Trismus in adults has a wide range of known causes, though few cases have ever been reported secondary to central pontine myelinolysis (CPM). This report describes a case of severe trismus without clear etiology successfully treated with onabotulinum toxin-A following development of CPM. Patient was a female aged in her early thirties who presented to the hospital with ascending weakness five days following hyponatremia correction at rates within guideline recommendations. MRI revealed increased signal in the central pons suggestive of CPM. Eighteen days later, she sustained tongue laceration after acute bilateral masseter hypertonic spasticity which was treated with chemo-denervation. Patient gradually regained the functional capacity to voluntarily open jaw for speech and mastication.
Central pontine myelinolysis, Locked-in syndrome, Trismus, Onabotulinum toxin A, Case report
Central pontine myelinolysis (CPM) is a disorder described by neuronal demyelination in the central pons, classically caused by the rapid correction of hyponatremia, advanced liver disease, or anorexia [1]. Clinical presentation is variable, but often rapidly leads to paraparesis or quadriparesis with high mortality and severe impairment in daily functioning secondary to residual neurological deficits in survivors [2]. Pseudobulbar symptoms have been described, such as dysarthria and dysphagia, but very few cases of trismus caused by CPM have been described in literature.
Trismus can be defined as jaw opening restricted to less than 35-40 mm, often self-limited and lasting less than two weeks, though rarely may become sustained over longer time periods. Mouth closure is mediated by a set of muscles innervated by the mandibular division of the fifth cranial (trigeminal) nerve, namely the masseter, temporalis, and pterygoid muscles. The motor nucleus of the trigeminal nerve continues to form a motor root at the level of the pons. This muscle group works in antagonism to those controlling jaw opening, with neural stimulation of one group simultaneously inhibiting the opposing muscle group. Treatment for trismus is aimed at the inciting etiology and may utilize heat therapy or muscle relaxants to alleviate symptoms in the acute phase [3].
We report a case of sustained trismus in a young female which developed following diagnosis of CPM after alcohol withdrawal and correction of hyponatremia at rates within recommended guidelines.
A 33-year-old Caucasian female with past medical history of untreated systemic and discoid lupus erythematous, alcohol abuse, alcoholic hepatitis, and polymyalgia was admitted to the inpatient medicine service secondary to a working diagnosis of central pontine myelinolysis. She originally presented 5 days prior to an outside hospital with alcohol withdrawal, vomiting, and hypokalemia with an admission serum sodium of 122. This was corrected per guideline adherence at a rate of 7 mEq over a period of 48 hours followed by 6 mEq over the next 24 hours. Patient discharged to home after treatment with normalized labs, no neurologic deficits, and complete functional independence at that time.
Five days after initial discharge, the patient was readmitted with ascending progressive weakness. On day one of her second admission, the patient on physical exam was alert and oriented, functionally capable of nodding her head yes or no, had full range of motion of her upper extremities with mildly reduced strength of 3/5, and notably in the lower extremities she had reduced strength 1/5 of her left foot and no movement in the right foot. By the second morning, she was alert but with sonorous respirations progressing to complete flaccid paralysis with aphasia. Brain MRI revealed restricted diffusion and FLAIR abnormality with increased signal in central pons and the superior medullary tectum with peripheral sparing suggesting osmotic myelinolysis syndrome (Figure 1).
