of clinical, surgical, complication, and radiographic outcomes with 3) An average follow-up ≥ 1 year. Clinical reviews, cadaveric studies, surgical technique papers, kinematic studies, patient-education articles, unpublished reports, and studies not written in English were not considered for inclusion. Studies that did not report union rate, complications, indications, and graft use were excluded. Additionally, studies reporting on fewer than 5 patients or on STA as part of a larger hindfoot surgery (e.g. tibiotalocalcaneal arthrodesis, triple fusion, Miller procedure etc.) were excluded. Studies using distraction arthrodesis technique were excluded. Use of xenograft was excluded. If an article was not omitted during the title and abstract review, the full text of the article was acquired and scrutinized in detail according to established inclusion and exclusion criteria. 26 studies ultimately met inclusion criteria and were included in this systematic review. A flow diagram of the literature search and selection process is illustrated in the Figure. The study selection process was performed independently by two observers (M.P., J.S.). If any inconsistency arose, the decision to include or exclude the study was made based on a group consensus.
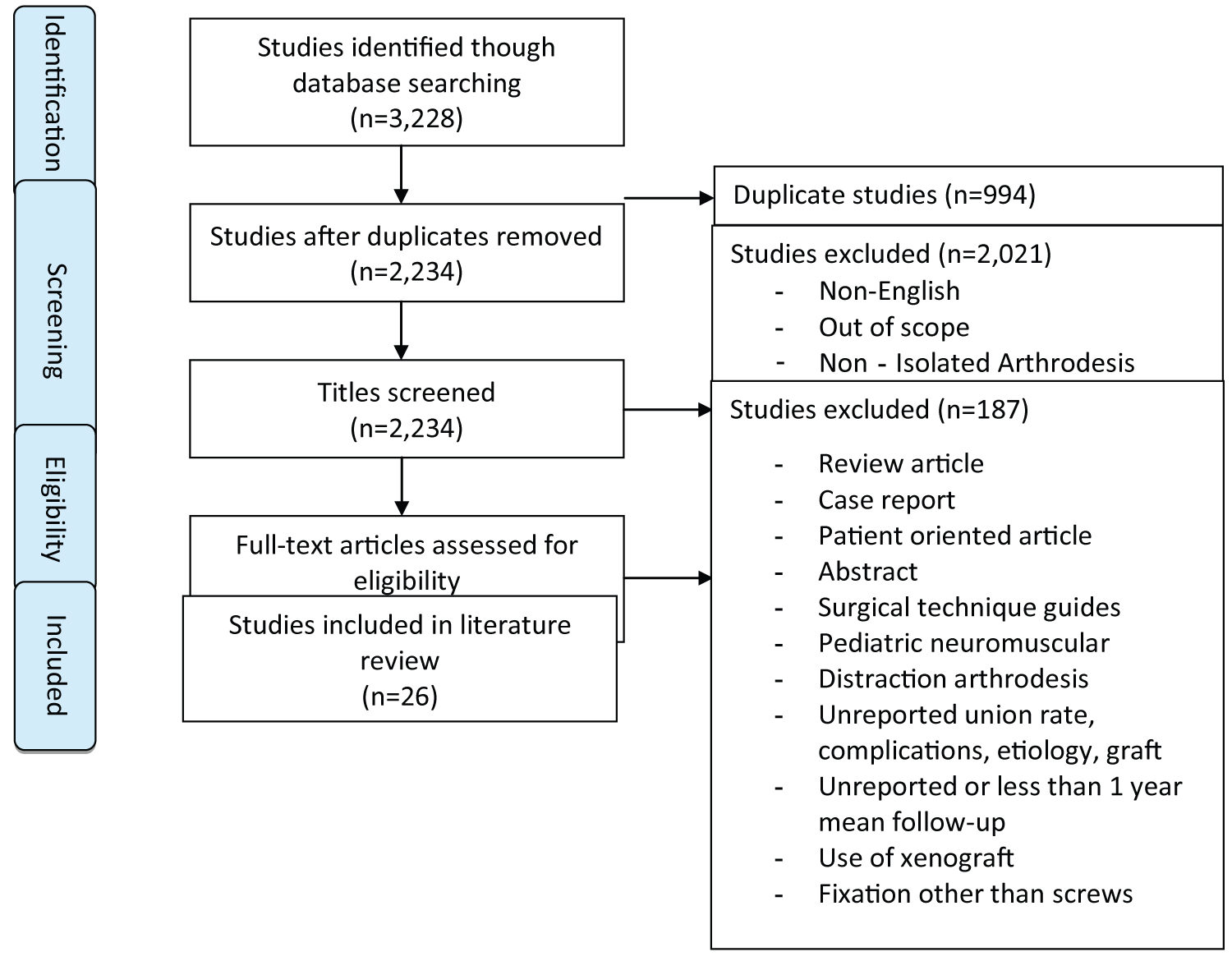 Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram.
