We present a case of a 72-year-old male diagnosed with concurrent crystal-storing histiocytosis and nodal marginal zone lymphoma with plasmacytic differentiation following a finding of new axillary lymphadenopathy during active surveillance for an early stage lung cancer. A panel of ancillary studies was performed to help establish the diagnosis and to exclude other histologic mimics. We share this case to promote awareness of this rare entity, discuss its association with immunoglobulin-producing lymphomas and review an approach to cases with CSH to avoid misdiagnosis".
Crystal-storing histiocytosis, Nodal marginal zone lymphoma, Plasmocytic differentiation
CSH: Crystal-Storing Histiocytosis; NMZL: Nodal Marginal Zone Lymphoma; CT: Computed Tomography; PAS: Periodic Acid-Schiff
Crystal-storing histiocytosis (CSH) is a rare disorder in which crystallized material accumulates within the cytoplasm of histiocytes. Many authors have proposed that the crystallized material represents an intra-lysosomal accumulation of immunoglobulins [1,2], as most cases of CSH are associated with B-cell lymphomas with plasmacytic differentiation or plasma cell neoplasms [3-5]. In some cases, a dominant histiocytic component can obscure the underlying neoplasm, which can possibly lead to an error in diagnosis. Herein, we present a case of nodal marginal zone lymphoma (NMZL) with plasmacytic differentiation occurring in association with CSH in a 72-year-old made with incidental axillary lymphadenopathy. In this article, we also discuss our approach to ancillary testing in cases of CSH, which is essential for excluding a variety of its histologic mimics.
A 72-year-old male status post radical radiotherapy for an early stage lung cancer was found to have new axillary lymphadenopathy on a computed tomography (CT) scan during active surveillance. Serum electrophoresis showed no paraprotein. Serum-free light chains were within normal limits. A positron emission tomography scan showed no FDG avid bone marrow or splenic involvement.
A fine needle aspiration of a right axillary lymph node revealed a cellular sample showing a mixture of small and medium sized lymphoid cells, scattered plasmacytoid cells, eosinophils, and plenty of large polygonal shaped histiocytes with abundant finely granular cytoplasm. Immunophenotypic analysis by flow cytometry confirmed a monotypic (lambda restricted) mature B-cell neoplasm, which were CD5 and CD10 negative.
Histopathologic examination of the excised lymph node showed an effaced architecture with small sized atypical lymphocytic infiltrates, foci of micro-granulomas and sheets of histiocytes with abundant granular cytoplasm".
By immunohistochemistry, the small lymphoid tumour cells were positive for CD20, but lacked staining for CD5 and CD10 (Figure 1). Scattered plasma cells were also identified, which were monotypic for lambda light chains. The histiocytes were positive for CD68. PAS, PASD, and AFB were negative for storage disease and mycobacteria, respectively (Figure 2). Cytokeratin, S100, CD1a, CD30, SOX10, desmin, Factor XIIIa, and EBER-ISH were negative (Figure 3). PCR showed a negative result for a MYD L265P mutation.
 Figure 1: H&E (A, 1X) atypical small lymphoid infiltrate with foci of micro-granulomas (B, 100X) and sheets of histiocytes with abundant granular cytoplasm (C, 200X).
View Figure 1
Figure 1: H&E (A, 1X) atypical small lymphoid infiltrate with foci of micro-granulomas (B, 100X) and sheets of histiocytes with abundant granular cytoplasm (C, 200X).
