Objective: Calcitonin-gene-related-peptide monoclonal antibodies (CGRP-MABs) are newly-introduced but widely-used treatments for migraine. We aimed to characterize some predictors of clinical response to CGRP-MABs.
Methods: This was a retrospective chart review of patients started on CGRP-MABs at our academic headache practice in a 3 year-period. All patients met the criteria for migraine with or without aura, and/or chronic migraine as per the international headache classification ICHD-III.
We collected demographics, migraine characteristics, phenotypical features of the headache, and response to CGRP-MABs. Responders had a 50% or more reduction in headache days. We performed multi-variate analyses and a logistic regression model to determine if any baseline characteristics or phenotypical features aided in predicting CGRP-MAB response.
Results: 76 subjects were enrolled, 82% female (63/76), with a mean age of 40.2 ± 13.1. We had 64% (49/76) of the patients experience a response. Having autonomic symptoms (such as lacrimation, rhinorrhea, congestion) was associated with lower likelihood of response to CGRP MABs (OR 0.12, 95% CI [0.02 to 0.60, p = 0.015]), as was increased age with a lower effect size (OR 0.94 95% CI [0.88-0.99], p = 0.020). Increased BMI was not statistically significant as a predictor although there may have been a trend towards and effect (OR 0.40 95% CI [0.11-1.33], p = 0.142).
Conclusion: The presence of autonomic symptoms in migraine headaches may predict lack of response to CGRP-MABs. This study is limited by the small sample size. However, it is biologically plausible that presence of autonomic features is predictive of a decreased response to CGRP MABs as migraine patients with autonomic symptoms have higher levels of VIP correlated to this, and not CGRP(3). Our study raises the possibility that migraines with autonomic features may be at least in part VIP driven. Larger prospective studies are needed to confirm these findings.
Headache, CGRP, Antagonists, Migraine, Phenotype, Treatment
1. Migraine phenotype may affect its treatment options.
2. CGRP-MABs may have reduced response in migraine with prominent autonomic features.
Calcitonin-gene-related-peptide monoclonal antibodies (CGRP-MABs) have been accepted as effective treatments for migraine, with an overall favorable side-effect profile [1]. Four CGRP-MABs are currently FDA-approved for the treatment of migraine. The efficacy of CGRP-MABs in preventing migraine are comparable based on the date available from their clinical trials, with a reduction of migraine frequency by more than 50% in more than half of the patients receiving them [2]. In clinical practice, CGRP-MABs have shown a variable response, with some patients reporting drastic improvement in their headache frequency, some reporting mild to moderate improvement, and some reporting no improvement at all. Unfortunately, at the present time we have no available markers on predicting how a certain individual would respond to CGRP-MABs. The lack of uniform response may be related to the heterogeneity of migraine disorder, [3,4] the differing levels of CGRP in certain individuals or migraine attacks, [5,6] and/or the differing pharmacodynamics or immunogenicity of CGRP-MABs among migraineurs [7-9].
There has been a push for finding predictors of response to treatment. It is clinically valuable and scientifically hypothesis-generating in characterizing features, whether clinical or physical (genetic markers, blood levels of molecules etc), that predict response to certain medications. Others have looked at features of the migraine disorder in general, and the phenotypical features of their individual attacks [10,11]. For example, it has been shown that migraine with aura is less responsive to triptans that migraine without aura [12,13], and onabotulinumtoxinA is more effective in migraines described as "imploding" rather than "exploding". [14-16], and a recent study suggests certain phenotypical profile predicts response to "frovatriptan" specifically [17]. Similar efforts to phenotype headache attacks have been carried on in other primary headache disorders such as cluster headache [18].
In this study we attempted to characterize, a possible association between the migraine characteristics, and phenotypical features of attacks as reported by the patients, and the response to CGRP-MABs.
