The aim of the present study was to assess the changes in cell membrane antigens on neutrophils from peripheral blood obtained from patients with pneumonia.
We obtained blood from twenty patients with pneumonia (16 men, four women; 67 ± 12 years of age). The expression levels of neutrophil membrane antigens were measured with a FACS caliber flow cytometer using several fluorescence-labeled monoclonal antibodies.
The expression levels of toll-like receptor 4 (TLR-4), a lipopolysaccharide recognition receptor, were higher in patients with pneumonia than in healthy individuals. In addition, the expression levels of CD64 (FcℽRI), an immunoglobulin G-binding receptor, were higher in patients with pneumonia than in healthy individuals. In contrast, the expression levels of CD11b and CD16 were lower in patients with pneumonia than in healthy individuals. The expression levels of tumor necrosis factor receptor (TNF-R) antigens were correlated with serum C-reactive protein concentrations. In addition, the expression levels of CD14, TLR-4, TLR-2, CD16, CD64, CD11b, TNF-R, and LFA-1 antigens were correlated with the ratio of immature neutrophils.
These results demonstrate that analyses of the surface antigens on neutrophils, which are strongly associated with biological defense or tissue injury, may be informative for understanding the pathology of pneumonia and for the development of new therapies targeting neutrophils.
Membrane antigens, TLR, FcℽR, Neutrophil, Pneumonia
FACS: Fluorescence activated cell sorting; CD: Clusters of differentiation; FcℽR: Fc-Gamma receptor; LFA-1: Lymphocyte function-associated antigen 1; IL: Interleukin; Mac-1: Macrophage-1 antigen; CR: Complement receptor; Ig: Immunoglobulin
Neutrophils play an important role in the phylaxis against pneumonia caused by bacteria and fungi. The recruitment of neutrophils to the lungs is a multistep process that involves granulopoiesis, neutrophil release, expression of neutrophil chemoattractants and cellular adhesion molecules, and the eventual transmigration of neutrophils into the alveolar spaces. Activated neutrophils play a major role in eliminating bacterial pathogens during infection.
Neutrophils employ the following mechanisms to recognize and eliminate microorganisms: [1] pathogen-associated molecular pattern recognition, represented by toll-like receptors (TLRs); [2] opsonization via complement receptors after complement activation; [3] and opsonization via antibodies produced during acquired immunity (including antibody-dependent cell-mediated cytotoxicity).
Neutrophils activated by various mediators including bacterial components such as lipopolysaccharide (LPS) or chemokines and inflammatory cytokines cause lung injury. Neutrophils adhere to the endothelial cells of microvessels in organs via adhesion molecules and migrate out of the vessels. During this process, toxic substances such as active oxygen and the enzymes produced by neutrophils may cause tissue or organ injury.
Neutrophils express many surface antigens, some of which (e.g., CD11b) are used as activation markers. Thus, analyses of surface antigens on neutrophils may reveal the neutrophil states and immune reactions against infection during pneumonia.
In this study, the expression levels of CD14 (an LPS recognition receptor), TLR-4, and TLR-2 (pattern recognition receptors), CD16 (FcℽRIII), CD64 (FcℽRI), CD11b (CR3, Mac-1), CD11a (LFA-1), CD120 (TNF-R) on neutrophil surfaces were compared between patients with pneumonia and healthy volunteers.
Twenty patients with pneumonia (16 men, four women; 67 ± 12 years of age) participated in this study. Twenty healthy volunteers (18 men, two women; 54 ± 6 years of age) were recruited as controls. The aims and significance of this study were explained to all participants to obtain informed consent. The protocol was approved by the Ethical Review Committee at Teikyo University School of Medicine (No. 07- 104). Peripheral blood was collected from patients with pneumonia and healthy volunteers.
Neutrophils from venous blood of pneumonia patients and healthy individuals were obtained following the procedure previously described [4]. In brief, neutrophils from pneumonia patients were isolated by employing the glucose dextran and ficoll (Amersham Pharmacia Biotech, France) method. The purity and viability of neutrophils was assessed by trypan blue dye staining. (Sigma, St. Louis, MO). An immature neutrophil (Stab) was assessed based on nucleus shape using Giemsa stain.