View Figure 1
Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram.
View Figure 1
The following data were extracted from the included studies: type of study, level of evidence, number of patients and feet included, age and gender of patients, diabetes diagnosis, tobacco use, laterality, indication, surgical approach, bone graft use, fixation devices, complications, outcome scores, union rate, method of radiographic assessment of union, and radiographic outcomes. Data extraction was performed by 3 reviewers (M.P., J.S., N.B.).
The modified Coleman score, which is a well-established tool for this purpose [5], was used to assess the methodological quality of each included study (Appendix A) [6]. The modified Coleman score is a 2-part scoring system that grades studies based on 10 parameters. Part A assesses the size of study, variety of surgical procedures, study type, diagnostic certainty, surgical procedure, and postoperative rehabilitation. Part B evaluates the outcome criteria, protocol for measuring outcomes, and description of the inclusion process. The Coleman score is out of a maximum of 100. A higher score suggests that a particular study likely avoids chance, biases, and confounding factors. Four observers (M.P, N.B, A.B, M.S) performed the Coleman scoring after ensuring standardized grading and reliability among the four observers.
The characteristics of the included studies (prospective vs. retrospective, single center vs. multicenter, level of evidence, Coleman methodology score, follow-up duration, number of patients/feet), patient demographics (age and sex, diabetes, diagnoses, tobacco use), surgical details, and clinical and radiographic outcomes were summarized across all patients. Descriptive variables were summarized using weighted averages. All data were analyzed using IBM SPSS Statistics version 26.0 (IBM, Armonk, NY). We did not seek IRB approval for this investigation because we did not employ the use of protected health information.
Initially, 3,228 articles were identified through a literature search of which 994 articles were removed as duplicates. The remaining titles were screened and 2,021 were removed as they were not written in English, out of the scope, or had included patients with non-isolated STA. This left 213 articles for full-text review of which 115 were excluded as review articles, case reports, patient-oriented educational articles, abstracts or surgical technique guides. seventy-two more studies were excluded as they had less than 1-year follow-up, included pediatric neuromuscular patients, use of distraction technique, xenograft, fixation other than screws, had unreported union rate, complications, graft use or indications. Ultimately, 26 studies were included for analysis [1,7-31] (Figure 1 and Table 1).
Table 1: Demographics, clinical data, outcome scores from included studies. View Table 1
Of the included studies, three studies were classified as Level III evidence [23,26,27] and 23 studies as level IV evidence. One study was conducted at multiple centers [15] whereas 25 were single-center studies. Using a modified Coleman Methodology Score, the mean total score was 49.8 (range: 28-76, SD: 11.3) with part A mean score of 39.2 and part B mean score of 10.7.
Of 815 patients, 463 were male (60.5%), 302 female (39.5%), with sex unreported in 50 patients. Sixty-seven had surgery on the left foot (40.6%), 74 on the right foot (44.8%), bilateral surgery was performed on 24 patients (14.5%), and laterality of surgery was unreported in 650 patients. The weighted average age of patients was 47.3 years (range: 28.7-56.0; SD: 7.3) with age unreported in 77 patients (Table 1 and Table 2).