View Figure 1
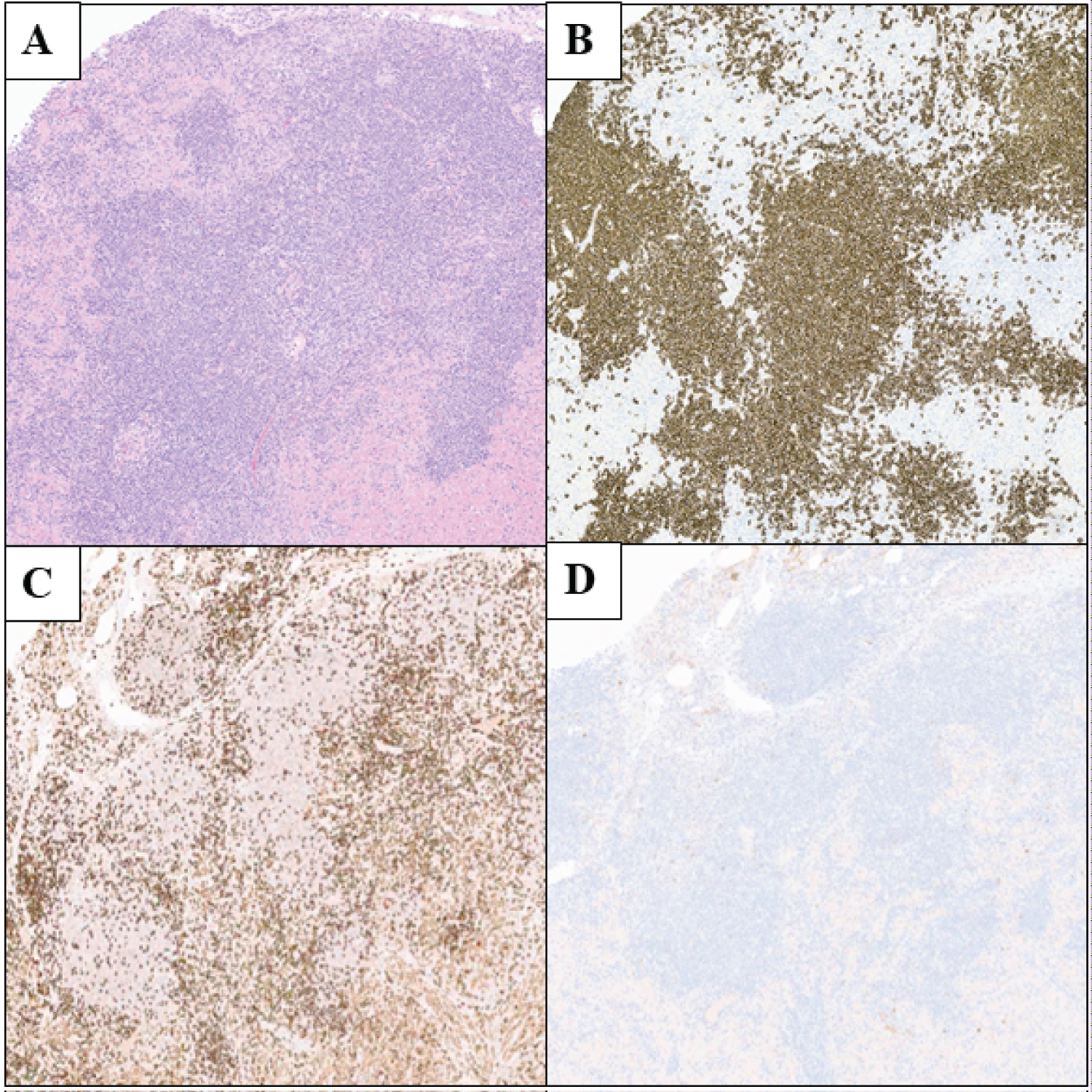 Figure 2: H&E of nodal marginal zone lymphoma (A, 40X) and select immunohistochemical stains.
Figure 2: H&E of nodal marginal zone lymphoma (A, 40X) and select immunohistochemical stains.
The atypical small lymphoid infiltrate stains positive for CD20 (B, 40X) but negative for CD5 (C, 40X) and CD10 (D, 40X).
View Figure 2
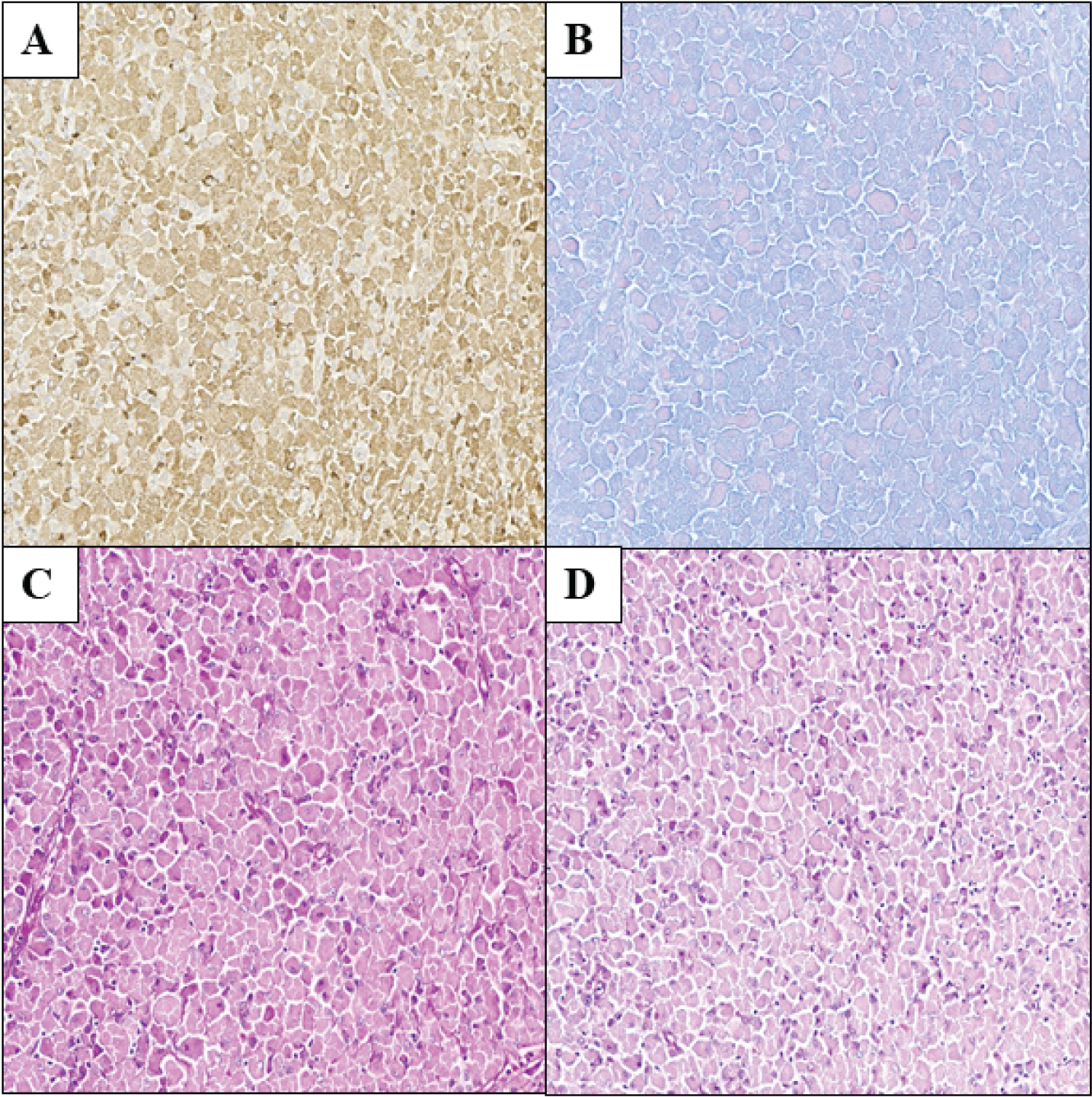 Figure 3: Crystal-storing histiocytosis showing positivity for CD68 (A, 100X). Special stains, including AFB (B, 100X), PAS (C, 100X) and PASD (D, 100X), were negative.
View Figure 3
Figure 3: Crystal-storing histiocytosis showing positivity for CD68 (A, 100X). Special stains, including AFB (B, 100X), PAS (C, 100X) and PASD (D, 100X), were negative.
View Figure 3
A diagnosis of a NMZL with plasmocytic differentiation and CSH was made. The patient is followed by hematology, where he continues to be asymptomatic from his lymphoma.
Accumulation of crystallized immunoglobin molecules within the cytoplasm of histiocytes may be seen in B-cell lymphomas with plasmocytic differentiation and plasma cell neoplasms [1-3]. While the molecular basis has not been established, it is conceivable that stored immunoglobulins have acquired abnormal crystallization characteristics and/or have undergone intra-lysosomal degradation [4-6].
In our case, the presence of micro-granulomas and bilateral lymphadenopathy raised the possibility of infection as an etiology. However, AFB and stains for fungi were negative. Other entities with granular cytoplasmic inclusions were considered, including lysosomal storage disorders. Periodic acid-schiff (PAS) stains performed in our case failed to highlight any PAS-positive diastase resistant inclusions. Immunostains did confirm the presence of CD68 positive histiocytes and hence, various histiocytic lesions were also considered in the differential diagnosis. The histiocytes in our case, however, lacked the characteristic nuclear grooves seen in Langerhans cell histiocytosis and were negative for CD1a (Figure 4). Sinus histiocytosis with massive lymphadenopathy and xanthogranuloma were also excluded based on the lack of immunoreactivity with S100 and Factor XIIIa, respectively. Although granular cell tumor and adult type rhabdomyoma share overlapping morphologic features with CSH, lymph node involvement would be uncommon in these two neoplasms. Regardless, we excluded both granular cell tumor and adult type rhabdomyoma by demonstrating a lack of immunoreactivity to SOX10 and Desmin, respectively.