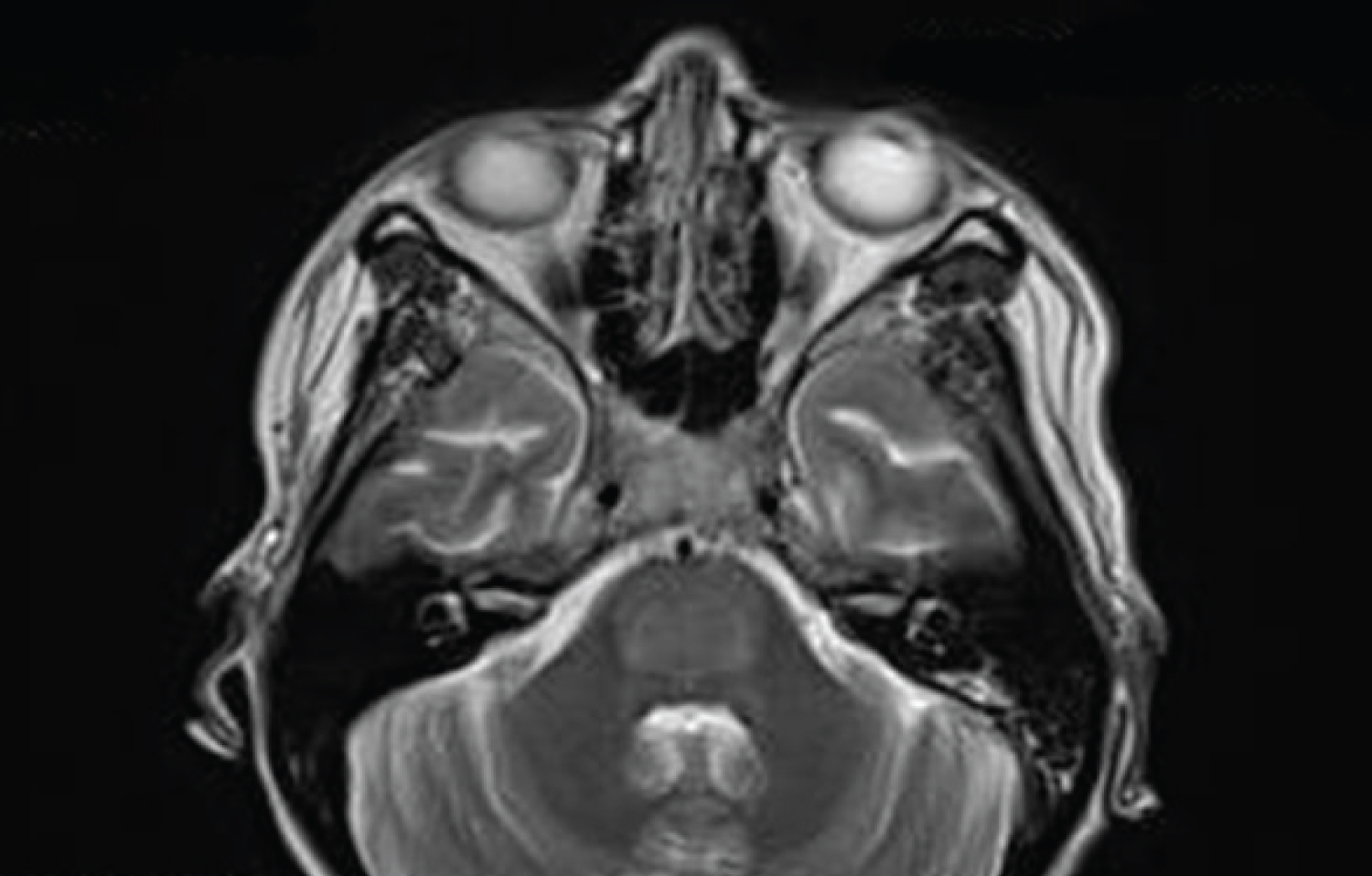 Figure 1: Brain MRI hyperintensity of pons sparing periphery and corticospinal tracts on axial T2-weighted image
View Figure 1
Figure 1: Brain MRI hyperintensity of pons sparing periphery and corticospinal tracts on axial T2-weighted image
View Figure 1
Full spinal MRIs showed some mild degenerative changes but nothing acute that could explain this patient's presentation. Electrolytes were within normal limits. Patient was transferred to another hospital for higher level care and further evaluation.
The Neurology service was consulted and recommended steroids and plasmapheresis before second transfer to higher level care hospital for second opinion. Upon transfer to our facility, four days after initially presenting with weakness, the patient was completely aphasic, tetraplegic with flaccid paralysis in all extremities, able to open her mouth only to yawn or cry and could only move her eyes vertically. Patient was admitted to the ICU for intubation secondary to respiratory failure. Neurology confirmed diagnosis of CPM, and she was treated with plasmapheresis and IVIG for total of five days, as well as IV steroids. She required tracheostomy and PEG tube placement.
