Introduction: Interactions between cancer genesis, sleep quality and patient's humor engage complex pathophysiological pathways. However, the outcome of various indicators of quality of life (Qol) after chemotherapy in non small cells lung cancer (NSCLC) and also their prognostic impact remain understudied.
The objective of this study was to analyze the Qol, sleep quality and anxio-depressive disorder in advanced NSCLC patients put on chemotherapy. We aimed also to demonstrate the correlation between the Qol and overall survival (OS) of the cohort.
Methods: In this monocentric prospective study, we included all patients with metastatic NSCLC, put on chemotherapy regimen from January to December 2018. We assessed the Qol, the sleep quality and disturbances of humor through dedicated questionnaires in Arabic Tunisian dialectal version. Concerning the outcome, the study mentioned the response to chemotherapy and the overall survival. The point date was on December 31st 2019.
Results: Seventy one male patients were included. Their mean age was 62.17 years. Adenocarcinoma was the most frequent histologic type (58%) and then was squamous cell carcinoma (25%). When analyzing QLQ-C30, we found a significant correlation between the global Qol coefficient and the coefficient of performances, an inversely proportional correlation with the coefficient of symptoms. Analysis of PSQI score had shown a poor sleep quality in 55% of patients after chemotherapy. A depressive humor was detected in 21 patients (30%) and an anxious humor in 24 patients (34%). Twenty six patients (37%) had a tumor regression after 1st line of chemotherapy. Mean OS was 317 days (IC = 95% [292-377], margin of error of 20 days) with extremes from 1.6 months to 21 months. One year survival rate was 44%. Statistical analysis had shown a closely comparable OS in our patients, whatever was the chemotherapy regimen. OS was correlated to Performance Status, response to chemotherapy, good sleep quality and high levels of performance dimensions. Multivariate analysis found poor sleep quality and tumor progression after chemotherapy as independent predictive factors of mortality.
Conclusions: Considering our results, we highlight the important decline of Qol in NSCLC patients, affecting several dimensions, whatever was the molecules of chemotherapy used. This decline would be predictive of a poor prognosis.
Non-small cell lung cancer, Quality of life, Chemotherapy, Survival
The prognosis of non small cell lung cancer (NSCLC) has been the subject of several clinical trials. Researchers have tried to look for predictors of the prognosis. Clinical, biological, pathological or cytogenetic markers, outcome to treatment and overall survival time were described [1-3].
In our context, the optimal management of broncho-pulmonary cancer requires an experienced multidisciplinary team to establish the indications of invasive explorations and treatment, to provide the necessary care, including anti-temporal or complementary treatment without forgetting the preservation of quality of life [5]. Supportive therapies are increasingly prominent in daily oncology practice [6-9].
The emotional impact of the diagnostic announcement, the psychosomatic manifestations that accompany it, have been studied and described. For patients with cancer, these disorders are frequent, severe, long-lasting and sometimes late-onset during or after chemotherapy [10-13]. Frequently, scientific literature reported and described abnormalities including nociceptive or neurogenic pain, cognitive disorders, psychological disorders (anxiety, depression, regression reaction, ritual application), substance abuse, or rather drug addiction and sleep disorders, especially insomnia. For a better specific description of any complaint, its severity, evolution and resolution, dedicated scores have been established and objectively validated.
However, the correlation between different quality of life indicators in stage IV lung cancer patients with the mean overall survival was not studied in Tunisia.
The aim of this study was to analyze quality of life, sleep quality and quality of humor in patients with stage IV lung cancer and put on chemotherapy. We aimed also to assess the correlation between quality of life indicators with the prognosis of the disease.
This was a single-arm prospective descriptive cohort study conducted in the pulmonology department Pavilion 4 in Ariana Hospital, Tunisia. The follow-up period was the duration of the chemotherapy course.
We included all NSCLC patients in stage IV of the disease according to the 8th edition of TNM classification, during an inclusion period from January to December 2018.
Inclusion criteria: Confirmed NSCLC with histological proof, stage IV of the disease, prescription of a palliative chemotherapy course, written informed consent to receive chemotherapy course and written informed consent to participate in the study.
Non-inclusion criteria: patients on medication who had interfered with the cycle or quality of sleep, and patients in need of morphine treatment, patients with an unbalanced chronic disabling disease that affects quality of life.
Exclusion criteria: Withdrawal of consent, non adherence of the patient to chemotherapy whatever was the reason, patients who had not completed the chemotherapy protocol, onset during follow-up of a synchronous tumor.