Table 2: Composite demographic data. View Table 2
Postraumatic osteoarthritis (PTOA) was the indication for STA in 68.2% of feet, the most common indication in this cohort. Of the patients with PTOA, 68.0% had calcaneus fractures. Lesser contributors to PTOA fractures of the talus, ankle, and tibial plafond [23]. Calcaneal fractures were treated with STA in both a delayed fashion as well as with primary STA at the time of injury [15,17,22,24]. Other indications include primary OA as well as secondary OA owing to posterior tibial tendon disfunction and tarsal coalition [10,14,17,27].
The most commonly used surgical technique among the included literature was a sinus tarsi incision to access the subtalar joint and two retrograde 6.5 mm screws starting at the plantar aspect of the calcaneal tuberosity crossing the subtalar joint. A variety of different approaches were employed to access the subtalar joint including extensile lateral, longitudinal posterolateral, lateral, and, rarely, medial approaches [12]. Additionally, arthroscopic approaches were utilized [8,13,19-21,23,27,28]. Screw size varied from 6.5 mm to 7.5 mm and number of screws ranged from one to three.
Bone graft was utilized in a majority of feet with local autograft from the lateral wall of the calcaneus or talus being most common. Iliac crest autograft was the other predominant source. Other autograft sources include proximal tibia, and fibula. Graft augments include demineralized bone matrix, bone morphogenic protein, and platelet rich plasma.
Union data were pooled with an overall reported rate of was 95.4% (800 of 839 feet). Of the group of successful fusions, a delayed union occurring between 6-9 months postoperatively was reported in 17 feet (2.1%). The methodology for assessing for union was subject to high variability and most commonly via a lateral projection x-ray, CT scan and physical exam with union defined as osseous trabeculation crossing the posterior facet of the subtalar joint. Presence of hindfoot pain was commonly reported as an indication for nonunion workup.
Complications data were pooled with symptomatic hardware and surgical removal of implants being the most common occurring in 96 feet (11.4%). Nonunion was reported in 39 feet (4.6%) of patients. Other complications include superficial infection not requiring surgical intervention which occurred in 17 feet (2.0%) while deep infection requiring return to the operating room occurred in 11 feet (1.3%). Sural neuropathy or nerve injury occurred in 14 feet (1.7%), complex regional pain syndrome was reported in 11 feet (1.3%), adjacent joint OA occurred in 7 feet (0.8%) and subfibular impingement occurred in 3 feet (0.4%). Symptomatic deep vein thrombosis (DVT) was reported in 2 feet (0.2%) (Table 3).
Table 3: Complications. View Table 3
Outcomes scores were not uniformly reported. Visual Analogue Scale (VAS) and American Orthopedic Foot and Ankle Score (AOFAS) were the most commonly reported outcome measures. Preoperative VAS pain scores were reported for 137 feet (16.3%) with a mean of 6.0 (range: 4.4-7.6; SD: 1.1). Postoperative VAS pain score was reported for 154 feet (18.4%), improving to a mean of 1.6 (range 0.9-2.9; SD: 0.7) at last follow-up. Preoperative AOFAS scores were reported for 255 feet (30.4%) with a mean of 49.6 (range: 33.0-61.7; SD: 9.6) with postoperative AOFAS scores reported for 316 feet (37.7%), improving to a mean of 79.4 (range: 69.0-88.0; SD: 5.5). Notably, the maximum possible AOFAS postoperatively is 94 due to the loss of subtalar motion (Table 4).
Table 4: Outcome scores. View Table 4
The purpose of this systematic literature review of in situ STA is to 1) Describe the characteristics of this body of literature and 2) Describe surgical characteristics including indications, techniques, complications, and outcomes, as well as 3) Quantify union rates after STA. To improve the quality of the included studies, a stringent inclusion and exclusion criteria was employed. Included studies had complete reporting of pertinent surgical details with ≥ 1 year follow-up to allow for assessment of union rate. As depicted in Figure 1, after screening for exclusion criteria, this systematic literature review of 26 studies regarding in situ STA evaluated a total of 815 patients with 839 feet. Despite stringent exclusion criteria, overall quality remained low with a mean Coleman methodology score or 49.8 out of a possible 100 points. Similarly, all studies were classified as level III or IV evidence.