Cell surface receptor expression was measured as previously described [4]. The expression levels of neutrophil membrane antigens were measured with a FACS caliber flow cytometer (Becton Dickinson Biosciences: BD, San Jose, CA) with fluorescence-labeled monoclonal antibodies. Fluorescence-labeled anti-CD14, anti-TLR-4, anti-CD11b, anti-CD16, anti-CD32, anti-CD64, anti-CD128a, anti-CD11a, anti-CD120 (BD), and anti-TLR-2 (CEDALEN) antibodies were used to analyze neutrophil membrane antigens. For the quantitative analysis of fluorescence, 10,000 cells were collected and analyzed using Cell Quest software (BD). The fluorescence intensity of the cells was measured with a flow cytometer, and the data are presented as mean fluorescence intensity (MFI).
The Mann-Whitney U test was used to compare differences in anti-membrane antibody levels. Differences were considered to be significant when the two-sided p-values were < 0.05. Pearson's test was used for the analysis of the correlation.
Clinical data of patients with pneumonia are presented in Table 1.
Table 1: Clinical data of patients with pneumonia. View Table 1
The expression levels of TLR-4, TLR-2, and CD14 are shown in Figure 1. The expression levels of the CD14 antigen tended to be higher in patients with pneumonia than in healthy individuals (Figure 1a). The expression levels of TLR-4 were also significantly higher in patients with pneumonia than in healthy individuals (Figure 1b). The expression levels of TLR-2 in patients with pneumonia tended to be higher than those in healthy subjects; however, the difference was not significant (Figure 1c). Expression levels of these receptors were comparable between patients with pneumonia caused by gram-negative bacteria and those with pneumonia caused by gram-positive bacteria (data not shown).
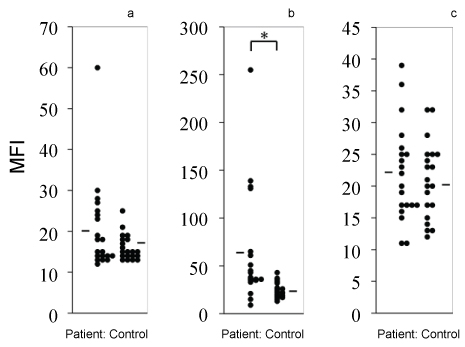 Figure 1: Expression levels of CD14 (a), TLR-4 (b), and TLR-2 (c) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
Figure 1: Expression levels of CD14 (a), TLR-4 (b), and TLR-2 (c) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
*P < 0.05 indicates a significant difference versus neutrophils from healthy controls.
MFI: Mean fluorescence intensity.
View Figure 1
The expression levels of CD16, CD32, and CD64 are shown in Figure 2. The expression levels of CD16 were significantly lower in patients with pneumonia than in healthy individuals (Figure 2a), whereas the expression levels of CD64 were significantly higher in patients with pneumonia than in healthy individuals (Figure 2b). The expression levels of CD32 did not differ between patients with pneumonia and healthy individuals. Furthermore, the expression levels of CD32 were separated in two phases.
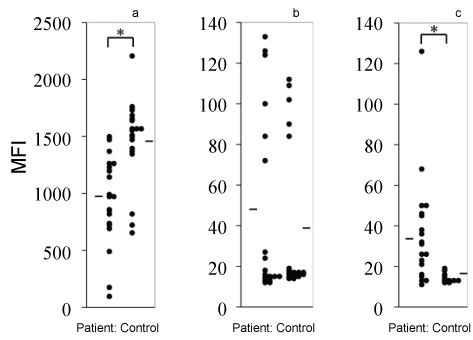 Figure 2: Expression levels of CD16 (a), CD32 (b), and CD64 (c) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
Figure 2: Expression levels of CD16 (a), CD32 (b), and CD64 (c) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
*P < 0.05 indicates a significant difference versus neutrophils from healthy controls.
MFI: Mean fluorescence intensity.
View Figure 2
The expression levels of CD11b were lower in patients with pneumonia than in healthy individuals. The expression levels of cytokine receptors such as interleukin-8 receptor (IL-8R) or tumor necrosis factor-receptor (TNF-R) were not significantly different between patients with pneumonia and healthy individuals (Figure 3).
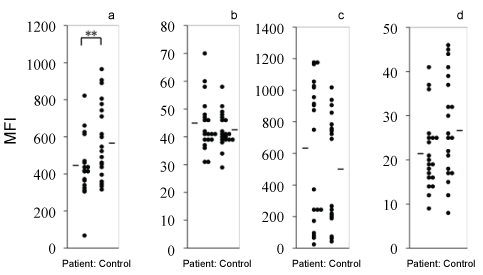 Figure 3: Expression levels of CD11b (a), CD11a (b), IL-8R (c), and TNF-R (d) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
Figure 3: Expression levels of CD11b (a), CD11a (b), IL-8R (c), and TNF-R (d) antigens on human neutrophils from healthy individuals and patients with pneumonia. Lines represent the means.