Clinical data were collected at the end of the last chemotherapy course. Then, questionnaires offered to our patients assessed the quality of life, the quality of sleep and quality of humor (respectively QLQ C-30, PSQI and HADS questionnaires in an Arabic Tunisian version):
The QLQ C-30 questionnaire included thirty forced-choice questions, classified as follows:
i. Symptom items (9 items, 13 questions): Fatigue, nausea and vomiting, pain, dyspnea, insomnia, anorexia, constipation, diarrhea, and financial difficulties
ii. Functional items (5 items, 15 questions): Physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning
iii. Global health item (1 item, 2 question)
The Pittsburgh Sleep Quality Index (PSQI) contains nineteen questions assessing seven dimensions of sleep disturbance patterns: global subjective quality of sleep-sleep latency-sleep duration-sleeping efficiency-sleep and wake disturbances-use of sleep medication-daytime dysfunction or sleepiness [14]. Every dimension is evaluated from 0 to 3 according to the patient's answers. The score reflects the disturbance severity. The seven dimensions scores were combined to give a global score ranging from 0 to 21. Greater scores indicate poorer sleep quality. When the PSQI score is greater than 5, sleep quality is considered as poor. The PSQI was validated for cancer patients [15]. We used an Arabic Tunisian dialectal version of PSQI.
Hospital Anxiety and Depression Scale (HADS) is a fourteen item questionnaire: Seven items relate to anxiety and seven others relate to depression. Each item on the questionnaire is scored from 0 to 3; totals of items scores provide us anxiety and depression scores.
Patients were put on chemotherapy validated by a pluri-disciplinary medical team. Patients had got one of the three chemotherapy regimen usually used: Cisplatin/Vinorelbin doublet, Cisplatin/Gemcitabine doublet and Carboplatin/Paclitaxel doublet. A subsequent follow-up of the disease was consistent with international recommendations for metastatic lung cancer [16,17]. RECIST 1.1 criteria were used to assess response to chemotherapy [18]. Patients were followed until death or until the point date of 31-12-2020.
We performed initially a descriptive statistical analysis to get frequencies, percentages, and mean socio-demographic and survival parameters. Quantitative and objective assessment of quality of life, quality of sleep and HAD score was provided. Then, we studied significant variability correlated to the therapeutic regimen, correlations between mean scores and anti-tumoral treatment (Student t-test, non parametric tests, Qui square test). The study was conducted then, to assess the correlation between quality of life indicators and the prognosis of stage IV NSCLC.
The study protocol was first, discussed in the hospital ethics committee. Then, the study was submitted in the Pan African Clinical Trial registry (PACTR): Study number PACTR202104725647601.
We enrolled 120 patients during the study. Exclusion criteria were decisive in 49 cases. We kept 71 cases in the data collecting step. The mean age of our patients was 62.17 years (42-85). All patients were smokers [56 pack-year at average]. Current smokers represented 34% of all patients. Most frequent past medical history were COPD (39%), arterial hypertension (30%) and diabetes (13%).
At their first consultation, 44 patients (62%) had a Performance Status (ECOG PS) better than 2.Mean delay from the 1st consultation to the histological confirmation on lung cancer was 21 days (min = 6 ; max = 41). The most common histological type was adenocarcinoma (58%). Using the TNM 8th edition, 27% of patients were in stage IVA; 34% in stage IVB and 39% in stage IVC of the disease. Sixty percent of patients received at least three cycles of palliative chemotherapy (Table 1). Brain radiation therapy was performed in 8 patients (brain metastases).
Table 1: Main characteristics of the cohort. View Table 1
Grade III or higher adverse events (requiring special treatment or a postponement in chemotherapy protocol) were noted in 35 patients (49%). Neutropenia, vomiting and anemia were the most common of the main adverse effects found (Table 1).
Tumours progressed after the first line of treatment in 42 patients (59%), 19 patients had tumour lesion stability (27%) and partial tumour regression was noted in 7 patients. An alteration in the general condition led to the discontinuation of chemotherapy for 3 patients (4%). At the end of our study, we had 14 survivors (20% of the cohort).
Twenty-six patients had a good response after 1st line treatment (37% of patients). Their average progression-free survival (PFS) was 194 days. PFS greater than 3 months was observed in 23 patients. The mean overall survival (OS) was 317 ± 20 days (95% confidence interval = 292-377) with extremes of 1.6 months to 21 months. The one-year survival rate was 44% (Figure 1).