We performed a retrospective chart review and identified all patients who presented to our academic headache clinic (State University of New York Upstate Medical University, Syracuse, New York) in the 3 year-period between June 1, 2018 and May 31, 2021, whom we initiated on CGRP-MABs. All patients met the criteria for migraine with or without aura, and/or chronic migraine per the international headache classification ICHD-III.
We recorded demographics, medication history, migraine characteristics including duration of migraine, diagnosis of chronic migraine, history of concussions, features of cervicogenic headache (including neck pain, occipital tenderness and facet tenderness) and presence of allodynia.
Finally, we also reviewed the detailed descriptions of their headache attacks including multiple variables:
1. Aura
2. Nausea/vomiting
3. Photophobia or phonophobia
4. Autonomic features (lacrimation, rhinorrhea, sinus-congestion, facial or orbital swelling).
We recorded their current migraine headache frequency based on recall at the initial visit when CGRP-MAB was started, and at their follow-up visit (3 to 12 months after).
Response to CGRP-MAB was categorized based on reduction of reported migraine days into responders (more or
The pre-planned primary outcome measure of this study was the categorical variable of 50% response rate. The primary analysis of the data was undertaken using pre-planned testing. We did not perform statistical power calculations, but rather used available data at time of study initiation.
Descriptive statistics were compiled using means and standard deviations (SD) or frequencies and percent (%) as appropriate to the data. Univariate analyses between demographic and clinical characteristics and response level used chi-square tests of independence or Fisher exact tests for categorical variables or t-tests for continuous variables. Variables that were felt to be related to response level in univariate analyses were entered into a logistic regression model to determine adjusted odds of having a lower response, we used univariate and multi-variate logistic regression to account for confounders in possible interactions. For all analyses, alpha = 0.05 was used to determine statistical significance. Analyses used R statistical software and R studio.
76 subjects were enrolled, of which 30 received Erenumab, 36 received Fremanezumab, 9 received Galcanezumab and 1 received Eptinezumab.
Baseline characteristics of enrolled subjects are summarized in Table 1.
Table 1: Descriptive characteristics by CGRP medication type. View Table 1
All the baseline features of biologic sex, age, duration of migraine disorder, post traumatic headache and BMI and headache associated features of aura, allodynia, phonophobia and photophobia, nausea, and autonomic symptoms were analyzed using chi-square tests of independence or Fisher exact tests for categorical variables or t-tests for continuous variables to see if there was a relationship with likelihood of response. This is represented in Table 2.
Table 2: Descriptive characteristics by response to CGRP MABs. View Table 2
We find that chronic migraine diagnosis and presence of autonomic symptoms were related to likelihood of response to CGRP MABs.
We studied these relationships further in univariate and multivariate logistic. A logistic regression was then done to adjust for confounders or interactions utilizing the variables we felt could have a significant effect on likelihood of response from previous analysis. We did multiple iterations of model selection for multi-variate model, and model was optimized at an AIC of 99.6 and C statistic of 0.86. Of all the collected features, having autonomic symptoms (such as lacrimation, rhinorrhea, and congestion) was correlated with decreased chance of response to treatment (OR 0.14, 95% CI [0.03-0.60]) (Figure 1 and Table 3). Age was also a predictive factor of a smaller effect size (OR 0.94 95% CI [0.88-0.99], p = 0.020). Increased BMI was not statistically significant as a predictor although there may have been a trend towards and effect (OR 0.40 95% CI [0.11-1.33], p = 0.142).
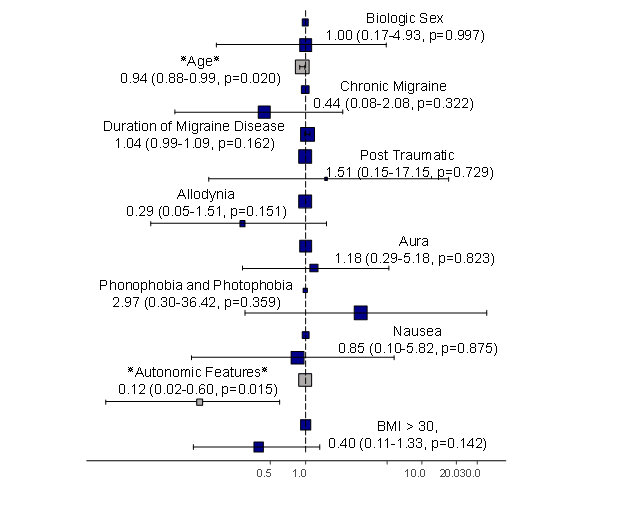 Figure 1: Forest plot of odds ratio of response to CGRP MABs.