*P < 0.05 indicates a significant difference versus neutrophils from healthy controls.
MFI: Mean fluorescence intensity.
View Figure 3
The expression levels of TNF-R antigens correlated with CRP concentration in the serum (Figure 4). However, those of surface antigens, except TNF-R, did not.
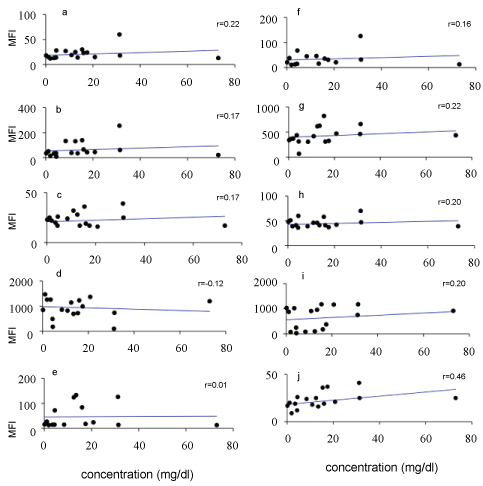 Figure 4: Correlative analysis of serum concentrations of CRP and expression levels of antigens. Expression levels of CD14 (a), TLR-4 (b), TLR-2 (c), CD16 (d), CD32 (e), CD64 (f), CD11b (g), CD11a (h), IL-8R (i), and TNF-R (j) antigens on neutrophils from patients with pneumonia. The CRP concentrations (mg/dL) in the serum of patients with pneumonia are also shown.
View Figure 4
Figure 4: Correlative analysis of serum concentrations of CRP and expression levels of antigens. Expression levels of CD14 (a), TLR-4 (b), TLR-2 (c), CD16 (d), CD32 (e), CD64 (f), CD11b (g), CD11a (h), IL-8R (i), and TNF-R (j) antigens on neutrophils from patients with pneumonia. The CRP concentrations (mg/dL) in the serum of patients with pneumonia are also shown.
View Figure 4
The expression levels of CD14, TLR-4, TLR-2, CD16, CD64, CD11b, CD11a, and TNF-R were correlated with the immature neutrophil ratio (Figure 5).
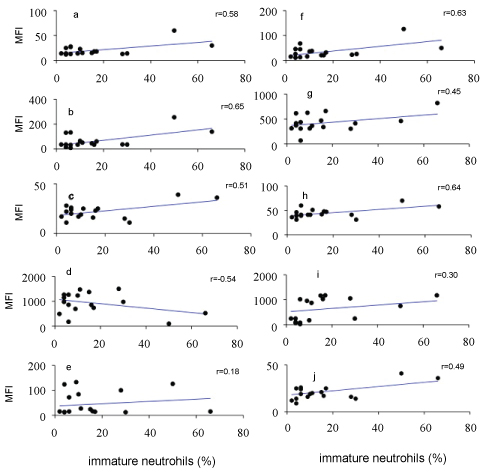 Figure 5: Correlative analysis of immature neutrophil ratio (% stab) and expression levels of antigens. Expression levels of CD14 (a), TLR-4 (b), TLR-2 (c), CD16 (d), CD32 (e), CD64 (f), CD11b (g), CD11a (h), IL-8R (i), and TNF-R (j) antigens on neutrophils from patients with pneumonia.
View Figure 5
Figure 5: Correlative analysis of immature neutrophil ratio (% stab) and expression levels of antigens. Expression levels of CD14 (a), TLR-4 (b), TLR-2 (c), CD16 (d), CD32 (e), CD64 (f), CD11b (g), CD11a (h), IL-8R (i), and TNF-R (j) antigens on neutrophils from patients with pneumonia.