 Figure 1: The survival curve of the cohort (Kaplan Meier curve displaying the estimated Survival Probability).
View Figure 1
Figure 1: The survival curve of the cohort (Kaplan Meier curve displaying the estimated Survival Probability).
View Figure 1
Patients had got one of the three chemotherapy regimen usually used: Cisplatin/Vinorelbin doublet, Cisplatin/Gemcitabine doublet and Carboplatin/Paclitaxel doublet. We found closely the same rates of response to treatment among the three groups of patients under chemotherapy (Figure 2, p = 0.33).
 Figure 2: Response to treatment among subgroups of patients under chemotherapy regimen.
View Figure 2
Figure 2: Response to treatment among subgroups of patients under chemotherapy regimen.
View Figure 2
Coefficient of symptoms: The dimensions "symptoms" most severely affected were financial difficulties, anorexia and dyspnea. Their mean scores were 50.23%, 42.72% and 38.5% respectively. Most cited symptoms in the questionnaire were fatigue, dyspnea and financial difficulties (reported by 83%, 76% and 73% of patients respectively). The mean score of the coefficient of symptoms was 26.56 (Table 2).
Table 2: QLQ-C30 dimensions and their mean scores. View Table 2
Coefficient of performances: At the end of chemotherapy, a limitation of capacity and performance was frequently found in our patients. The lowest mean score was 50, 7 and corresponded to "Limitation in Social Life" dimension and the most preserved mean score was equal to 69 and corresponded to "Limitation in Daily Life" dimension. The average performance score was 64.07.
Coefficient of global life: The mean score of this coefficient was 37.44 (min = 0; max = 83.3). We found a significant correlation with positive proportionality index between the global life coefficient and the performance coefficient. Furthermore, the symptom coefficient was significantly correlated with the global life coefficient with negative proportionality index meaning an inversely proportional link between them (Table 3).
Table 3: Correlations between mean scores of quality of life. View Table 3
Differences in mean scores of Qol among the three subgroups of patients receiving regimen of chemotherapy were minor and out of significance. Regimen of chemotherapy didn't interfere so, with the Qol in stage VI NSCLC patients (Table 4).
Table 4: Comparison of Qol scores among subgroups of patients receiving regimen of chemotherapy. View Table 4
Sleep quality questionnaire: analysis of the PSQI score: Analysis of the PSQI score at the end of chemotherapy showed that 55% of patients had a score ≤ 5 (good sleep quality). Insomnia was the most reported sleep disorder (85% of patients). An excessive daily sleepiness was noted in 52% of patients.
The PSQI score was correlated to the quality of life as shown in the Table 3.
HAD anxiety-depression questionnaire: Anxious humor was found in 21 patients (30%), a borderline anxious humor was found in 17 patients (24%) and a normal humor was found in 33 patients (46%). Patients with anxious humor had a significant degradation of global life coefficient score (p = 0.0005), performance coefficient score (p = 0.006) and a worsened symptoms coefficient score (p = 0.0009).
Depressive humor was found in 24 patients (34%), a borderline depressive humor was found in 14 patients (20%) and a normal score was found in 33 patients (46%). Patients with anxious humor had a significant degradation of global life coefficient score (p = 0.0001), performance coefficient score (p = 0.0024) and a worsened symptoms coefficient score (p = 0.0007).
Prognostic impact of epidemiological and clinical features: Statistical analysis had shown no correlation between OS and several features as age, tobacco consumption, clinical revealing symptoms, Body Mass Index or histological sub-type (Table 5).
Table 5: Correlation between clinical features and overall survival in stage VI CBNPC patients. View Table 5
OS was obviously longer for patients with a preserved PS when chemotherapy started.
Mean OS was closely correlated with tumour response after 1st line chemotherapy. In patients who had objective partial tumour regression, OS was 551 days and one-year survival rate was 85%. For patients who had tumor progression, OS was 265 days with a one-year survival rate of 28% (p = 0.0001).
Correlation between OS and quality of life: OS was correlated and proportional with the coefficient of global life and the coefficient of performances, which means a poor prognosis related to the degradation of quality of life, as perceived by the patient after chemotherapy (Table 3).
Considering performance dimensions each separately, a correlation was found between their mean scores and overall survival (Pearson's test). Considering the nine dimensions of symptoms separately, there was a significant inverse proportional correlation between OS on one side and the dimensions of "Fatigue", "Vomiting", "Insomnia" and "Anorexia" on the other side.