The leading indication for STA in this cohort was PTOA, present in 68.2% of feet. This is consistent with a recent systematic literature review on arthroscopic STA which found that 70.35% of patients had PTOA [32]. This is also similar to tibiotalar arthrodesis, for which PTOA was reported as the indication for surgery in 70.0-79.5% of cases [33,34].
Overall, in situ STA union rates were found to be 95.4%. A systematic literature review on distraction STA had a comparable 94.9% union rate [35]. Similarly, two recently published systematic literature reviews on arthroscopic STA had union rates of 95.8% and 95.0% [32,36]. Additionally, in situ STA has a marginally smaller nonunion rate as compared to the 9% nonunion rate after tibiotalar arthrodesis [37].
Including the of the 4.6% rate of nonunion, the pooled complication rate among all included studies was 23.8%. The most common complication was symptomatic hardware requiring removal (11.4%), followed by nonunion (4.6%), superficial infection not requiring surgery (2.0%), deep infection requiring surgery (1.3%), sural neuropathy (1.7%) and complex regional pain syndrome (1.3%). Prominent and symptomatic hardware has been similarly shown to be the most common complication after distraction STA [35] as well as arthroscopic STA [32,36]. This review found a 1.7% rate of sural neuropathy with non-distraction technique whereas distraction STA had a 4.5% rate. Similarly, Non-distraction technique had a 3.3% rate of wound complications whereas distraction STA had a cumulative 6.8% rate of wound complications. We theorize that greater dissection and increased tension of soft tissue associated with distraction techniques may be responsible for this apparent increased risk of wound and sural nerve complications [35]. Patients should be counseled pre-operatively of the cumulative complication rate and an approximate 17% risk of need to return to the operating room for further procedures following in situ STA.
Patient reported outcomes scores were commonly assessed by the AOFAS scale which is difficult to interpret given concerns of this scoring system’s validity and the AOFAS recommendation against the use of this score [38]. However, VAS pain scores were reported as well, and on average showed an improvement after STA to 1.6 points from a preoperative score of 6.0. Patients should receive counseling that while STA greatly reduces pain, they are likely to have some level of residual pain postoperatively.
This systematic literature review was subject to limitations, largely attributable to the quality of the included studies. Quality of the included studies was limited by cohort size, which averaged 31.3 patients per study, the retrospective nature of data collection in all included studies, and AOFAS scores commonly used as the sole outcome measure, a score which does not meet validity criteria as it involves patient and investigator input without a logical framework for weighting [38]. A further limitation was the number of studies that did not include outcome scores in any form and which may have lead to an inaccurate estimation of improvement post-operatively. Additionally, important information on risk factors for complication and nonunion, such as diabetes and smoking status, were underreported. In an effort to mitigate the limitations of underreported data, studies that did not include details on union rate, complications, indications, and graft use were excluded. The large number of feet included in the study reduces, but does not completely eliminate, such risk of bias inherent when gaps in reporting such as this exist.
Current evidence for STA consists primarily of small retrospective case series with a moderately heterogenous group of patient and surgical factors. Overall union rate of STA was 95.4% and patients should be advised that STA will improve pre-operative pain but is unlikely to completely eliminate pain. Patients should be further counseled pre-operatively that STA carries an approximate 17% risk of return to the operating room, most commonly for removal of symptomatic implants.
We would like to acknowledge the contributions of Alexei Barg, deceased, in the conception of this study. No grants or funds were received to fund this study. C.L.S. is a consultant for Paragon 28 and Smith & Nephew. No assistance was received by medical writing experts.
None.
All authors contributed equally to the creation of this manuscript.