View Figure 5
In the present study, changes in the expression levels of neutrophil membrane antigens were examined in patients with pneumonia and were compared to those in healthy individuals. We showed that the expression levels of TLR-4 were markedly increased in pneumonia patients, irrespective of the gram stain type of the causative bacteria. TLR-4 functions together with CD14 in recognizing LPS, a cell wall component of gram-negative bacteria, and activates cells [5,6]. By contrast, the expression levels of CD14 and TLR-2 tended to be unchanged between patients with pneumonia and healthy controls. TLRs activate cells through antigen stimulation via nuclear factor-kappa B, suggesting a correlation between the amounts of antigen and activation [7,8]. Bernhard, et al. [9] measured the expression levels of TLRs in monocytes from patients with sepsis. Septic patients had increased expression of CD14, TLR2, and TLR4 on monocytes compared to the controls. However, death due to sepsis is associated with the down-regulation of TLR2 and CD14 expression on monocytes and correlates with decreased cytokine-inducing ability. There are few reports on neutrophils in that respect. We previously reported the expression of CD14, TLR-4, TLR-2, CD16, CD11b, and IL-8R in neutrophils from patients with sepsis [4]. In neutrophils from patients with pneumonia, the expression levels of CD14 and TLR-4 were increased, and the levels of CD11b and CD16 were decreased. Neutrophil expression of CD14, TLR-4, CD11b, and CD16 showed similar changes in patients with pneumonia and patients with sepsis. Petit-Bertron, et al. reported that the expression levels of TLR-2 decreased in neutrophils in the blood of patients with cystic fibrosis but increased in those from inflamed sites of the lungs [10]. Thus, the expression levels of TLR-2 in neutrophils may change depending on the site of infection. Neutrophils around infected sites and those that have not yet migrated to the infected sites may show different states with respect to the expression of surface antigens. The expression levels of CD11b on neutrophil membranes were lower in patients with pneumonia than in healthy individuals. However, CD11b, a cell membrane antigen, is a known marker of neutrophil activation [11,12]. There is also a contradictory report that CD11b expression increases in response to inflammatory cytokines and chemokines [13]. The expression levels of CD11b increase in neutrophils activated by LPS, suggesting that cellular differentiation and activation are involved in the expression of CD11b in neutrophils. Decreased CD11b expression in the neutrophils of patients with pneumonia in the acute phase is presumably correlated with the count of immature neutrophils. Relja, et al. reported that the serum of patients with pneumonia reduces neutrophil CD11b expression [14]. Perhaps serum may contain substances that suppress the expression of CD11b. Thus, the expression levels of CD11b may decrease in clinical states in which inflammation develops with a rapid turnover of neutrophils. The factors affecting the migration of neutrophils include foreign migration factors (e.g., fMLP), as well as cytokines and chemokines (e.g., TNF and IL-8) and in vivo migration factors associated with complement (e.g., C5a). Many investigators have reported that neutrophil migration is suppressed in infected patients [15-17]. However, no marked change was seen in the expression levels of IL-8R in patients with pneumonia. Thus, signal transduction systems in neutrophils, but not decreased receptor expression, may be involved in the reduced migration of neutrophils in patients with pneumonia.
We found decreased expression levels of CD16 in neutrophils from patients with pneumonia. In contrast, the expression levels of CD64 were higher in patients with pneumonia than in healthy individuals. Neutrophils in infected patients have increased CD64 expression. CD64 expression on neutrophils could be a useful diagnostic for bacterial infections [18,19]. CD64 is a member of the immunoglobulin superfamily and is expressed on neutrophils. Its expression can be up-regulated by IFN-ℽ stimulation. CD64 binds the IgG immune complex and plays a role in antigen capture and in the phagocytosis of IgG-bound bacteria. Neutrophil adherence to the endothelium is known to be mediated in part by adhesion molecules such as LFA-1. There are many reports on the increased expression of CD64 on the membrane of neutrophils of patients with pneumonia, but there are few articles on changes in CD16 and LFA-1 expression. In this study, it was revealed that the expression of CD16 on the neutrophil membrane was decreased at the onset of pneumonia. There was no difference in the expression level of LFA-1, but it correlated with the ratio of immature neutrophils. Although CD64 has been shown to be a biomarker for bacterial infections including pneumonia, the potential of CD16 and LFA-1 expression as novel biomarkers is a subject to be studied in the future.
Upon stimulation of inflammatory cytokines like IL-6 and TNF, CRP is produced in the liver. The inflammatory cytokine TNF during infectious diseases increases TNF-R expression on neutrophils. The expression levels of tumor necrosis factor receptor (TNF-R) antigens were correlated with serum C-reactive protein concentrations. The other serum concentrations of CRP were not correlated with the amount of membrane antigen; however, the degree of maturity of blood neutrophils correlated with the amount of membrane antigen.
Collectively, our results suggest that analyses of some surface antigens on neutrophils may reveal neutrophil states and immune reactions against pneumonia caused by bacteria and can be used to identify useful biomarkers of bacterial infection.
We would like to thank Chizuru Miyazaki for technical assistance in collecting human neutrophils. This study was supported by the Private University Research Branding Project.
The authors declare no conflict of interest.