Correlation between OS and regimen of chemotherapy used: Statistical analysis had shown a closely comparable overall survival in our patients, whatever was the chemotherapy regimen used to treat the NSCLC (Table 6).
Table 6: Correlation between overall survival and chemotherapy molecules. View Table 6
Correlation between OS and sleep quality: Mean OS in patients with PSQI ≤ 5 scores was better than patients with PSQI scores > 5. The difference was significant (Figure 3; Log Rank test revealed an OS in good and poor sleepers equal to 441 days VS 219 days respectively; p 0.001).
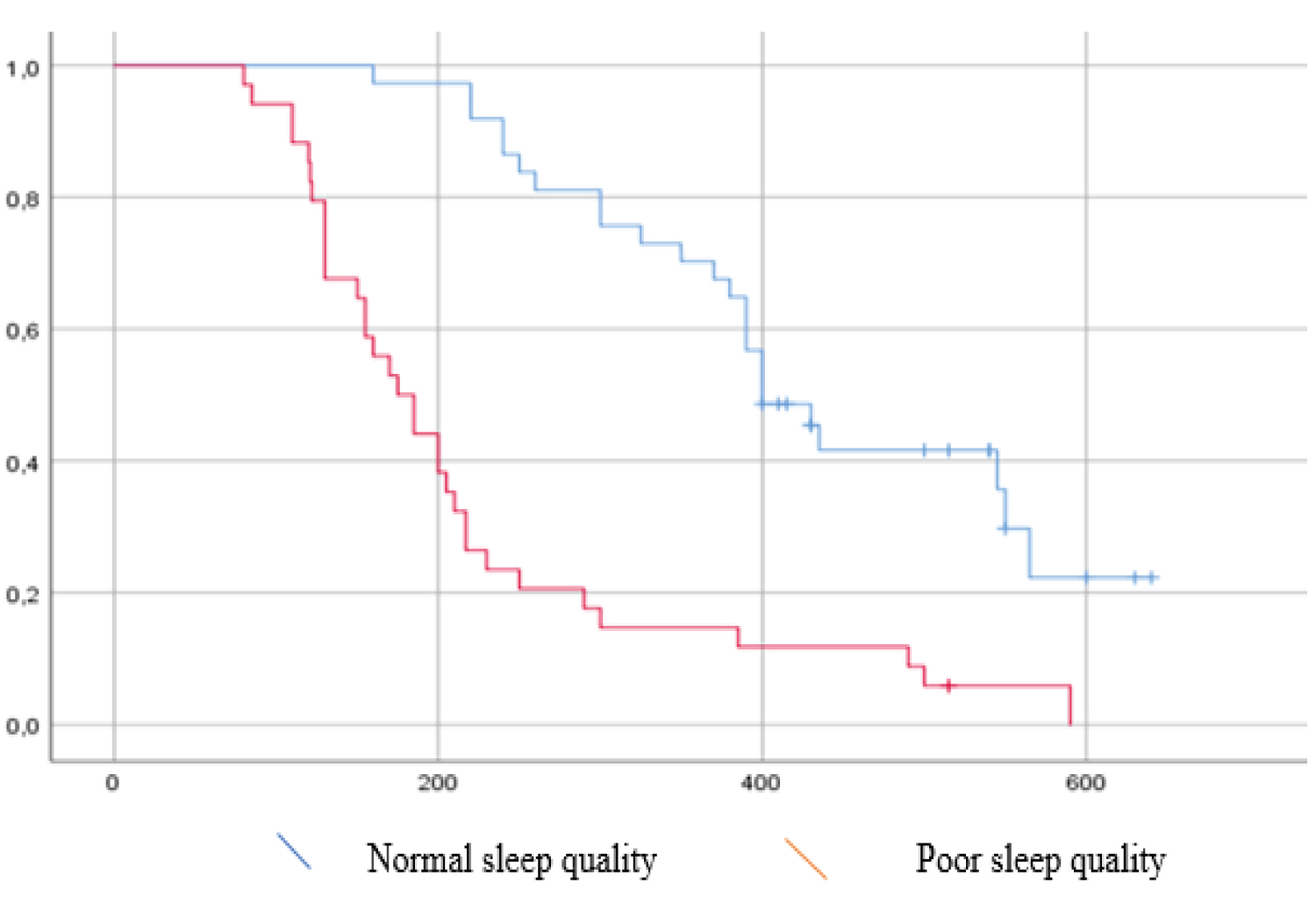 Figure 3: Kaplan-Meier curves displaying the estimated survival probability for Good and poor sleepers (Log Rank test).