Eighteen days following initial presentation with weakness, the patient developed acute, severe trismus causing tongue laceration and bleeding from the patient's tracheostomy and oral cavity requiring placement of bite block and transfer back to ICU for ventilatory management and laceration repair. Our PM&R team was consulted for evaluation and treatment. On physical examination, bilateral masseters were tense and contracted, right side slightly more than left. The patient's mouth could not be passively opened to provide needed oral and respiratory care. Due to the focal nature of her spasticity, we recommended a trial of chemo-denervation of the hypertonic masseters with botulinum toxin. After providing informed consent both to the patient and to her husband, we proceeded with chemo-denervation of the bilateral masseters using 50 units onabotulinum toxin-A to each masseter (100 units total) diluted 2:1 with normal saline and divided into three injection sites per side to try to relieve her trismus. The procedure was well-tolerated with no untoward effects noted directly after. Patient continued to sustain trismus accompanied by jaw pain in the days immediately following the procedure, but over a period of 3 weeks following the injections, serial physical exams demonstrated improved ability to open the jaw both passively and actively. Bite guard was removed, and the patient maintained the ability to yawn and cry reflexively with variable range of jaw motion but without voluntary opening. Four weeks post-procedure, the patient's speech therapist noted increased voluntary mouth opening to allow a spoon slightly between her teeth, a distance of several millimeters.
The patient gradually improved over several weeks and eventually regained sufficient oral motor control to smile, protrude her tongue, and purse her lips. She further regained sufficient strength to allow phonation and functional speech, and she was able to be advance to a pureed diet. She also began to regain strength in the upper extremities although the lower extremities remained flaccid. Nearly 11 weeks after therapeutic chemo-denervation of the bilateral masseters and over three months total after initial presentation with CPM, she was discharged to an acute inpatient rehabilitation facility for continued recovery.
Trismus is an upper motor neuron pathology resulting in hypertonic spasticity of masticatory muscles. The differential for trismus in adults is broad, including inflammatory, traumatic, odontogenic, neoplastic, neurogenic, psychogenic, or iatrogenic etiologies [4]. Cerebrovascular accidents are known culprits as well, although trismus following lesions in the brain stem is known to be a rarer complication than those in the cerebral hemisphere [5]. Usual treatment is conservative and directed at the cause of trismus except when symptoms interfere with patient care in the hospital or become severe enough to present an immediate threat to life.
This patient's development of bilateral spasticity of the masseters occurred less than three weeks after presenting with symptoms of CPM. Palpation of the pterygoid and temporalis muscles did not reveal obvious sustained contraction. Patient was a febrile prior to the event, electrolytes within normal limits, and had no other new neurologic changes (including any loss of sensation of the face) at the time nor prior procedures around the face or oral cavity. No inciting events nor prior imaging findings on further review explained this development. Marchiafava-Bignami disease and basilar artery thrombosis have been rare imaging findings described in association with development of trismus in context of CPM [6,7], as well as vertebrobasilar dolichoectasia [8], though neither conditions were apparent on head CT or brain MRI of this patient. She had no documented history of seizures or head injuries. In theory, it may be possible that regional inflammation and edema surrounding the pons secondary to myelinolysis, or less likely an otherwise subclinical microvascular stroke may have caused sufficient irritation to the trigeminal nerve to induce trismus. It is unclear why the mandibular branch was affected in isolation, especially within the context of CPM without other significant imaging findings. Of note, the patient did have a reported history of nocturnal bruxism and chronic anxiety, though their role in the prolonged duration and severity of her acute trismus remain questionable.
Onabotulinum toxin-A is indicated for treatment of spastic disorders, including trismus and TMD, with onset of effect 48-72 hours after administration, peak effect in 2-6 weeks, and greatest clinical efficacy of 2-3 months [9]. This treatment modality was chosen given severity of the case, the focal nature of her symptoms, the need for oral access to facilitate patient care, and to potentially help relieve pain caused by tonic spasm of the masticatory muscles. Chemo-denervation therapy for this unusual incident appears to have assisted in alleviating symptoms and improving functionality in speech, swallowing, and facial expression. The significance of this case report centers around the development of trismus in absence of distinctly attributable causation in the context of CPM.
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. Authors have no disclosures, funding sources, or competing interests.