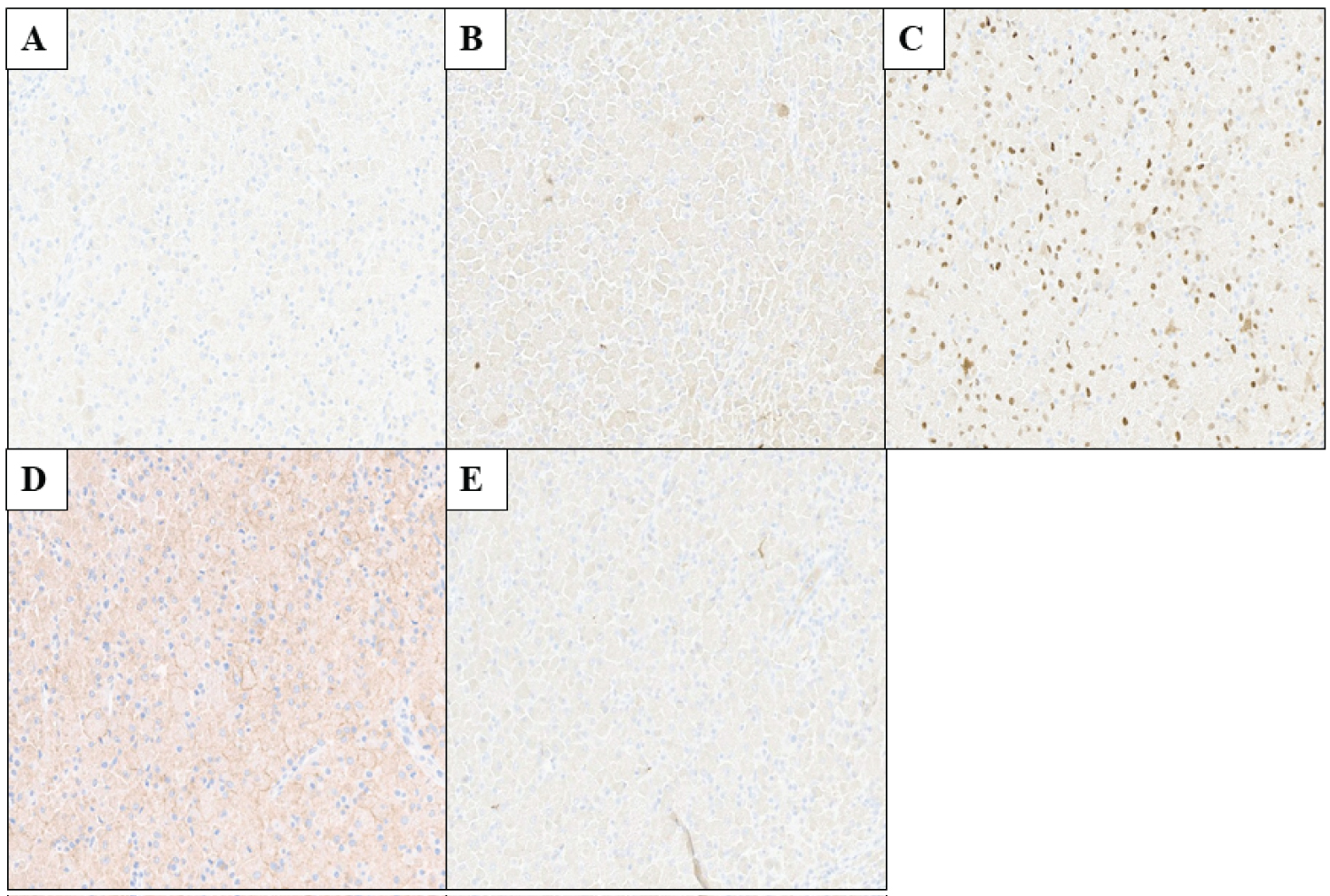 Figure 4: Sheets of histiocytes with granular cytoplasm are negative for CD1a (A, 100X), S100 (B, 100X), factor XIIIa (C, 100X), SOX10 (D, 100X) and desmin (E, 100X).
View Figure 4
Figure 4: Sheets of histiocytes with granular cytoplasm are negative for CD1a (A, 100X), S100 (B, 100X), factor XIIIa (C, 100X), SOX10 (D, 100X) and desmin (E, 100X).
View Figure 4
We also emphasize the observation that tissues with extensive histiocytosis may obscure an underlying lymphoid neoplasm. An awareness of this association is therefore crucial to avoid such misdiagnosis. The present case adds to the few reports in the literature of CSH associated with a NMZL and highlights the importance of having a high degree of awareness of this rare entity.
Authors declare that there are no conflicts of interest regarding the publication of this paper.