View Figure 3
Figure 3: Kaplan-Meier curves displaying the estimated survival probability for Good and poor sleepers (Log Rank test).
View Figure 3
Correlation between OS and HAD scale: Patients with normal anxiety score had a significantly better mean OS than borderline or anxious humor patients (399 days, 280 days and 217 days respectively; p = 0.001). Also, patients with normal depression score had a significantly better mean OS than borderline or depressive humor patients (409 days, 371 days and 206 days respectively; p = 0.001).
Several key points distinguished our study and made its strength. Former studies about quality of life in NSCLC patients found a significant and sometimes unique correlation between pain intensity and quality of life in cancer patients or survivors after cancer treatment. Pain control during the treatment course with no need for morphine prescription was within the inclusion criteria in this study. These selection criteria helped to keep a consistent group of patients in whom the assessment of quality of life and sleep quality was not affected by pain or opioid treatment. By applying those exclusion criteria, the study has shown us correlations between various aspects of quality of life, which were hidden. Other publications were specifically insisting on pain intensity, self-consideration or body-image after a mutilating surgery [19-22].
Our study, however, may have some limitations. First, the number of people included was quite reduced. Second, the assessment of the complaints as well as the Qol was based on questionnaires. These are validated measuring tools with known standards to define the presence and the severity of a clinical abnormality. We used QLQ-C30 to assess Qol, PSQI questionnaire to assess sleep quality and HADS to screen humor disturbances [14,23,24]. To avoid the eventual lack of objectivity, some authors tried to couple them with other explorations. Some studies have used polysomnography in similar evaluation of sleep quality but they conducted their protocol on a cohort with small number [25-29]. Using Arabic Tunisian dialectal versions of the questionnaires already mentioned was beneficial. It allowed our patients to fill easily auto-questionnaires with answers with no interference of the investigators. Those versions were already pre-tested, reviewed and used in former studies in Tunisia [10,30,31]. Clarity and internal consistency are guaranteed. Comparison with English versions is still to get done, to prove the reliability of these newly produced questionnaires.
The enrolled patients were below the average age usually found for lung cancer, between the sixth and seventh decade most often. The explanation would be the inclusion criteria. However, our patients had multiple past medical diseases. Impact of the age on prognosis was widely discussed in the oncological field. Particular importance has been given to the concept of physiological age, closely linked to the prognosis according to several studies. We may say that there is no precise definition of the physiological age. It is usually described based on "some benchmarks" that describe the autonomy, general status and even psychological well being; which are dimensions classically assessed in Qol questionnaires and translated to scores.
Subjective weight loss (found in the interrogation) had a significant negative impact on OS in our patients. However, low BMI had not the same significance. Several studies have focused on the negative impact of weight loss on therapeutic management and the prognosis of lung cancer [32-35]. The recommendations of these authors emphasized the detection and prevention of weight loss during the exploration or treatment period, through a repeated assessment of the nutritional balance [36]. Weight loss is a sign of a decline in the nutritional balance. But given its subjectivity and its connection to the body image, generally harmed in our patients and their surrounds, this functional sign lacks precision. Topkan, et al. stressed the very negative psychological impact of weight loss during the treatment course [32]. It would therefore be more rational to look for an association of uncounted weight loss with the anxiety-depressive reaction or the adherence of patients to treatment protocols.
Belloumi, et al. had recruited 64 patients with stage III or IV NSCLC in 2018 [10]. The study involved the assessment of quality of life, quality of humor and sleep quality using the QLQ-C30, HADS and PSQI questionnaires. The analysis was performed before then after 4 cycles of chemotherapy. Sleep quality was deteriorated (45.3% of patients at the end of chemotherapy; mean PSQI = 5.4). Authors noted persistence of a poor sleep quality after treatment and sometimes a late onset complaint (during chemotherapy). In addition, the QLQ-C30 analysis showed increasing scores after chemotherapy concerning the dimensions of symptoms "Nausea" and "Insomnia". Also, physical and social performance dimensions were altered and showing decreasing scores. A strong positive correlation was found between sleep quality, psychological equilibrium and overall quality of life coefficient. An inversely proportional relationship was found between those variables and dimensions of symptom's scores.