Figure 1: Forest plot of odds ratio of response to CGRP MABs.
Odds ratio crossing 1 means no significant effect of variable on response to CGRP MABs.
BMI: Body Mass Index.
View Figure 1
Table 3: Likelihood of response based on characteristics. View Table 3
The standard clinical practice in classifying primary headache disorders has been solely based on their clinical features, rather than on genetic sequencing, biomarker profiles, or imaging findings [19]. Hence, neurologists and headache providers are accustomed to managing patients based on the phenotypical description of their attacks, even when it falls in the grey zone between different headache entities such as in migraine-cluster, or migraine-trigeminal neuralgia [20-22]. Studies have suggested that significant variability exists in the underlying mechanism of migraine [23], and in its response to certain treatment [24]. Attempts to identify certain clinical phenotypes that can guide the choice of pharmacological management has been undertaken in prior studies with CGRP MABs [25-30].
In our study, we collected clinical features and baseline variables that may have affected the response of CGRP-MABs.
Our study identified two factors as predictive of a response, the presence of autonomic features and age of patients. Patients who experienced autonomic features with their headache were more likely to report worse response compared to their peers without autonomic symptoms. This was unexpected. Previous studies have suggested that migraine with autonomic symptoms represents a clearly different entity from migraine without autonomic features [31,32]. Some differences in pathophysiology have also been proposed since autonomic symptoms usually indicate involvement of the parasympathetic nervous system (predominantly sphenopalatine ganglion SPG) [33,34], rather than the typical pain related to trigeminal activation. Trigeminal pain is largely determined by the sensitization of its nerve-endings by CGRP [35], while the same mechanism is not identified in parasympathetic mediated symptoms [36]. Mechanisms of parasympathetic mediated pain include a flow of post-ganglionic parasympathetic signal, and secondary sensitization of trigeminal nucleus caudalis in the brainstem [33]. Either mechanism may be proof to the effect of CGRP-MABs which has no parasympathetic inhibiting properties, and does not penetrate the CNS [35]. There is some evidence that presence of autonomic features in migraine is associated with increased VIP levels, and not CGRP levels [37]. We show that autonomic features may be predictive of a decreased response to CGRP MABs. This may indeed be because there are higher levels of VIP correlated to this, and not CGRP [37]. Our study raises the possibility that migraines with autonomic features may be at least in part VIP driven.
Although we found only a trend toward BMI effect, our study may not have been powered to detect this association that has been reported [28,38]. There is some evidence that CGRP levels decrease with bariatric surgery in obese patients [38] and these previous findings do raise the question if the levels in obese patients of CGRP may be so elevated in obese patients that dosing may not be adequate. Larger studies may be informative on this issue, and perhaps considerations for dosing regimens depending on weight need to be studied.
There are numerous limitations of our study, including its single center design, small sample size and dependance on patient reporting at time of their visit. These features render our study prone to some biases. We hope this is a hypothesis generating study, and other groups study the association of autonomic phenotypic features and response to CGRP medication. Reproducing the results in more stringent clinical studies will be of great value in shedding light of different aspect of migraine pain, and perhaps getting closer to individualized approach to migraine treatment based on its phenotypical features.
The study was declared as exempt from review by the institutional review board IRB of SUNY Upstate Medical University.
The authors declare that they have no conflict of interest.
No funding was required for this research.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
AZ and AR collected the date. AZ and IM wrote the manuscript. GB and IM performed the data analysis.