Quality of life and psychological balance were also assessed before and after cognitive behavioural therapy in cancer patients. It was concluded that quality of life and sleep quality indexes improved at 8 weeks, 3 months, 6 months and 12 months of management. Therapists noted less use of hypnotizing drugs (fewer times and lesser doses) and a reduced rate of humor disorders. A recent meta-analysis highlighted the effectiveness of palliative management by the nurse "Nurse-led disease management" [37]. Seven randomized controlled studies were tabulated with a total of 1,110 patients. The nurses provided telephone follow-up, cognitive therapy, health education, family supervision and psychological support. The quality of life assessment was conducted using the QLQ-C30 questionnaire. Comparison of nurse-led and control groups showed significant differences in dimensions: Insomnia, constipation and financial difficulties. Those studies hadn't scout the prognostic impact of quality of life in cancer patients.
Studies of advanced cancer survivors reported a psychological improvement after one year of progression-free survival for gynecological cancers and lymphomas [38,39]. Berhili explained in part this result by the particularly religious background of the Moroccan society, analyzed in his study [38]. Religion has been described as the most widely adopted coping strategy to face-off the shock of the diagnosis and then to surpass the intensive treatment course. A study on a cohort of all cancer types found that religion was the major "coping" strategy in 86% of patients who felt they had become practicing more prayers after the disease [39].
The correlation between quality of life and sleep quality of NSCLC patients was analyzed in several studies [10,40,41]. In these studies, small samples of patients with stage II, III or IV lung cancer were recruited. Dean, et al. study found a correlation between the two parameters [40]. In this study of 29 patients, a confusion bias would be created by the effect of comorbidities and chief complaints. In Belloumi study, the sleep quality was degraded from the beginning to the end of the chemotherapy course, mean PSQI increased from 2.9 to 5.4 [10]. The quality of life (including performance dimensions and symptom dimensions) was deteriorated in the same way among good and bad "sleepers" [10]. The most affected symptoms dimensions after chemotherapy were: «Nausea» and «Insomnia».
The prognostic impact of an early introduction of palliative treatment for cancer patients was a hypothesis to verify. Palliative management was provided by a trained doctor and nurse, but involved almost systematically the intervention of the psychologist, nutritionist and physiotherapist at the slightest subjective degradation felt [42,43]. Paradoxically, the correlation of this personalized intervention with the average survival of patients with advanced cancers was not significant. On the other hand, palliative treatment prescribed "on-demand" significantly improved prognosis according to the multicentre study of the Early Palliative Care Italian Study Group [43,44]. Wide range publications including NSCLC patients at various stages suggested a statistically significant close link between quality of life and overall survival [45,46]. These studies reported degradation of overall survival correlated to scores of "Fatigue", "Nausea/Vomiting", "Insomnia" and "Diarrhea" dimensions assessed by QLQ-C30. At the end of chemotherapy course, a pejorative prognostic impact of the dimension "Fatigue" was still significant [45,46].
Des publications portant sur de larges séries de patients entre 2000 et 2010, ont suggéré un lien étroit statistiquement significatif entre le niveau de la qualité de vie et la survie globale [47,48]. Les patients inclus étaient porteurs de CNPC à des stades variés. Ces études ont fait part d'une dégradation de la survie globale proportionnelle aux scores des dimensions « Fatigue », « Nausées/Vomissement », « Insomnie » et « diarrhée » évalués lors du diagnostic de cancer [47]. Après la fin de traitement anti-cancéreux, La survie globale était inversement corrélée uniquement à la dimension « Fatigue » [47]. Les auteurs ont donc recommandé de mener des études dédiés à la recherche des variables ou des thérapeutiques promotrices de la qualité de vie surtout en absence de traitement curatif. The authors therefore recommended conducting studies dedicated to the search for therapeutics that promote quality of life, especially in the absence of curative treatment.
In our study, we found a statistically significant correlation between overall survival on the one hand and indicators of quality of life and sleep quality, which would give value to the various palliative treatments designed to promote quality of life. Many studies have discussed which factors promote quality of life among cancer survivors, increasingly investigated since the publication of the EORTC multicentre study [48]. The authors proposed physical activity, yoga sessions, psychological management, or treatments such as melatonin for insomnia [37,49-51]. Opinions concerning the role of alternative medicine remain controversial. These studies often include patients with neoplasms of good prognosis, after a good response to anti-tumoral treatment. There is a lack of specific studies for patients with advanced NSCLC.
Study data is available upon request to the corresponding author: nidhalbelloumi@gmail.com
The study was submitted in the Pan African Clinical Trial registry (PACTR): Study number PACTR202104725647601
Open access HTML and verified link of your registration number: https://pactr.samrc.ac.za/Search.aspx
No funding was used in this study.